

Abstract
Background:
Delayed puberty can result either from constitutional delay of growth and puberty (CDP) or idiopathic hypogonadotropic hypogonadism (IHH). Gonadotropin-releasing hormone (GnRH) stimulation test has been generally accepted as a current method for diagnosing delayed puberty. The objective of this research was to assess the cut-off values and the efficacy of GnRH stimulation test in the diagnosis of delayed puberty in both males and females.
Methods:
A study of 91 IHH, 27 CDP patients, 6 prepubertal children, and 20 pubertal adults was undertaken. Blood samples were obtained at 0, 30, 60, and 120 min after GnRH administration and the levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) were measured. For each parameter, the sensitivities and specificities were estimated, and the receiver operating characteristic (ROC) curves were constructed.
Results:
The ROC curves indicated that a serum basal LH <0.6 IU/L or peak LH <9.74 IU/L resulted in moderate sensitivity (73.8% or 80.0%) and specificity (90.9% or 86.4%) in the diagnosis of HH in males. Serum basal LH <0.85 IU/L or basal FSH <2.43 IU/L resulted in moderate sensitivity (80.0% or 100.0%) and specificity (75.0% or 50.0%) in the diagnosis of HH in females.
Conclusions:
Our data suggest that isolated use of the gonadorelin stimulation test is almost sufficient to discriminate between HH and CDP in males, but unnecessary in females. The most useful predictor is serum basal or peak LH to differentiate these two disorders in males, but serum basal LH or FSH in females.
Keywords: Constitutional Delay of Growth and Puberty, Delayed puberty, Gonadotropin-releasing Hormone, Idiopathic Hypogonadotropic Hypogonadism
INTRODUCTION
Delayed puberty is one of the most common issues presenting to pediatric endocrinologists. The prevalence is approximately 5% at age 14 in boys, with 0.1% remaining prepubertal by age 18.[1] The most common cause of delayed puberty was a constitutional delay of growth and puberty (CDP), which affected 53% of the patients (63% of males and 30% of females).[2] CDP is a benign condition that recovers spontaneously. In contrast, idiopathic hypogonadotropic hypogonadism (IHH) is a rare genetic condition (prevalence 0.025%), which is caused by defective gonadotropin secretion from the anterior pituitary because of defective gonadotropin-releasing hormone (GnRH) from the hypothalamus.[3] Discrimination between IHH and CDP is of great importance in terms of treatment; however, in most cases, differentiation is very difficult. The GnRH stimulation test appears to be the most widely used test in the differential diagnosis of IHH and CDP. This test can evaluate the hypothalamus–pituitary–gonadal (HPG) axis by stimulating the pituitary gland to secrete luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Although, there have been various research studies abroad during the past decades, currently no cut-off values for this test have been generally accepted in China. Additionally, there is no comprehensive statistical analysis or evaluation on the cut-off values of the GnRH stimulation test for discrimination between these two disorders in females. In this study, we investigated the cut-off values of the GnRH (gonadorelin) stimulation test to discriminate between IHH and CDP by estimating the values of LH and FSH at various time points after GnRH stimulation, and evaluating the sensitivity and specificity of the test.
METHODS
Patients
This retrospective study was done by reviewing the medical records of 91 IHH (including 62 normosmic IHH and 29 Kallmann syndrome) and 27 CDP patients, who presented at Chinese PLA General Hospital between 1994 and 2011, as well as 6 normal prepubertal children, and 20 normal pubertal volunteers. Evaluation included documentation of the history of onset and the progression of pubertal changes including Tanner breast (girls), testicular volumes (boys), and pubic hair stages, height and weight, growth velocity, bone age, olfactory sense, basal LH, FSH, testosterone, estradiol, prolactin, and progesterone levels, and GnRH stimulation testing.
Study protocol
Blood samples were obtained in the supine position and after an overnight fast, starting between 8:30 and 9:00 am. Gonadorelin acetate (100 μg; Fengyuan Pharmaceutical, Anhui, China) was then administered subcutaneously, and blood samples were drawn from an indwelling catheter positioned in an antecubital vein at 0, 30, 60, and 120 min after stimulation. The blood samples were immediately centrifuged, and serum was kept at −20°C until assayed. The protocol was approved by the ethics committee at the Chinese PLA General Hospital.
Hormone assays
Serum LH and FSH concentrations were determined by a fully automated immunometric chemiluminescent assay (ADVIA Centaur XP Immunoassay System, Siemens Healthcare Diagnostics, Inc., USA). The calibration range and analytical sensitivity for LH were 0.07–200 IU/L, and that of FSH was 0.3–200 IU/L. The mean intra- and inter-assay coefficients of variation were 3.3% and 4.0% for LH, and 2.9% and 2.7% for FSH.
Statistical analysis
The analysis was performed using SPSS version 19.0 software (IBM, Chicago, IL, USA). All data are expressed as mean ± standard error of the mean. All data from the two groups were compared using the two independent samples t-test. Statistical significance was accepted at P < 0.05. The receiver operating characteristic (ROC) curve was used to depict and determine the cut-off values. The area under the ROC (AUC) was computed to assess the predictive diagnostic value of the GnRH stimulation test and select the best predictors. A test with an AUC >0.9 is considered to have high accuracy, while 0.7–0.9 indicates moderate accuracy, 0.5–0.7 indicates low accuracy and 0.5 indicates a chance result.[4]
RESULTS
The basal information of all patients and volunteers is depicted in Table 1. Testosterone levels in male IHH (t = –87.4, P < 0.001) and CDP (t = –44.8, P < 0.001) patients and the estradiol levels in female IHH (t = –15.8, P < 0.001) and CDP (t = –9.5, P < 0.001) patients are much lower than those in male and female pubertal adults.
Table 1.
Clinical characteristics of study patients and control subjects
| Indices | Patients | Control subjects | |||||
|---|---|---|---|---|---|---|---|
| IHH | CDP | Prepubertal | Pubertal | ||||
| Male (n = 81) | Female (n = 10) | Male (n = 23) | Female (n = 4) | Male (n = 6) | Male (n = 10) | Female (n = 10) | |
| Chronologic age (year) | 18.83 ± 0.59 | 23.20 ± 2.78 | 15.09 ± 0.28 | 16.75 ± 0.49 | 11.17 ± 0.70 | 24.90 ± 0.35 | 24.40 ± 0.34 |
| Height (cm) | 168.25 ± 1.33 | 162.00 ± 2.48 | 152.61 ± 2.68 | 162.25 ± 2.63 | 149.50 ± 5.70 | 173.60 ± 1.60 | 164.10 ± 1.46 |
| Weight (kg) | 66.00 ± 1.97 | 49.93 ± 3.09 | 50.95 ± 4.22 | 45.50 ± 2.18 | 53.42 ± 6.29 | 70.50 ± 4.88 | 58.60 ± 2.07 |
| BMI (kg/m2) | 23.03 ± 0.52 | 18.79 ± 0.78 | 21.52 ± 1.34 | 16.80 ± 1.00 | 23.32 ± 1.36 | 23.29 ± 1.30 | 21.76 ± 0.74 |
| Testosterone (nmol/L) | 1.48 ± 0.20 | – | 1.62 ± 0.42 | – | 1.08 ± 0.20 | 19.50 ± 1.84 | – |
| Estradiol (pmol/L) | – | 35.14 ± 3.39 | – | 44.71 ± 8.01 | – | – | 408.76 ± 74.5 |
Data are mean ± SEM. BMI: Body mass index; IHH: Idiopathic hypogonadotropic hypogonadism; CDP: Constitutional delay of puberty; SEM: Standard error of mean.
Baseline hormonal levels, responses to peak LH and FSH levels to GnRH, and the time to peak hormonal levels after GnRH stimulation are depicted in Table 2 and Figure 1. Pubertal adults showed the highest peak LH and FSH responses after GnRH stimulation, whereas the CDP patients showed intermediate responses between those found in IHH patients and in pubertal children. Peak serum LH levels occurred mainly within 30 min after stimulation in CDP, prepubertal and pubertal groups, and within 60 min after stimulation in IHH groups. However, this difference does not exist in time to peak serum FSH levels.
Table 2.
Serum LH and FSH levels before and after gonadorelin stimulation and time to peak serum LH and FSH levels in study patients and control subjects
| Indices | Patients | Control subjects | |||||
|---|---|---|---|---|---|---|---|
| IHH | CDP | Prepubertal | Pubertal | ||||
| Male (n = 81) | Female (n = 10) | Male (n = 23) | Female (n = 4) | Male (n = 6) | Male (n = 10) | Female (n = 10) | |
| LH (IU/L) | |||||||
| Baseline | 0.63 ± 1.09 | 0.57 ± 0.21 | 2.11 ± 0.45 | 1.54 ± 0.63 | 0.43 ± 0.14 | 4.04 ± 0.59 | 11.03 ± 3.94 |
| Peak | 6.77 ± 0.86 | 8.66 ± 3.80 | 15.29 ± 1.43 | 23.25 ± 7.66 | 7.86 ± 2.70 | 35.92 ± 2.26 | 60.94 ± 18.41 |
| Time of peak (%) | |||||||
| 30 min | 44.4 | 20 | 56.5 | 100 | 66.7 | 90 | 50 |
| 60 min | 50.6 | 60 | 34.8 | 0 | 33.3 | 10 | 30 |
| 120 min | 4.9 | 20 | 8.7 | 0 | 0 | 0 | 20 |
| FSH (IU/L) | |||||||
| Baseline | 1.30 ± 0.16 | 1.24 ± 0.26 | 3.61 ± 0.59 | 2.79 ± 1.02 | 1.94 ± 0.43 | 4.21 ± 0.60 | 7.55 ± 3.21 |
| Peak | 5.03 ± 0.58 | 6.42 ± 0.84 | 10.02 ± 1.32 | 8.20 ± 3.27 | 7.27 ± 1.10 | 9.27 ± 1.01 | 12.74 ± 2.97 |
| Time of peak (%) | |||||||
| 30 min | 13.6 | 0 | 8.7 | 50 | 0 | 30 | 10 |
| 60 min | 37.0 | 10 | 34.8 | 25 | 66.7 | 70 | 30 |
| 120 min | 48.1 | 90 | 52.2 | 25 | 33.3 | 0 | 60 |
Data are mean ± SEM. LH: Luteinizing hormone; FSH: Follicle-stimulating hormone; IHH: Idiopathic hypogonadotropic hypogonadism; CDP: Constitutional delay of puberty; SEM: Standard error of mean.
Figure 1.
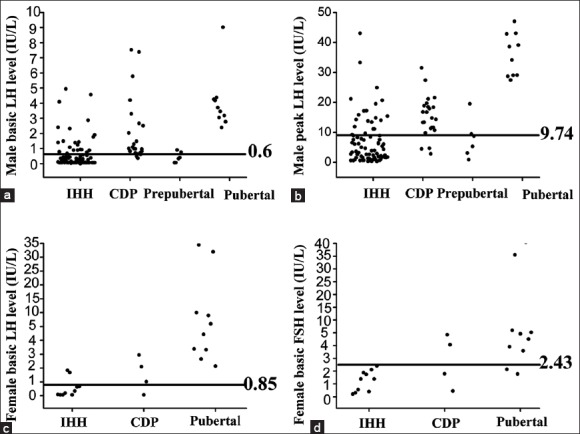
Mean serum luteinizing hormone and follicle-stimulating hormone levels before or after gonadotropin-releasing hormone stimulation in all groups. a: male basic LH level; b: male peak LH level; c: female basic LH level; d: female basic FSH level.
The ROC curves and the AUCs of basic LH and FSH levels, peak LH and FSH levels, as well as the differences between baseline and peak hormonal levels (Δ values) in both males and females were analyzed. The AUCs were 0.847 (basic LH levels), 0.845 (peak LH levels), 0.825 (ΔLH levels), 0.823 (basic FSH levels), 0.809 (peak FSH levels), and 0.726 (ΔFSH levels) in males. Given that basic and peak serum LH levels had the greatest AUCs, these are the most effective predictors for diagnosing IHH and CDP patients in males. The AUCs were 0.750 (basic FSH levels), 0.738 (basic LH levels), 0.675 (peak LH levels), 0.675 (ΔLH levels), 0.525 (peak FSH levels), and 0.450 (ΔFSH levels) in females. Basic serum LH and FSH levels had the greatest AUCs and were the most effective predictors for diagnosing IHH and CDP patients in females, meaning that the GnRH stimulation test is unnecessary in differentiating between IHH and CDP in female patients.
DISCUSSION
Normal puberty occurs as a consequence of resurgence of the episodic GnRH stimulation from the hypothalamus, resulting in an increase in the frequency and magnitude of the episodic release of pituitary gonadotropins, especially LH. Delayed puberty is defined clinically by the absence or incomplete development of secondary sexual characteristics bounded by an age of 14 for boys (i.e., testicular size >4 ml being the first sign) and 13.4 for girls (breast development being the first sign).[5] CDP is the most common cause of delayed puberty, which results from a delay in reactivation of the GnRH pulse generator. IHH is a rare genetic condition caused by a defective gonadotropin secretion from the anterior pituitary because of defective GnRH from the hypothalamus. Discrimination between IHH and CDP is very difficult. Clinical characteristics, if present, may be useful for diagnosis, such as a positive family history, slow prepubertal growth with skeletal delay, or the presence of chronic diseases. However, these characteristics are not sufficient. In practice, a decision is often made to treat patients with sex steroids to optimize their growth and pubertal progress and reassess later in terms of diagnosis. However, a definitive diagnosis would be important from the viewpoint of long-term prognosis for fertility and to alleviate anxiety in adolescents with CDP. HPG axis function should be clearly defined before starting sex steroid replacement therapy, which has the potential to inhibit a normal HPG axis. Thus, the various tests have been used to differentiate children with delayed puberty such as the GnRH stimulation test, human chorionic gonadotropin stimulation test, thyrotropin releasing hormone-stimulated test, overnight frequent LH sampling, urinary LH evaluation, and repetitive intravenous GnRH testing.[6,7,8,9] Of these, the GnRH stimulation test appears to be the most widely used, is simple, effective, and relatively inexpensive, and well-tolerated considering that other options are time-consuming, expensive, and difficult to perform on an ambulatory basis. However, the predictive value of the GnRH stimulation test has been in controversy, and there is no comprehensive statistical analysis or evaluation in China.[10,11,12] Moreover, no data have been published on the predictive value of the GnRH stimulation test to discriminate between IHH and CDP in females.
Analogs of GnRH have been synthesized since the 1970s, and buserelin, nafarelin, leuprolide, and triptorelin are some common analogs of GnRH.[13] Our data show that males with CDP show an increase in LH levels after GnRH stimulation, which distinguishes them from patients with gonadotropin deficiency. The predictive value of this test is almost sufficient to discriminate between IHH and CDP in males, though there is also overlap between the two groups, as shown in previous studies. The best predictor is peak LH levels after GnRH stimulation. ROC analysis revealed that the cut-off point for peak LH levels was 9.74 IU/L (sensitivity 80.0%, specificity 86.4%). These results are close to those from a study conducted at the Chinese Academy of Medical Science and the Peking Union Medical College (8 IU/L).[14] However, this cut-off value is a little higher than other GnRH analog stimulation tests, such as buserelin, nafarelin, leuprolide, and triptorelin.[10,12,13] It is possible that in the in vivo setting, GnRH has a more enhanced pituitary gonadotrophic stimulatory effect than GnRH analogs. However, there are no sufficient available pharmacokinetic data on the effect of GnRH on gonadotropin release and serum levels. In future, pharmacokinetic studies on the effect of GnRH on plasma LH and FSH levels may be useful to optimize the GnRH protocol. Our data show that the basic LH value, which was previously reported useless to discriminate between IHH and CDP, is not lower than peak LH levels. This difference may rely on a more accurate LH assay than past decades, providing clearer discrimination in differentiating patients with IHH from those with a normal HPG axis, including CDP.[15] These results confirm the validity and specificity of GnRH stimulation in the differential diagnosis between IHH and CDP in males, but also suggest that the unstimulated LH levels may also be an important screening tool in differential diagnosis.
Unlike males, peak LH levels are not a good predictor to discriminate between IHH and CDP in females, and the best predictors are basic LH and FSH levels. ROC analysis revealed that the cut-off point for basic LH levels was 0.85 IU/L (sensitivity 80.0%, specificity 75.0%) and for basic FSH levels was 2.43 IU/L (sensitivity 100.0%, specificity 50.0%). These results indicate that the basic hormonal levels are also very important in differentiating patients with IHH from those with CDP, especially in females. Although the prevalence of IHH and CDP in females is very low, these patients should not be ignored. Our data show that the best predictors in females are basic rather than peak LH or FSH levels, demonstrating that the GnRH stimulation test may not be helpful in diagnosing females whereas basic hormone levels may be very useful. Given that the basic hormone levels are not sufficient for diagnosis, clinical characteristics, if present, are also very useful for diagnosis, such as a positive family history, slow prepubertal growth with skeletal delay, or the presence of chronic diseases. A limitation of this study is the number of females; therefore, further studies are needed to find more effective methods for diagnosis in females. Moreover, peak serum LH levels occurred mainly within 30 min after stimulation in the CDP group (56.5% in males and 100% in females), while within or after 60 min after stimulation in the IHH group (55.5% in males and 80% in females). Although the overlap is significant, it may also be helpful in differential diagnosis.
In conclusion, this study is the first comprehensive statistical analysis and evaluation of the cut-off values and diagnostic value of the GnRH stimulation test to discriminate between IHH and CDP in both males and females in China. The results suggest that the GnRH stimulation test is almost sufficient to discriminate between IHH and CDP in males, but useless for diagnosis in females. However, our study was conducted at a single site, and the number of females in the sample was limited. Thus, multicenter and large sample studies in China are needed to establish standards for GnRH stimulation testing in the future.
Financial support and sponsorship
This work was supported in part by National Science and Technology Major Project Grant Number (2011ZX09307-001-08).
Conflicts of interest
There are no conflicts of interest.
Footnotes
Edited by: Xiu-Yuan Hao
REFERENCES
- 1.Harlan WR, Grillo GP, Cornoni-Huntley J, Leaverton PE. Secondary sex characteristics of boys 12 to 17 years of age: The U.S. Health Examination Survey. J Pediatr. 1979;95:293–7. doi: 10.1016/s0022-3476(79)80677-0. [DOI] [PubMed] [Google Scholar]
- 2.Sedlmeyer IL, Palmert MR. Delayed puberty: Analysis of a large case series from an academic center. J Clin Endocrinol Metab. 2002;87:1613–20. doi: 10.1210/jcem.87.4.8395. [DOI] [PubMed] [Google Scholar]
- 3.Fathi AK, Luo X. Normosmic idiopathic hypogonadotropic hypogonadism: Update on the genetic background and future challenges. J Pediatr Endocrinol Metab. 2013;26:405–15. doi: 10.1515/jpem-2013-0061. [DOI] [PubMed] [Google Scholar]
- 4.Akobeng AK. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007;96:644–7. doi: 10.1111/j.1651-2227.2006.00178.x. [DOI] [PubMed] [Google Scholar]
- 5.Traggiai C, Stanhope R. Delayed puberty. Best Pract Res Clin Endocrinol Metab. 2002;16:139–51. doi: 10.1053/beem.2001.0186. [DOI] [PubMed] [Google Scholar]
- 6.Savage MO, Preece MA, Cameron N, Jones J, Theintz G, Penfold JL, et al. Gonadotrophin response to LH-RH in boys with delayed growth and adolescence. Arch Dis Child. 1981;56:552–6. doi: 10.1136/adc.56.7.552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kauschansky A, Dickerman Z, Phillip M, Weintrob N, Strich D. Use of GnRH agonist and human chorionic gonadotrophin tests for differentiating constitutional delayed puberty from gonadotrophin deficiency in boys. Clin Endocrinol (Oxf) 2002;56:603–7. doi: 10.1046/j.1365-2265.2002.01520.x. [DOI] [PubMed] [Google Scholar]
- 8.Büyükgebiz A, Oktay S. The role of TRH-stimulated prolactin responses in distinguishing gonadotropin deficiency from constitutional delayed puberty. J Pediatr Endocrinol. 1994;7:325–30. doi: 10.1515/jpem.1994.7.4.325. [DOI] [PubMed] [Google Scholar]
- 9.Smals AG, Hermus AR, Boers GH, Pieters GF, Benraad TJ, Kloppenborg PW. Predictive value of luteinizing hormone releasing hormone (LHRH) bolus testing before and after 36-hour pulsatile LHRH administration in the differential diagnosis of constitutional delay of puberty and male hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 1994;78:602–8. doi: 10.1210/jcem.78.3.8126131. [DOI] [PubMed] [Google Scholar]
- 10.Kanika G, Jose FC, Robert LR. Gonadotropin releasing hormone agonist (nafarelin) test to differentiate gonadotropin deficiency from constitutionally delayed puberty in teen-age boys – A clinical research center study. J Clin Endocrinol Metab. 1995;80:2980–6. doi: 10.1210/jcem.80.10.7559884. [DOI] [PubMed] [Google Scholar]
- 11.Lanes R, Gunczler P, Osuna JA, Palacios A, Carrillo E, Ramirez X, et al. Effectiveness and limitations of the use of the gonadotropin-releasing hormone agonist leuprolide acetate in the diagnosis of delayed puberty in males. Horm Res. 1997;48:1–4. doi: 10.1159/000185421. [DOI] [PubMed] [Google Scholar]
- 12.Street ME, Bandello MA, Terzi C, Ibañez L, Ghizzoni L, Volta C, et al. Leuteinizing hormone responses to leuprolide acetate discriminate between hypogonadotropic hypogonadism and constitutional delay of puberty. Fertil Steril. 2002;77:555–60. doi: 10.1016/s0015-0282(01)03213-7. [DOI] [PubMed] [Google Scholar]
- 13.Wilson DA, Hofman PL, Miles HL, Unwin KE, McGrail CE, Cutfield WS. Evaluation of the buserelin stimulation test in diagnosing gonadotropin deficiency in males with delayed puberty. J Pediatr. 2006;148:89–94. doi: 10.1016/j.jpeds.2005.08.045. [DOI] [PubMed] [Google Scholar]
- 14.Pan H, Shi YF, Deng JY, Wu XY, Lu S. Clinical value of LHRH exciting test in differential diagnosis of constitutional delayed puberty and male hypogonadotropic hypogonadism. Chin J Endocrinol Metab. 2003;19:110–4. [Google Scholar]
- 15.Resende EA, Lara BH, Reis JD, Ferreira BP, Pereira GA, Borges MF. Assessment of basal and gonadotropin-releasing hormone-stimulated gonadotropins by immunochemiluminometric and immunofluorometric assays in normal children. J Clin Endocrinol Metab. 2007;92:1424–9. doi: 10.1210/jc.2006-1569. [DOI] [PubMed] [Google Scholar]