
Figure 1.
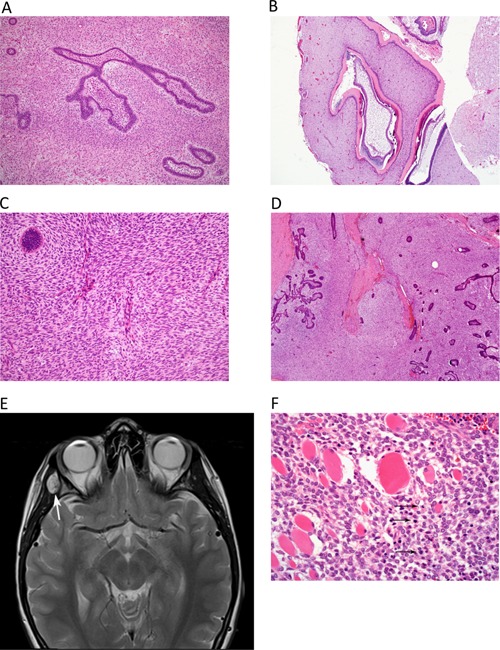
Histologic findings in the AFO and AFOS specimen and on MRI prior to first relapse. (A,B) Hematoxylin–eosin (HE) stained sections of the initial tumor [ameloblastic fibro‐odontoma (AFO)]. (A) Small islands and branching cords of ameloblastic epithelium are interspersed within spindle cell stroma. The mesenchymal component is of moderate cellularity, but no pleomorphism is present and mitotic activity is low (up to 2/10 hpf; magnification 100×. (B) Other areas show odontogenic epithelium and dentine; magnification 40×. (C,D) HE‐stained section of the first tumor recurrence [ameloblastic fibro‐odontosarcoma (AFOS)]. (C) The prominence of the mesenchymal (spindle cell) component is apparent and is of higher cellularity than the initial AFO; magnification 40×. (D) The fascicular fibrosarcoma‐like architecture of the spindle cell component is discernible in areas, and only a small island of epithelium is seen here (top left). There is a focal mild atypia, and increased mitotic count of the mesenchymal component (5/10 hpf); magnification 100×. (E) Surveillance MRI 4 months after completion of radiotherapy for AFOS with involved margins. T2‐weighted sequence shows focal area of high signal (arrows) lying on lateral wall of right orbit, involving right temporalis muscle. (F) HE‐stained section of the first relapse of AFOS. The tumor shows more aggressive morphology, with prominent cellularity and pleomorphism of the mesenchymal component, along with numerous mitotic figures (arrows) and a significantly increased mitotic index of 17/10 hpf. The tumor is seen to extensively infiltrate skeletal muscle fibres. The epithelial component is markedly reduced and is not seen in this field; magnification 200×.