

Abstract
Introduction:
Intrapelvic complications resulting from total hip arthroplasty are rare. Intrapelvic migration of the acetabular cup along with proximal migration of the femoral stem is one of these entities. Despite being a rare entity, there are serious complications.
Case Report:
We report a case image of an elderly lady who presented 6 months after total hip arthroplasty to her general practitioner and gynaecologist complaining of a palpable hard pelvic mass as well as difficulty walking. This proved to be the result of protrusio acetabuli prosthetica. This was reconstructed using saddle prosthesis.
Conclusion:
Protrusio Acetabuli Prosthetica can present as pelvic mass without any other associated symtoms. Although a rare complication, with noted morbidity, it might still be reconstructable.
Keywords: Total hip arthroplasty (THA), acetabular cup, intrapelvic migration
Introduction
Intrapelvic complications of total hip arthroplasty (THA) are not well understood, and most are secondary to intrapelvic migration of the acetabular component [1]. Although a rare condition, it has serious complications [2]. Intrapelvic migration of the acetabular component after total hip replacement, where there is severe acetabular destruction making reconstruction very difficult as was the case with our patient, is a very rare entity [3].
Case Report
A 73-year-old female presented to her general practitioner with a complaint of difficulty with walking, and an inability to weight bear on her right side. She also complained of pelvic pain, and had noticed an abdominal mass centrally and on her right side. There was no history of vaginal bleeding, discharge or a change in bowel habits. The general practitioner suspected a possible gynaecological cause for her presentation, most likely fibroid uterus, and subsequently referred her to a gynaecologist for further work up. She also had a history of five previous hip replacement operations for severe osteoarthritis of her hip joints, three on her right and two on her left side. Her last surgery was for her 3rd right hip total arthroplasty. This last total hip replacement surgery was performed in a teaching hospital setting. There were postoperative complications, most significantly a cold right lower limb. For this she had undergone successful endovascular stenting of her right external iliac artery and was discharged home. Her current presentation was 6 months after the last surgery. Gynaecological examination revealed a firm non-tender right iliac fossa mass. Vaginal examination revealed mobile masses protruding into the pouch of Douglas. Ultrasound examination of the pelvis demonstrated extensive acoustic shadowing. A working diagnosis of possible retained swab with a granulomatous mass was entertained. Having now suspected a non-gynaecological aetiolgy for her presentation, plain film radiographs were requested.
Supine pelvis and lateral hip radiographs (Fig.1a,b) demonstrated superior migration of the femoral head component of the prosthesis into the right side of the pelvis as well as a dislocated acetabular component lying in the mid lower pelvis. On lateral view the dislocated acetabular component was situated in the region of the pouch of Douglas with its screws directed inferiorly.
Figure (1a and b).
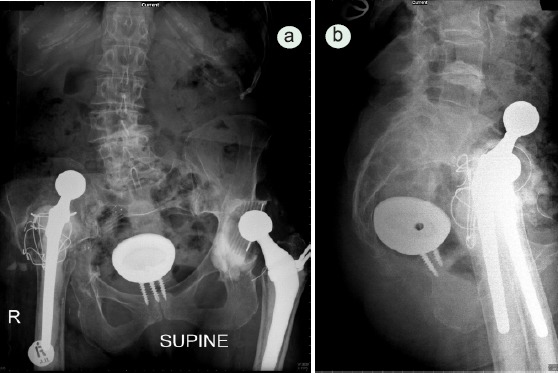
Supine pelvis (a) and lateral hip (b) radiographs demonstrate superior migration of the femoral head component of the prosthesis into the right side of the pelvis as well as a dislocated acetabular component lying in the mid lower pelvis.
The patient was transferred to a teaching orthopaedic unit where she underwent emergency surgery for removal of the intrapelvic acetabular cup. It was postulated by the surgeons that her multiple revision surgeries and osteoporotic bone state predisposed her to protruso acetabuli prosthetica. Her surgery involved a laparotomy with a transperitoneal approach. In view of the extensive destruction of the acetabular bone salvage was done using a saddle prosthesis and a total femoral replacement. This was done at a different institute and thus a follow up radiograph was not available
Discussion
Protrusio acetabuli prosthetica refers to failure of hip replacement surgery when there is intrapelvic migration of components. Predisposition to protrusio acetabuli prosthetica includes: over-reaming, multiple pelvic perforations, osteopenia, infection, trauma, diseases of bone deficiency, overactivity, or formation of a hypertrophic membrane [3]. In cases of osteoporosis and where acetabular rim support is inadequate the use of a reconstruction cage has been favourable in revision total hip arthroplasty[4]. The 2007 paper by Stiehl reported 17 previous such cases and they described three additional cases [5]. Since then we could find 5 more articles in pubmed [6-10]. The clinical picture in protruso acetabuli prosthetica include pain and visceral complications. Other complications reported include vascular injury, haematoma, nerve palsy, fistula from the hip to the intrapelvic viscera, compression of the bladder, ureters and vagina and clinical features of dyspareunia and gross haematuria [5]. In our case patient had peculiar history of palpable abdominal mass with pelvic pain and symtoms of right hip. Such high degree of migration of the femoral stem is uncommon especially with cemented stem that has not loosened from the medullary canal. Another peculiarity of these cases is female preponderance [5] which might be because of higher incidence and severity of osteoporosis in post-menopausal females. A treatment trend for such complications was mostly girdlestone excision arthroplasty however recent reports do favor use of saddle prosthesis or other reconstructions [5]. Long term follow up will be needed to recommend for or against any treatment protocol.
Conclusion
Our patient presented with two masses without haematuria or vaginal bleeding. Even though presentation was to a gynaecologist (via a general practitioner), use of multiple imaging techniques allowed for early management and prevented further complications.
Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Tomak Y, Birol G, Malazgirt Z, Karaismailoglu TN. Severe pelvic pain and extrinsic compression of the rectum:late complication of total hip arthroplasty. Journal of Orthopaedic Science. 2001;6:282–285. doi: 10.1007/s007760100048. [DOI] [PubMed] [Google Scholar]
- 2.Girard J, Blairon A, Wavreille G, Migaud H. Revue de Chirurgie Orthopedique et Traumatologique. 2011;97:181–190. [Google Scholar]
- 3.Morley DC, Schmidt RH. Protrusio Acetabuli Prosthetica. Orthopaedic Review. 1986;3:135–141. [PubMed] [Google Scholar]
- 4.Ries MD. Total Hip Arthroplasty in Acetabular Protrusio. Orthopaedics. 2009;32(9):666. doi: 10.3928/01477447-20090728-12. [DOI] [PubMed] [Google Scholar]
- 5.Stiehl JB. Acetabular prosthetic protrusion and sepsis:case report and review of the literature. J Arthroplasty. 2007 Feb;22(2):283–8. doi: 10.1016/j.arth.2006.02.170. [DOI] [PubMed] [Google Scholar]
- 6.Sarasin SM, Karthikeyan R, Skinner P, Nassef A, Stockley I. Transperitoneal removal of an intrapelvic acetabular component after total hip replacement and salvage of a destroyed acetabulum. J Bone Joint Surg Br. 2011 Jun;93(6):844–6. doi: 10.1302/0301-620X.93B6.26323. [DOI] [PubMed] [Google Scholar]
- 7.Girard J, Blairon A, Wavreille G, Migaud H, Senneville E. Total hip arthroplasty revision in case of intra-pelvic cup migration:Designing a surgical strategy. Orthop Traumatol SurgRes. 2011 Mar 1; doi: 10.1016/j.otsr.2010.10.003. [DOI] [PubMed] [Google Scholar]
- 8.Ahmad MA, Biant LC, Tayar R, Thomas PR, Field RE. A manoeuvre to facilitate acetabular component retrieval following intra-pelvic migration. Hip Int. 2009Apr-Jun;19(2):157–9. doi: 10.1177/112070000901900215. [DOI] [PubMed] [Google Scholar]
- 9.Foster S, Chaudhary H, Assenmacher B. Intrapelvic cementless component extraction with immediate triflange acetabular reconstruction using the retroperitoneal approach. J Arthroplasty. 2009 Feb;24(2):323ne1–5. doi: 10.1016/j.arth.2008.04.024. [DOI] [PubMed] [Google Scholar]
- 10.Yagdi S, Kazimoglu C, Dirim B, Bulut T, Sener M. Retroperitoneal migration of a septically loose femoral component. J Arthroplasty. 2011 Sep;26(6):977e17–20. doi: 10.1016/j.arth.2010.04.035. [DOI] [PubMed] [Google Scholar]