

Abstract
Introduction:
Osteochondromas are common benign bone tumours. They are usually seen in metaphyses of long bones and are seldom found in flat bones like scapula. When present in scapula, they may cause abnormal scapulothoracic movements leading to pain, snapping and winging of scapula.
Case Report:
We describe the case of a middle-aged woman with painful snapping and pseudo-winging of scapula due to a large osteochondroma. The patient was treated with open resection with relief of symptoms.
Conclusion:
Pseudo-winging and snapping scapula can be rarely caused by scapular osteochondromas even in cases presenting in fourth decade. These lesion respond well to surgical excision.
Keywords: Osteochondroma, Snapping Scapula, Pseudo-winging Scapula
Introduction
Osteochondromas constitute 10-15% of all bone tumours and 30-50% of benign bone tumours, representing the most common benign bone tumours [1,3]. They are usually solitary tumours, but can be multiple in hereditary exostoses. Though considered as a tumour, an osteochondroma is actually a developmental physeal growth defect. This defect usually occurs in the metaphysis of long bones like femur, humerus and tibia. It is unusual in scapula [4-7], seen only in 4% cases [8]. It usually presents as an asymptomatic slowly-growing mass, but may produce symptoms as a result of an overlying bursa[2,3,8,9], soft tissue impingement[10], a fracture of the stalk[11], a vascular injury[12,13], a neurological injury[14] and malignant transformation. Snapping scapula is an uncommon disorder resulting from derangement of the scapula-costal mechanism. The etiology is usually idiopathic. However, an anatomical cause like osteochondroma may lead to snapping scapula; in such cases excision of the tumour is required to obtain normal scapulothoracic motion [15].
This report describes a case with a large scapular osteochondroma causing pseudo-winging and snapping scapula syndrome and treated with excision.
Case Report
A 34-year old right-hand dominant female presented with tolerable pain in upper back associated with “clunking” during active movements of right shoulder. The patient also noticed a mass in the scapular region. Symptoms developed gradually over a six month period following trauma.
Physical examination revealed a non-tender palpable mass at superior angle of scapula. Marked crepitus, both palpable and audible, was produced during active shoulder range of motion. Winging of scapula was noticed (Fig. 1a). The upper extremity and shoulder girdle muscles were neurologically intact. Laboratory investigations were within normal limits.
Fig 1.
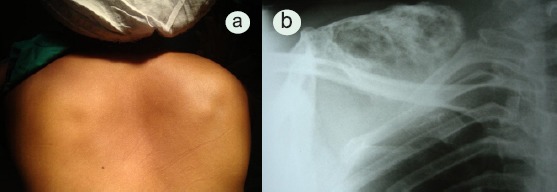
a-Photograph of the patient shows prominent medial border of right scapula (Pseudo-winging). b- AP scapular radiograph showing osteochondroma arising form scapula.
Radiographs showed a large bony tumour arising from superior angle of scapula towards the thorax (Fig. 1b). Computed tomography scan images revealed a pedunculated osteochondroma measuring 6.2x5.0 cm attached to ventral surface of superior angle of scapula by a small stalk. Similar but smaller sessile and pedunculated lesions were also seen involving the body of the scapula as well as the upper shaft of right humerus (Fig. 2a-b).
Figure 2.
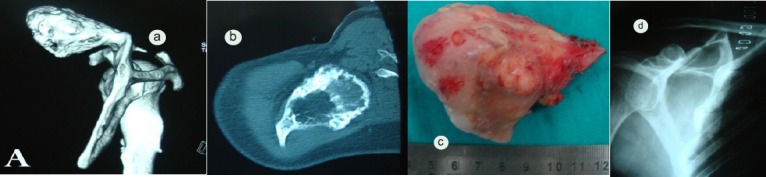
a-A CT scan of right shoulder joint shows a large pedunculated lytic bony lesion originating from the medial aspect of the superior margin of right scapula. The mass measures 6.2×5.0 cm in size. The tumour shows speculated sclerosed margins with no cortical break. Similar but smaller lesions are also seen involving the upper shaft of right humerus. b-Axial CT image of the lesion. c- A photograph showing the measurement of the tumour. Gross examination of the excised tumour shows irregular surface along with its stalk with characteristic bluish gray cap of cartilage. d- final radiograph confirming complete removal of tumor.
The patient was treated with excision of osteochondroma in prone position under general anesthesia. No bursa was demonstrated (Fig. 2c) and we encountered no technical difficulties during surgery. Histopathological examination confirmed the mass to be an osteochondroma. No malignant transformation was noticed in the cartilaginous cap. Post-operative clinical examination showed painless and full shoulder mobility as well as absence of scapular winging and crepitus. Radiograph confirmed complete removal of the tumor (Fig. 2d). There was no recurrence of symptoms at one year follow up
Discussion
The snapping scapula syndrome was first described by Boinet in 1867. Since then, case reports of painful snapping scapula due to scapular osteochondroma have been infrequent [16-19]. The syndrome presents with pain in back and around the shoulder girdle associated with audible and/or palpable crepitus of scapula on scapulocostal movements. Milch[17] described this crepitus as a tactile-acoustic phenomenon secondary to an abnormality between the anterior surface of the scapula and the thoracic wall. Milch[17] also reported that Mauclaire divided the sounds into three classes- Froissement or gentle friction sound, Frottement or somewhat louder sound and Craquement or loud snapping sound. According to Milch, the second category is the commonest.
The diverse etiology of the snapping scapula syndrome includes anomalies of bone, muscles or bursae[17]. Carlson et al [16] in a review of 89 cases of snapping scapula syndrome reported skeletal abnormalities in 11 cases. 27 cases were idiopathic and osteochondromas were seen in 3 cases.
Mechanism of snapping can be explained by the study of local anatomy. Normally, the serratus anterior and subscapularis muscle cushion the anterior surface of scapula assisting the gliding of scapula over the thoracic wall [16, 6]. However, there is little cushion over the superior and inferior angles and the medial border. Thus, osteochondromas in these locations can lead to snapping. The repeated friction between the tumour and the chest wall may lead to formation of a bursa [2,20]. No bursa, however, could be demonstrated in our case.
Scapular osteochondroma causes snapping usually in adolescence or early adulthood [18]. However in our case, the patient presented in fourth decade. Trauma, as in our case, might precipitate the symptoms[7,19]. Winging of scapula is a described feature of scapular osteochondroma[2,18]. This “pseudo-winging” is indicative of a subscapular mass with neurologically intact serratus anterior[2].
Snapping scapula caused by soft tissue abnormality may be treated conservatively. However, when a bony abnormality like osteochondroma has been detected, surgical intervention is required. Carlson[16] reported that 52%(12 out of 23) patients with idiopathic type had relief of symptoms with conservative therapy, while no patient(0 out of 4) with skeletal abnormality had relief with conservative line of management. Surgical resection of osteochondroma leads to relief of symptoms as illustrated by our case.
Table 1.
Literature Review of Case Reports of Snapping Scapula
| Author | Year | No. of Patients | resenting Complaints | Management | Results |
|---|---|---|---|---|---|
| Dobelle et al (4) | 1939 | 1 | Grating sound without pain | Surgical resection | Resolution of symptoms |
| Milch (17) | 1950 | 4 | Pain, crepitations, swelling; one case presented with grating with winging of scapula but no pain | All underwent surgical resection | Resolution of symptoms |
| Parsons (18) | 1973 | 5 | Pain, swelling, discomfort and crepitations; one had winging of scapula | 4 patients underwent surgical excision; one patient declined surgery | Resolution of symptoms in those who underwent surgery |
| Strizak et al (19) | 1982 | 1 | Pain with audible and palpable grating | Surgical excision | Resolution of symptoms |
| Carlson et al (16) | 1997 | 3 | Pain and clicking noise | 2 treated surgically and 1 non-surgically | Out of surgically treated patients one had relief while other had partial relief. The third patient had no significant change in symptoms |
| Okada K et al (3) | 1999 | 1 | Pain, crepitation with snapping | Surgical excision | Resolution of symptoms |
| Mohsen et al (2) | 2006 | 1 | Pain, swelling with winging of scapula | Surgical resection | Resolution of symptoms |
| Riet et al (5) | 2007 | 1 | Painful crepitus with pseudowinging of scapula | Arthroscopic resection | Resolution of symptoms |
| Fukunaga S et al (21) | 2007 | 1 | Pain with clunking but no winging | Endoscopic removal of tumour | Resolution of symptoms |
| Yoo et al (9) | 2008 | 1 | Swelling | Surgical excision | Resolution of symptoms |
| Aalderink et al (6) | 2010 | 1 | Pain with winging | Arthroscopic resection | Resolution of symptoms |
Successful arthroscopic resection of a subscapular osteochondroma has also been described [5,6]. Incomplete removal, however, may lead to recurrence.
Conclusion
To conclude, snapping scapula syndrome is a disorder caused by abnormal scapulothoracic motion of variable etiology. This syndrome may be a clinical manifestation of a subscapular osteochondroma with or without history of trauma. Surgical resection of the tumour is a reliable treatment which results in resolution of the crepitus and pain.
Clinical Message.
Snapping scapula is a syndrome of variable etiology. It is important to differentiate between idiopathic and anatomical causes as conservative treatment is less likely to be successful if a clear anatomical cause can be found.
Acknowledgements
Auther will like to thank Dr Ketan Khurjekar for his guidance and Dr Ashok Shyam for providing reference articles for preparing this case report.
Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Pongkripetch M. Sirikulchayanonta V:Analysis of bone tumors in Ramathibodi Hospital, Thailand, during 1977-1986: study of 652 cases. J Med Assoc Thai. 1989;72:621–628. [PubMed] [Google Scholar]
- 2.Mohsen MS, Moosa NK, Kumar P. Osteochondroma of the scapula associated with winging and large bursa formation. Med Prin Pract. 2006;15:387–390. doi: 10.1159/000094275. [DOI] [PubMed] [Google Scholar]
- 3.Okada K, Terada K, Sashi R, Hoshi N. Large bursa formation associated with osteochondroma of the scapula:a case report and review of the literature. Jpn J Clin Oncol. 1999;29(7):356–360. doi: 10.1093/jjco/29.7.356. [DOI] [PubMed] [Google Scholar]
- 4.Dobelle M. An unusual location of an osteochondroma:Report of a case. J Bone Joint Surg Am. 1939;21:781–784. [Google Scholar]
- 5.Reit RP, Glabbeek FV. Arthroscopic resection of a symptomatic snapping subscapular osteochondroma. Acta Orthop Belg. 2007;73:252–254. [PubMed] [Google Scholar]
- 6.Aalderink K, Wolf B. Scapular osteochondroma treated with arthroscopic excision using prone positioning. Am J Orthop. 2010;39(2):E11–E14. [PubMed] [Google Scholar]
- 7.Tomo H, Ito Y, Aono M, Takoaka K. Chest-wall deformity associated with osteochondroma of the scapula:A case report and review of the literature. J Shoulder Elbow Surgery. 2005;14:103–106. doi: 10.1016/j.jse.2004.03.007. [DOI] [PubMed] [Google Scholar]
- 8.El-Khoury GY, Bassett GS. Symptomatic bursa formation with osteochondromas. Am J Roentgenol. 1979 Nov;133:895–898. doi: 10.2214/ajr.133.5.895. [DOI] [PubMed] [Google Scholar]
- 9.Yoo W, Kim JR, Jang KY, Lee SY, Park JH. Rapidly developed huge bursitis associated with scapular osteochondroma of the multiple exostosis:a case report. Rheumatol Int. 2009;29:317–319. doi: 10.1007/s00296-008-0659-8. [DOI] [PubMed] [Google Scholar]
- 10.Ogawa K, Yoshida A, Ui M. Symptomatic osteochondroma of the clavicle. A report of two cases. JBone Joint Surg Am. 1999;81:404–408. doi: 10.2106/00004623-199903000-00014. [DOI] [PubMed] [Google Scholar]
- 11.Prakash U, Court-Brown CM. Fracture through an osteochondroma. Injury. 1996;27(5):357–358. doi: 10.1016/0020-1383(96)00015-0. [DOI] [PubMed] [Google Scholar]
- 12.Greenway G, Resnick D, Bookstein JJ. Popliteal pseudoaneurysm as a complication of an adjacent osteochondroma:angiographic diagnosis. Am J Roentgenol. Feb. 1979;132:294–296. doi: 10.2214/ajr.132.2.294. [DOI] [PubMed] [Google Scholar]
- 13.Hershey SL, Lansden FT. Osteochondromas as a cause of false popliteal aneurysms:Review of the literature and report of two cases. J Bone Joint Surg Am. 1972;54:1765–1768. [PubMed] [Google Scholar]
- 14.Twersky J, Kassner EG, Tenner MS, Camera A. Vertebral and costal ostoechondromas causing spinal cord compression. Am J Roentgenol. 1975;124:124–128. doi: 10.2214/ajr.124.1.124. [DOI] [PubMed] [Google Scholar]
- 15.Poppen NK, Walker PS. Normal and abnormal motion of the shoulder. J Bone Joint Surg Am. 1976;58:195–201. [PubMed] [Google Scholar]
- 16.Carlson HL, Haig AJ, Stewart DC. Snapping scapula syndrome:Three case reports and analysis of the literature. Arch Phys Med Rehabil. 1997 May;78:506–511. doi: 10.1016/s0003-9993(97)90165-9. [DOI] [PubMed] [Google Scholar]
- 17.Milch H. Partial scapulectomy for snapping of the scapula. J Bone Joint Surg Am. 1950;32:561–566. [PubMed] [Google Scholar]
- 18.Parsons TA. The snapping scapula and subscapular exostoses. JBone Joint Surg Am. 1973 May;55B:345–349. [PubMed] [Google Scholar]
- 19.Strizak AM, Cowen MH. The snapping scapula syndrome. A case report. J Bone Joint Surg Am. 1982 Jul;64:941–942. [PubMed] [Google Scholar]
- 20.Wright JM, Matayoshi E, Goldstein AP. Bursal osteochondromatosis overlyong an osteochondroma of a rib. J Bone Joint Surg Am. 1997;79:1085–88. doi: 10.2106/00004623-199707000-00018. [DOI] [PubMed] [Google Scholar]
- 21.Fukunaga S, Futani H, Yoshiya S. Endoscopically assisted resection of a scapular osteochondroma causing snapping scapula syndrome. World J Surg Oncol. 2007;5:37. doi: 10.1186/1477-7819-5-37. [DOI] [PMC free article] [PubMed] [Google Scholar]