
Fig. 2.
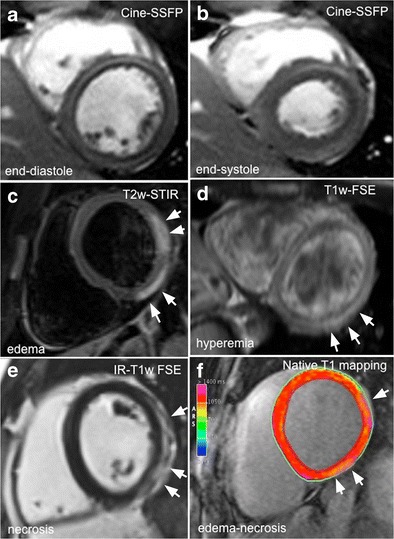
Comprehensive CMR evaluation in a 27-year-old man with acute myocarditis following an upper respiratory infection. At admission, patient presented with acute chest pain, abnormal ST segment elevation in the inferolateral leads, and mildly elevated troponin; left ventricular global function was preserved (a, b; ejection fraction 56 %). Typical hallmarks of active myocardial inflammation are portrayed, consisting of meso/subepicardial striae of high signal intensity on both T2-STIR and LGE images (c–e), combined with a positive EGEr (d; 7.6). Corresponding native T1 parametric map calculated using a modified Look-Locker inversion recovery (MOLLI) sequence with a 1.5 T magnet (MAGNETOM Avanto; Siemens Healthcare, Erlangen, Germany) shows increased T1 values in the same location (1211 ± 16 ms; normal reference value mean 1027 ± 61 ms; f)