

Abstract
Background:
Osteoporosis is commonly encountered by postmenopausal women. There is an increased need for a low cost and efficient treatment alternative to address this population.
Aims:
To study the effects of integrated yoga on bone mineral density (BMD) in postmenopausal women with osteoporosis.
Settings and Designs:
Experimental pre-post study conducted in a community setting.
Materials and Methods:
30 females in the age group of 45–62 years suffering from postmenopausal osteoporosis with a dual-energy X-ray absorptiometry (DEXA) score of ≤−2.5 underwent a 6 months fully supervised yoga session. All the participants completed the study. Pretraining and posttraining BMD was calculated. Outcome measure: DEXA score at the lumbar spine.
Statistical Analysis:
The study was statistically analyzed using paired t-test to see the significance of pretraining and posttraining effects of a yoga session.
Results:
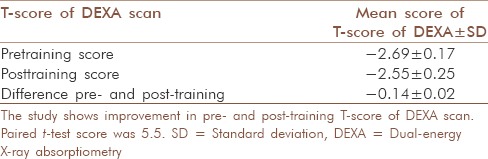
Improvement in T-score of DEXA scan of −2.55 ± 0.25 at posttraining as compared to a pretraining score of −2.69 ± 0.17.
Conclusions:
Integrated yoga is a safe mode of physical activity which includes weight bearing as well as not weight bearing asanas, Pranayama, and suryanamaskar, all of which helps induce improvement in BMD in postmenopausal osteoporotic females.
Keywords: Dual-energy X-ray absorptiometry-scan, menopause, osteoporosis, yogasanas
INTRODUCTION
Osteoporosis has been defined as a progressive bone disease characterized by decreased bone mass and density leading to bone fragility and increased risk of fractures.[1] Primary type 1 osteoporosis occurs due to the low level of estrogen in postmenopausal women. Primary type 2 also known as senile osteoporosis affects both females and males greater than age 75 years at a ratio of 2:1.[2] Secondary osteoporosis affects males and females at an equal ratio at any age. Hence, females are at an increased risk of developing osteoporosis.[3]
In early adult life, the remodeling cycle of bone resorption and formation allows the skeleton to adjust changes in biomechanical stresses and to repair deficits that occur in bone. During menopause and aging; the perfect link between amounts of bone resorbed and subsequently laid down is broken; with a net deficit occurring at the end of each remodeling cycle. It is characterized by pain, gradual loss of height, dowager's hump (severe kyphosis), and osteoporotic bone fractures.[4]
The peak bone mass can be maximized by pharmacological and nonpharmacological means.[4] Pharmacological means includes drugs calcium supplements, bisphosphonates, Vitamin D, hormone replacement therapy, which includes estrogen, progesterone, and calcitonin.[4,5] Nonpharmacological treatment includes weight bearing exercises, yoga, and diet.
Bone strength is seen to be improved by weight bearing endurance exercises and muscle strength training.[6] In addition, aerobics and resistance training help maintain or increase the bone mineral density (BMD) in postmenopausal women.[7] Regular exercise helps to slow the rate of aging of the skeleton. Regardless of age, individual who maintain an active lifestyle have significantly greater bone mass compared to sedentary counterparts.[8] This benefit is maintained into the seventh and eighth decade of life. Exercises of weight bearing nature, which includes walking, running, dancing, rope skipping, all activities like circuit resistance training in which significant muscle forces can be generated against the long bones of the body are extremely beneficial.[9]
If the female has already begun to lose the mass or is otherwise susceptible to vertebral stress fractures, running can put too much stress on the knees, ankles, and lumbar spine. Furthermore, weight-bearing activities such as walking or running, only benefit lower limbs, and do nothing to strengthen the wrists, elbows, shoulders, or upper back. The drawback of the aerobic exercises is that there is the corresponding drop in body fat which can result in loss of BMD.[10]
The resistance training; such as working out with free weights or circuit training is a particularly effective method of strengthening bone. Postmenopausal women performing regularly resisted training exercises causes 1% increment in BMD.[11] This training program requires specific elaborate equipment which are costly.[12] It also needs a special place to perform this resisted training regime.
Many health practitioners today are therefore increasingly turning towards alternative therapies to improve health and lifestyle. Yoga is recommended and is becoming increasingly popular to counter the negative effects of menopause on the female body. It then serves the purpose in several ways.
Yoga can stimulate the bones to retain calcium, provided the body gets enough calcium in the first place.[13] It does this through weight bearing poses of yogasanas that affect the spine, arms, shoulders, elbows, legs while encouraging a full range of motion. Weight bearing yoga training has shown a positive effect on the bone by reducing the bone resorption and hence preventing the risk of osteoporosis in postmenopausal women.[14] It also has a positive effect on improving the quality of life and balance.[14,15,16]
Study proves that yoga enhances muscular strength and body flexibility.[15] It is one of the few exercise systems in which weight is borne through the arms and upper body, causing bones to become thicker and stronger. Recent research has proved that yoga can alleviate some of the height loss associated with osteoporosis.[17] Yoga can be used as alternative therapy to exercises.[16]
Thus, the present study was done to analyze the effects of integrated yoga on osteoporosis.
MATERIALS AND METHODS
Study design and settings
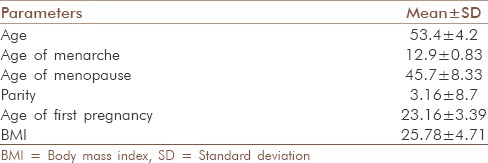
The study was an experimental pre-post study. A total of 30 functionally active females in the age group of 45–62 years suffering from postmenopausal osteoporosis, with a dual-energy X-ray absorptiometry (DEXA) score of ≤−2.5 were selected for this study, based on consecutive sampling. Subjects were excluded if they had fractures associated with osteoporosis and any major associated illness of cardiovascular, neurological, or respiratory system that deemed them unfit for performing yogasanas. Selected subjects were then asked to read and sign a consent form for the confirmation of them being involved in the study. At this time, demographic details (gender, age, height, weight, age of menopause, the age of menarche, parity, number of abortions, and age of 1st pregnancy), family history of osteoporosis, details about the diet, supplements, and physical activity were recorded [Table 1]. Ethical clearance was obtained from the institution before proceeding.
Table 1.
Integrated yogasanas

All the subjects included in the study were involved in a 6 months fully supervised yoga session. The session was supervised by a physical therapist and a yoga instructor.
Procedure
Individuals who were included in the study underwent 1 h yoga session for 4 days every week for 6 months. The session for 1 h involved warm-ups, suryanamaskar, and asanas in different positions (standing, sitting, supine, and prone). Each position included three different asanas one of which was meant for relaxation to the subjects; also to let them get ready for the next position without any stress. These were followed by Pranayama and Omkar. Each asana was repeated 5 times with holds of 15–30 s [Table 2]. After completion of 6 months of yoga intervention, T-score of DEXA scan at the lumbar spine was calculated. Patients were asked to report about their overall experience in terms of any pain or discomfort during the yoga practice for 6 months on completion of the study. This was not measured using any outcome score.
Table 2.
Demographic data
DATA ANALYSIS AND RESULTS
The study was statistically analyzed using paired t-test to see the significance of pretraining and posttraining effects of the yoga session.
DISCUSSION
This experimental pre-post trial was done to find the effects of yogasanas on osteoporosis in postmenopausal women. The results showed improvement in BMD (as shown by the increase in T-score of DEXA scan at lumbar spine).
The BMD score of spine showed improvement from pre T-score of −2.69 to post T-score of −2.55 which suggest high significance [Table 3] where P < 0.05. Thus with various weight bearing yogasanas BMD has indeed improved. The study also showed that intervention at any age can reverse and improve BMD losses imposed by menopause or ageing.
Table 3.
Mean scores and SD of pre- and post-training scores and the difference between pre- and post-training scores
Improvement in BMD could be attributed to the effects of mechanotransduction which plays an important role in pathologic fracture healing, physical adaptations, and most importantly the therapeutic adaptations to osteogenesis.[18] In order to meet the functional demands in the mechanical environment, physical remodeling of the bone takes place. There is a dynamic balance maintained between the process osteogenesis and bone resorption by the virtue of mechanical loading which activates the mechanotransducers to do so.[18]
A pilot study done by Fishman showed significant improvement in the T-score at spine and hip over a period of 2 years. The study included various yogasanas such as trikonasana, bhujanganasa, setu bandhasana, and paschimotasana which were also a component of the current study. Above study showed greater increase in BMD at the hip as compared to the spine.[19]
Study done by Angin and Erden showed an improvement in the T-score, though there was no significant difference between the mean improvements obtained after the exercise program for the postmenopausal osteoporotic and osteopenic groups, but 43.8% of osteoporotic women had a T-score showing osteopenia, and 23.5% of osteopenic women had a T-score falling within normal range.[20]
A study done on comparing the effects of osteoporosis prevention exercise protocol versus walking for preventing osteoporosis in younger females, by Soomro et al., showed no difference in the T-score of both groups after 3 months of intervention, which implicated further studies to be done for longer duration to evaluate the efficacy of the exercise protocol.[21]
Yogasanas has also contributed to the improvement in joint mobility, the range of motion and flexibility of muscles.[22] It has positive effects on patients ailing with back pain, arthritis, and issues related to increased risk of falls, which might lead to osteoporotic fractures.[19,23] It helps improve the overall quality of life of an individual.
Pranayama helps relax the body and mind, regulates the blood pressure and heart rate, and improves the lung function of people suffering from asthma.[24,25,26] It also addresses stress, anxiety, depression, stress-related medical illness, etc.[27]
An additional observation was that yogasanas was a safe method of physical activity and had no adverse effects if addressed to women in their postmenopausal age by a trained yoga practitioner; as noted in the study population.
Therefore, it was concluded that various weight bearing as well as nonweight bearing asanas along with Pranayama and suryanamaskar are effective in improving BMD and integrated yoga exercises should be an important component of any osteoporosis treatment exercise regime.
CONCLUSION
Statistically, a significant difference was found in the BMD score posttraining as compared to the pretraining T-score. However, the clinically beneficial effects of the selected integrated yoga could not be commented upon in terms of functional improvement of the participants as the only difference in the T-score was measured pre- and post-intervention. Further, no report of discomfort or pain during the session was reported by any of the participants. Thus, we could conclude that integrated yoga is a safe mode of physical activity which includes weight bearing as well as not weight bearing asanas, Pranayama, and suryanamaskar, all of which helps induce improvement in BMD in postmenopausal osteoporotic females.
Limitation and future direction
This study had the small sample size and no control group. More sample size would be costlier, and no funding was received. Hence, future studies can be done with a larger sample size and a control group. Furthermore, the overall experience of the patient at the end of the study in terms of patient satisfaction or functional abilities can be measured. Studies can also be done comparing yoga and other weight bearing exercises.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank all the participants who participated in the study. We would additionally like to thank Mrs. Nirmala Date, yoga specialist and to Dr. Rachana Dhabadgav.
REFERENCES
- 1.Alldredge BK, Koda-Kimble AM, Lloyd YY, Kradjan WA. Philadelphia: Wolters Kluwer Health/Lippincott Williams and Wilkins; 2009. Applied Therapeutics: The Clinical Use of Drugs; pp. 101–3. [Google Scholar]
- 2.Available from: http://www.adjustforwellness.com/osteoporosis. . [Last Cited on 2015 Sept 15].
- 3.Mayoclinic.org. [Last Cited on 2005 Jun 21]. Available from: http://www.mayoclinic.org/diseasesconditions/osteoporosis/basics/risk-factors/con-20019924 .
- 4.Fordham J. London: Elsevier Health Sciences; 2003. Osteoporosis: Your Questions Answered; pp. 3–5. [Google Scholar]
- 5.Cranney A. Treatment of postmenopausal osteoporosis. BMJ. 2003;327:355–6. doi: 10.1136/bmj.327.7411.355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Body JJ, Bergmann P, Boonen S, Boutsen Y, Bruyere O, Devogelaer JP, et al. Non-pharmacological management of osteoporosis: A consensus of the Belgian Bone Club. Osteoporos Int. 2011;22:2769–88. doi: 10.1007/s00198-011-1545-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Howe TE, Shea B, Dawson LJ, Downie F, Murray A, Ross C, et al. Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane Database Syst Rev. 2011;7:CD000333. doi: 10.1002/14651858.CD000333.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lewis RD, Modlesky CM. Nutrition, physical activity, and bone health in women. Int J Sport Nutr. 1998;8:250–84. doi: 10.1123/ijsn.8.3.250. [DOI] [PubMed] [Google Scholar]
- 9.Ramaswamy B, Shapiro CL. Osteopenia and osteoporosis in women with breast cancer. Semin Oncol. 2003;30:763–75. doi: 10.1053/j.seminoncol.2003.08.028. [DOI] [PubMed] [Google Scholar]
- 10.Martin D, Notelovitz M. Effects of aerobic training on bone mineral density of postmenopausal women. J Bone Miner Res. 1993;8:931–6. doi: 10.1002/jbmr.5650080805. [DOI] [PubMed] [Google Scholar]
- 11.Kronhed AC, Möller M. Effects of physical exercise on bone mass, balance skill and aerobic capacity in women and men with low bone mineral density, after one year of training – A prospective study. Scand J Med Sci Sports. 1998;8(5 Pt 1):290–8. doi: 10.1111/j.1600-0838.1998.tb00485.x. [DOI] [PubMed] [Google Scholar]
- 12.Troosters T, Gosselink R, Decramer M. Deconditioning, and principles of training. In: Weisman IM, Zeballos RJ, editors. Clinical Exercise Testing. Vol. 32. Basel: Karger Medical and Scientific Publishers; 2002. p. 67. [Google Scholar]
- 13.Sparrowe L. Good to the bone. Yoga J. 2001. [Last cited on 2015 Nov 3]. p. 112. Available from: http://books.google.co.in/books?id=JeoDAAAAMBAJ&pg=PA112&dq=Good+to+the+bone.+Yoga+Journal+2001&hl=en&sa=X&redir_esc=y#v=onepage&q=Good%20to%20the%20bone.%20Yoga%20Journal%202001&f=false .
- 14.Phoosuwan M, Kritpet T, Yuktanandana P. The effects of weight bearing yoga training on the bone resorption markers of the postmenopausal women. J Med Assoc Thai. 2009;92(Suppl5):S102–8. [PubMed] [Google Scholar]
- 15.Woodyard C. Exploring the therapeutic effects of yoga and its ability to increase quality of life. Int J Yoga. 2011;4:49–54. doi: 10.4103/0973-6131.85485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tüzün S, Aktas I, Akarirmak U, Sipahi S, Tüzün F. Yoga might be an alternative training for the quality of life and balance in postmenopausal osteoporosis. Eur J Phys Rehabil Med. 2010;46:69–72. [PubMed] [Google Scholar]
- 17.Sander E. Menopause the yoga way. Yoga J. 1996;126:68. [Google Scholar]
- 18.Huang C, Ogawa R. Mechanotransduction in bone repair and regeneration. FASEB J. 2010;24:3625–32. doi: 10.1096/fj.10-157370. [DOI] [PubMed] [Google Scholar]
- 19.Fishman LM. Yoga for osteoporosis a pilot study. Top Geriatr Rehabil. 2009;25:244–50. [Google Scholar]
- 20.Angin E, Erden Z. The effect of group exercise on postmenopausal osteoporosis and osteopenia. Acta Orthop Traumatol Turc. 2009;43:343–50. doi: 10.3944/AOTT.2009.343. [DOI] [PubMed] [Google Scholar]
- 21.Soomro RR, Ahmed SI, Khan M, Ali SS. Comparing the effects of Osteoporosis Prevention Exercise Protocol (OPEP) versus walking in the prevention of osteoporosis in younger females. Pak J Med Sci. 2015;31:336–40. doi: 10.12669/pjms.312.5990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Grabara M, Szopa J. Effects of hatha yoga exercises on spine flexibility in women over 50 years old. J Phys Ther Sci. 2015;27:361–5. doi: 10.1589/jpts.27.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sherman KJ, Cherkin DC, Erro J, Miglioretti DL, Deyo RA. Comparing yoga, exercise, and a self-care book for chronic low back pain: A randomized, controlled trial. Ann Intern Med. 2005;143:849–56. doi: 10.7326/0003-4819-143-12-200512200-00003. [DOI] [PubMed] [Google Scholar]
- 24.Yogicwayoflife.com. [Last cited on 2010 Mar 30]. Available from: http://www.yogicwayoflife.com/sheetali-pranayama-the-cooling-breath .
- 25.Pramanik T, Sharma HO, Mishra S, Mishra A, Prajapati R, Singh S. Immediate effect of slow pace bhastrika pranayama on blood pressure and heart rate. J Altern Complement Med. 2009;15:293–5. doi: 10.1089/acm.2008.0440. [DOI] [PubMed] [Google Scholar]
- 26.Saxena T, Saxena M. The effect of various breathing exercises (pranayama) in patients with bronchial asthma of mild to moderate severity. Int J Yoga. 2009;2:22–5. doi: 10.4103/0973-6131.53838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zope SA, Zope RA. Sudarshan kriya yoga: Breathing for health. Int J Yoga. 2013;6:4–10. doi: 10.4103/0973-6131.105935. [DOI] [PMC free article] [PubMed] [Google Scholar]