
Fig 3.
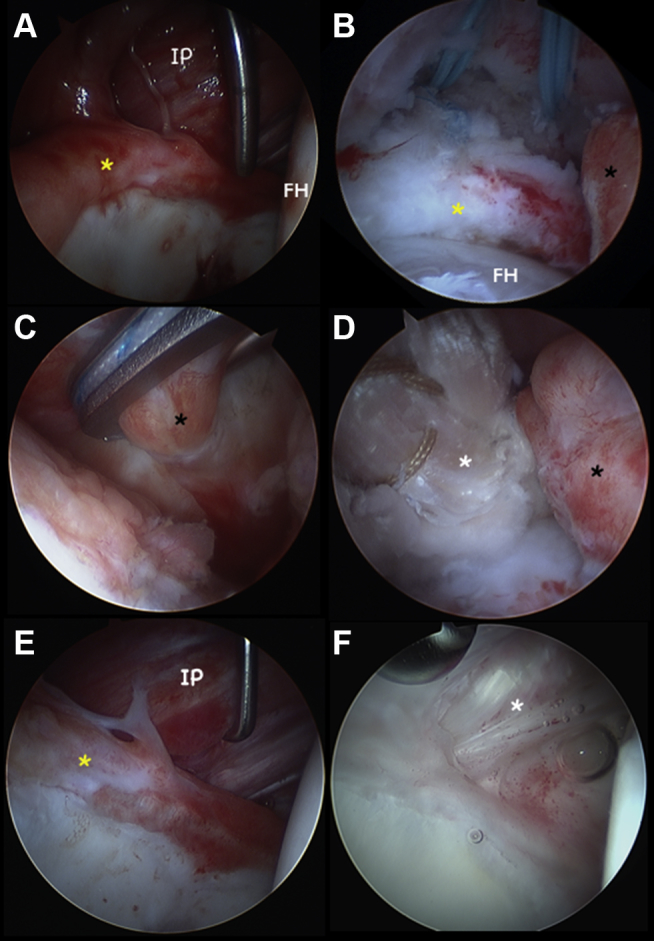
Intra-operative pictures of the same patient from Figure 2. (A) Iliopsoas muscle visualized with 30° arthroscope in mid-trochanteric portal under dry conditions, no capsule is seen. The iliopsoas is directly abutting the anterior labrum (yellow asterisk). (B) Arthroscope (70°) in mid-trochanteric portal viewing proximally in the peripheral compartment with traction released, with the labrum (yellow asterisk) resting nicely on the FH. Double loaded anchors placed in acetabular rim for proximal fixation. The distal capsular stump at the level of the zona orbicularis is seen to the right (black asterisk). (C) Speed stitch utilized to capture the distal capsular stump (black asterisk) near the zona orbicularis for suture passagee, while viewing “inside-out” with a 70° arthroscope in the mid-trochanteric portal. (D) Excellent approximation of distal capsular stump (black asterisk) with achilles graft (white asterisk) after tying the first suture. (E) Before view with 30-degree arthroscope through mid-trochanteric portal revealing inflamed anterior labrum (yellow asterisk, hours 1:30 to 3 are seen) post recurrent anterior dislocation. It is clear that no anterior capsule is present as the ilio-psoas muscle is seen (IP) behind/above the labrum. Femoral head is seen on the right. (F) A second look arthroscopy 12 month later depicting the same view. The well-incorporated Achilles allograft is seen (white asterisk). (IP, iliopsoas, FH, femoral head.)