
Figure 2. Interpersonal Fear Avoidance Model of Pain (IFAM).
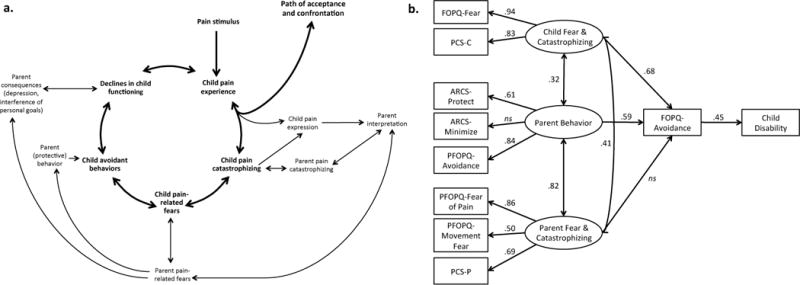
a. In the IFAM model, a child or adolescent develops pain, often in response to an event; although, it can also begin spontaneously. In the context of the child’s pain experience, (s)he either responds with progressive confrontation and acceptance of pain in his/her life for now or continues to perceive the presence of pain as threatening. This expression of threat and fear is observed and interpreted by the parent and reciprocally interacts with a parent’s own catastrophic thinking about his/her child’s pain. This, in turn, leads to hypervigilance and persistent fear in the child and parent. In the context of heightened fear, the child avoids activities that (s)he perceives as potentially harmful to his/her with parent protective behavior providing further encouragement for avoidance behavior. Ultimately, this leads to declines in child functioning and limitations in the life of the parent/caregiver. b. Child fear and catastrophizing and parent behavior had a direct and indirect influence on child avoidance behavior, while parent fear and catastrophizing indirectly influenced child avoidance. Overall, the model accounted for 20% of the variance in functional disability, X2(30) = 46.95, CFI = .97, RSMEA = .06 (CI=.02–.09). Child avoidance is measured with the Avoidance of Activities subscale of the Fear of Pain Questionnaire, Child report (FOPQ). Child disability is measured with the Functional Disability Inventory (FDI). Parent Avoidance is measured with the Parent Avoidance subscale of the Parent Fear of Pain Questionnaire (PFOPQ). PCS-C: Pain Catastrophizing Scale, Child report; ARCS: Adult Responses to Child’s Symptoms; PCS-P: Pain Catastrophizing Scale, Parent report.