

Abstract
Background:
Kidney transplantation is a preferred treatment for many patients with end-stage renal disease (ESRD) and is far more profitable than hemodialysis. Analyzing renal transplantation data can help to evaluate the effectiveness of transplantation interventions. The aim of this study was to determine the organ survival rate after kidney transplantation during a period of 10 years (March 2001-March 2011) among transplanted patients in Arak, Markazi Province, Iran.
Materials and Methods:
In this historical cohort study, all recipients of kidney transplantation from Arak, Markazi Province, Iran who had medical records in Valiasr Hospital and “charity for kidney patients” of Arak, Markazi Province, Iran during a period of 10 years from March 2001 to March 2011 were included. Data collected by using checklists were completed from patients’ hospital records. Kaplan-Meier method was used to determine the graft cumulative survival rate, log-rank test to compare survival curves in subgroups, and Cox regression model to define the hazard ratio and for ruling out the intervening factors. Statistical analysis was conducted by Statistical Package for the Social Sciences (SPSS) 20 and Stata 11.
Results:
Mean duration of follow-up was 55.43 ± 42.02 months. By using the Kaplan-Meier method, the cumulative probability of graft survival at 1, 3, 5, 7, and 10 years was 99.1, 97.7, 94.3, 85.7, and 62.1%, respectively. The number of dialysis by controlling the effect of other variables had a significant association with the risk of graft failure [hazard ratios and 95% confidence interval (CI): 1.47 (1.02-2.13)].
Conclusion:
This study showed that the graft survival rate was satisfactory in this community and was similar to the results of single-center studies in the world. Dialysis time after transplantation was a significant predictor of survival in the recipients of kidney transplantation that should be considered.
Keywords: Graft rejection, Iran, kidney transplantation, survival analysis
INTRODUCTION
End-stage renal disease (ESRD) is a potential outcome of chronic kidney disease (CKD).[1] The prevalence and incidence of ESRD as a worldwide public health concern are increasing in developed and developing countries. According to the report published by the Management Center for Transplantation and Special Disease (MCTSD) affiliated to Iran's Ministry of Health in 2007, the total number of patients with ESRD undergoing renal replacement therapy (RRT) was 32,686, which indicates a prevalence of 435.8 per million population (population = 75 million people).[2] Usually, these patients are treated by hemodialysis,[3] kidney transplantation,[4] and peritoneal dialysis.[5,6] These RRTs were started in Iran in 1964, 1967, and 1975 and at present kidney transplantation is the most common among them in Iran (48.8%).[2,7] Kidney transplantation is the preferred treatment for most patients with ESRD and is far more profitable than hemodialysis.[8,9] Transplanted patients have better quality of life and survival rate.[10] The first kidney transplant in Iran that was performed in Shiraz, Fars Province, Iran in 1967 was the first organ transplant among the countries that are current members of the Middle East Society for Organ Transplantation (MESOT).[7,11] Over the past three decades, the number of kidney transplants has steadily increased that is concurrent with the development of the primary health care system, reduction of mortality, population growth, increase of life expectancy, and a significant shift from communicable to noncommunicable diseases.[11,12] There are three different resources for kidney transplants including living-related, living-unrelated, and deceased donors[10] and the function of kidneys from living donors is better than from deceased individuals.[13] In 2013, there were 2,670 kidney transplants in Iran including 1,501 living donors and 1,169 deceased donors.[14] Although kidney transplantation in Iran started from living-related donors, currently the main source of kidney donations is living nonrelated donors.[2] Analyzing renal transplantation data can help to evaluate the effectiveness of transplantation activities and estimation of future costs in the health care system.[12] Several studies have been conducted to estimate the survival rate of renal transplantation in different transplantation centers of Iran such as Tehran,[8] Shiraz,[15,16,17] Mashhad,[18] Hamadan,[19] but there is no any study about the survival rate in patients of one city who had undergone kidney transplantation in other centers. Therefore, the aim of this study was to determine the organ survival rate after kidney transplantation during a period of 10 years (March 2001-March 2011) in transplanted patients from Arak, Markazi Province, Iran.
MATERIALS AND METHODS
Study design and participants
In this historical cohort study, all recipients of kidney transplantation from Arak, in all transplant centers of Iran who have medical records in Valiasr Hospital and “charity for kidney patients” of Arak, Markazi Province, Iran during a period of 10 years from March 2001 to March 2011 were included. In this period, 225 cases of transplantation, out of which 189 from living donors and 36 from deceased donors were performed. Data collected by using checklists were completed from patients’ hospital records. In this study, the exact time of transplantation was considered as the “initial event” and the time of irreversible transplant rejection leading to a return to dialysis was defined as the “end-point event.” Cases in which didn’t experienced this event due to finishing the study, the patients who were lost to follow-up, or who died for reasons other than transplant rejection were considered as “censored data.” Deaths due to surgical consequences immediately after surgery were excluded.
There was no ethical problem in this research because the data were extracted from patient records without mentioning the name, and there was no any intervention on the patient. The research proposal was approved by the Deputy of Research of Arak University of Medical Sciences with project number 1063 and the Ethics Committee with ethics number 92-160-14.
Study's variables
The studied variables were donor source (deceased, related, unrelated), donor and recipient's age, gender, recipient's place of residency (city, rural), family history of kidney transplantation, marital status (single, married, widow), blood group (A, B, AB, O), Rh (positive, negative), underlying cause of ESRD (diabetes, glomerulonephritis, hypertension, kidney poly cystic, other), and the number of dialysis after transplantation in 1 week.
Statistical analysis
The obtained data were analyzed using Statistical Package for the Social Sciences (SPSS) 20 and Stata 11 (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp). Kaplan-Meier method was employed to determine the graft cumulative survival rate, log-rank test to compare survival curves in subgroups, and Cox regression model to define the hazard ratio and for ruling out the intervening factors. The proportional hazards assumption for all variables was checked using the estat phtest,[20] and the results confirmed this assumption.
RESULTS
In this study, among the 225 patients followed up over 10 years, 30 cases (13.3%) of irreversible transplant rejection that led to the initiation of dialysis or death was observed. 214 (95.11%) out of 225 patients were followed successfully until the end of the study. The mean age of the kidney donors and recipients was 28.78 ± 5.23 years and 36.42 ± 14.34 years, respectively. The other variables are presented in Table 1.
Table 1.
Frequency distribution of demographic and clinical variables in study

The mean duration of follow-up was 55.43 ± 42.02 months and the time at risk in the study was 12471.5 person-months. The mean of entry and exit time was 0 months and 55.68 months, respectively. As shown in Figure 1, by using the Kaplan-Meier method, the cumulative probability of graft survival and 95% confidence interval (CI) at 1, 3, 5, 7, and 10 years after transplantation were 99.10 (96.45-99.77), 97.72 (93.89-99.16), 94.33 (88.74-97.18), 85.66 (77.27-91.13), and 62.12 (48.45-73.15)%, respectively.
Figure 1.

Graft survival rate in renal transplant recipients from Arak, 2001-2011
As shown in Table 2, based on the log-rank test results, the recipients’ gender showed a significant relationship with the cumulative survival rate of kidney transplantation such that survival was significantly higher in female recipients compared with male recipients (P = 0.02). The recipient age was one of the affecting factors of survival so that survival in the age group of 21-40 years was significantly high and in the age group above 60 years was low (P < 0.001). Also, in terms of the underlying cause of ESRD, survival was significantly lower in diabetes and glomerulonephritis groups (P = 0.01). In the present study, kidney survival rate has not been significantly different in terms of following factors: donor's gender (P = 0.31), donor's age (P = 0.69), donor's source (P = 0.47), recipient's Rh (P = 0.14), recipient's residency (P = 0.41), recipient's family history (P = 0.38), recipient's marital status (P = 0.24), and recipient blood group (P = 0.29).
Table 2.
Comparison of survival rates at different time intervals including 1 year, 3 years, 5 years, 7 years, and 10 years after kidney transplantation in studied variables

Univariate Cox regression model was used to determine the affecting quantitative variables on the kidney rejection that not entered in log-rank test. Based on the results of univariate Cox regression, the number of dialysis was significantly associated with cumulative probability of survival [hazard ratios and 95% CI: 1.71 (1.21-2.40)] so that for every one unit increase in the number of dialysis after transplantation, the hazard ratio of kidney transplantation rejection increased 1.71 times. The recipient's weight was not significantly associated with cumulative probability of survival [hazard ratios and 95% CI: 0.99 (0.96-1.01)].
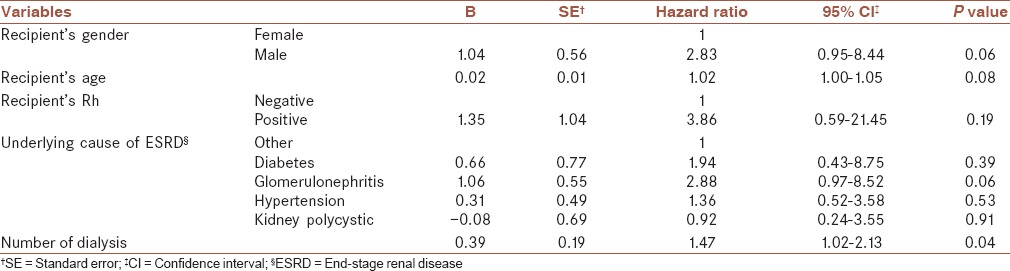
Finally, in order to have a multivariate analysis and determination of the affecting variables on the kidney rejection, multivariate Cox regression models were used. At this point, the variables that had a P value ≤0.2 in univariate analysis were entered into the model. Results show that only the number of dialysis by controlling the effect of other variables had a significant association with the risk of kidney transplant rejection [Table 3].
Table 3.
Multivariate analysis by Cox regression model for affecting variables on the kidney rejection
DISCUSSION
This study showed that graft survival rates at 1 year, 3 years, 5 years, 7 years, and 10 years after transplantation in transplanted patients from Arak city, Markazi Province, Iran were 99.1, 97.7, 94.3, 85.7, and 62.1%, respectively.
Based on the report of Iran organ procurement network, the 1-year survival rate of kidney transplantation has been reported to be 94.7%.[17] In contrast, this rate is higher in our studied patients. Based on the results of the largest survival analysis in the country, so far 1-, 5-, 10-, and 15-year graft survival rates were 85%, 68%, 46%, and 24%, respectively.[21,22] In the studies that were conducted in 2010 at the Shiraz Transplant Center, the survival rates for these intervals from the deceased donor were 96.6%, 93.7%, 88.9%, 87.1%, and 85.8%, respectively, and from the living donor were 98.3%, 96.4%, 92.5%, 90.8%, and 89.2%, respectively;[15,17] the survival rate at intervals of 1 year, 3 years, and 5 years was less than our study but on the contrary, at intervals of 7 years and 10 years it was greater. In the study of Javanrouh Givi et al. in Mashhad Qaem Hospital, 1-, 5-, and 10-year survival rates were estimated to be 98.3, 92.5, and 89.2%, respectively.[18] In another study that was conducted in Tehran, Tehran Province, Iran in 2011, the survival rates at 1 month, 1 year, and 5 years after transplantation were 93.2%, 89% and 82.5%, respectively,[8] and the survival rate was lower than our study. In a study in Taiwan the 5-year survival rate of kidney transplantation was estimated to be 84.7% that was lower than our study.[23] Saatchi et al. conducted a retrospective cohort study in Hamadan Province on 475 patients who had undergone kidney transplantation from 1994 to 2011; they found that 1-, 5-, 10-, 15-, and 18-year survival rates of transplantation were 97.1%, 92.3%, 86.2%, 77.6%, and 60.3%, respectively.[19] Kwon et al. conducted a similar study in South Korea on 614 patients and reported that 1-, 5-, and 10-year survival rates of kidney transplantation patients were 92.62%, 82.37%, and 76.07%, respectively.[24] Based on the results of a single-center experience from Turkey, 1-year graft survival rates were estimated to be 99.3% and 95.8% in the preemptive and nonpreemptive transplantation groups, respectively.[25] In general, the observed differences on the one hand could be due to lack of synchronicity in these studies and changes in transplantation techniques or prescription drugs and type of immunosuppressive regimen for patients during the time while on the other hand they could be due to the nonuniform experience of transplant centers and physicians. Also, this inconsistency could be attributed to the study setting, individual characteristics, and clinical status of the patients.[19]
In this study, in univariate model the cumulative probability of survival was significantly higher in female recipients compared to male recipients. This was consistent with the study of Chen et al. in Taiwan[23] but was different from the study of Hassanzadeh et al.[17] The higher survival rate in women could be due to hormonal or immunological changes in them,[26] However, this association was not significant after adjustment for the effect of other variables. A recent study has confirmed this issue and concluded that the association between graft rejection and sex was confounded by other variables.[19] The donor's gender showed no association with survival rate and this finding was consistent with the results of many studies[15,23,27,28,29] while in some studies graft failure has been reported to be higher in women donors that has been attributed to lower body weight and fewer nephrons in women.[17]
In the present study, there was no significant association between the age of donors and survival rate of transplantation while the results of many studies and the literature review shows the negative effect of age on the cumulative probability survival of kidney transplantation.[15,30,31] This negative effect attributes to the structural changes of the elderly renal parenchyma and also, inadequacy of the nephrons of elderly graft to fulfill the functional requirements of a poorly equipped recipient.[21,32] However, survival in recipients aged 21-40 years was significantly high while in the age groups of above 60 years and below 20 years it was low, which was consistent with the results of many existing studies.[15,33,34,35] The relationship between the recipient's age and graft survival in young subjects is justifiable due to their small anatomical body parts and probability of the existence of technical problems, and in the older subject can be explained by loss of nephron function.[15]
In this study, no association was observed between the donor sources (deceased, living-related, living-unrelated) with the probability of graft survival while in the study of Almasi-Hashiani et al., the percentage of irreversible rejections, which led to the initiation of dialysis in the cases of transplantation from deceased donors was more.[16] Also, this finding has been confirmed in other studies,[13,33,36] which may have been caused by differences in the transmission system of donated organs or could have been due to cold ischemia time of the kidney since increasing the time of ischemia resulted in decreased graft survival.[17,37] The absence of association in our study might have been due to the low sample size.
In this study similar to most of the existing studies,[17,27,28] there was no association between the underlying cause of ESRD and graft survival. However, based on the study results of Courtney et al.[33] the underlying cause of ESRD may influence the survival time.
In the present study, dialysis time after transplantation had a significant effect on the survival of renal transplantation after adjusting the effect of other variables. Based on the results of other studies, the waiting time on dialysis before transplantation was one of the largest independent risk factors for graft loss after kidney transplantation.[18,27,38]
The strength of this study was successful follow-up of survival rate of more than 95% of the patients while its major limitations were low sample size and conducting a retrospective cohort study and using medical records instead of prospective design. The lack of accurate registration of some factors such as creatinine in the patient's records did not allow assessment of the effect of these variables. Also, we were unable to survey the effect of immunosuppressive drugs.
CONCLUSION
In this study, 1-, 3-, 5-, 7-, and 10-year graft survival rates were satisfactory and similar to the results of single center studies in the world. Dialysis time after transplantation was a significant predictor of survival in recipients of kidney transplantation this issue should be considered during kidney transplant in order to increase the survival.
Financial support and sponsorship
Arak University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
AUTHORS’ CONTRIBUTION
MR designed and conducted the research, performed the statistical analyses, participated in all of the research, and prepared the manuscript. FS and SK designed and conducted the research, collected the data, and participated in the manuscript preparation. HS corrected the English manuscript, revised further statistical data, and participated in manuscript preparation. HJ provided assistance in conducting the research, and participated in data-gathering and manuscript preparation. All the authors have read and approved the content of the manuscript.
Acknowledgements
The authors wish to acknowledge the Deputy of Research of Arak University of Medical Sciences for approval and financial support of this research project as well as the dialysis unit staff of Valiasr Hospital and charity supporting kidney patients of Arak city, Markazi Province, Iran.
REFERENCES
- 1.Couser WG, Remuzzi G, Mendis S, Tonelli M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011;80:1258–70. doi: 10.1038/ki.2011.368. [DOI] [PubMed] [Google Scholar]
- 2.Mousavi SS, Soleimani A, Mousavi MB. Epidemiology of end-stage renal disease in Iran: A review article. Saudi J Kidney Dis Transpl. 2014;25:697–702. doi: 10.4103/1319-2442.132242. [DOI] [PubMed] [Google Scholar]
- 3.Mahdavi-Mazdeh M, Zamyadi M, Nafar M. Assessment of management and treatment responses in haemodialysis patients from Tehran province, Iran. Nephrol Dial Transplant. 2008;23:288–93. doi: 10.1093/ndt/gfm580. [DOI] [PubMed] [Google Scholar]
- 4.Mahdavi-Mazdeh M, Heidary Rouchi A, Norouzi S, Aghighi M, Rajolani H, Ahrabi S. Renal replacement therapy in Iran. Urol J. 2007;4:66–70. [PubMed] [Google Scholar]
- 5.Najafi I, Hakemi M, Safari S, Atabak S, Sanadgol H, Nouri-Majalan N, et al. The story of continuous ambulatory peritoneal dialysis in Iran. Perit Dial Int. 2010;30:430–3. doi: 10.3747/pdi.2008.00235. [DOI] [PubMed] [Google Scholar]
- 6.Aghighi M, Heidary Rouchi A, Zamyadi M, Mahdavi-Mazdeh M, Rajolani H, Ahrabi S, et al. Dialysis in Iran. Iran J Kidney Dis. 2008;2:11–5. [PubMed] [Google Scholar]
- 7.Ghods AJ. Renal transplantation in Iran. Nephrol Dial Transplant. 2002;17:222–8. doi: 10.1093/ndt/17.2.222. [DOI] [PubMed] [Google Scholar]
- 8.Ghanei E, Nasrolahi A, Razaghi M. Evaluation Short and Long term graft and survival rates in kidney transplanted patients between 1995-2011. J Army Univ Med Sci. 2012;9:251–5. [Google Scholar]
- 9.Peroviæ S, Jankoviæ S. Renal transplantation vs hemodialysis: Cost-effectiveness analysis. Vojnosanit Pregl. 2009;66:639–44. doi: 10.2298/vsp0908639p. [DOI] [PubMed] [Google Scholar]
- 10.Hashiani AA, Rajaeefard A, Hasanzadeh J, Kakaei F, Behbahan AG, Nikeghbalian S, et al. Ten-year graft survival of deceased-donor kidney transplantation: A single-center experience. Ren Fail. 2010;32:440–7. doi: 10.3109/08860221003650347. [DOI] [PubMed] [Google Scholar]
- 11.Ghods A. The history of organ donation and transplantation in Iran. Exp Clin Transplant. 2014;12(Supp 1):38–41. doi: 10.6002/ect.25liver.l29. [DOI] [PubMed] [Google Scholar]
- 12.Noorbala MH, Rafati-Shaldehi H, Azizabadi-Farahani M, Assari S. Renal transplantation in iran over the past two decades: A trend analysis. Transplant Proc. 2007;39:923–6. doi: 10.1016/j.transproceed.2007.03.094. [DOI] [PubMed] [Google Scholar]
- 13.Legendre C, Canaud G, Martinez F. Factors influencing long-term outcome after kidney transplantation. Transpl Int. 2014;27:19–27. doi: 10.1111/tri.12217. [DOI] [PubMed] [Google Scholar]
- 14.International Registry in Organ Donation and Transplantation — IRODaT. [Last accessed on 2014 Jun 6]. Available from: http://www.irodat.org/
- 15.Almasi Hashiani A, Rajaeefard A, Hassanzade J, Salahi H. Survival analysis of renal transplantation and its relationship with age and sex. Koomesh. 2010;11:302–6. [Google Scholar]
- 16.Almasi-Hashiani A, Hassan Zaede J, Rajaee Fard A, Salahi Ho. The relationship between graft survival rate of renal transplantation and donor source in transplanted patients at the transplantation center of Namazi Hospital of Shiraz. J Arak Univ Med Sci. 2011;14:10–7. [Google Scholar]
- 17.Hassanzadeh J, Hashiani AA, Rajaeefard A, Salahi H, Khedmati E, Kakaei F, et al. Long-term survival of living donor renal transplants: A single center study. Indian J Nephrol. 2010;20:179–84. doi: 10.4103/0971-4065.73439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Javanrouh Givi N, Alimi R, Esmaily H, Shakeri MT, Shamsa A. Assessment of effective factors on renal transplantation survival and estimation of rejection hazard for transplanted in Mashhad Qaem hospital. J North Khorasan Univ Med Sci. 2013;5:315–21. [Google Scholar]
- 19.Saatchi M, Poorolajal J, Amirzargar MA, Mahjub H, Esmailnasab N. Long-term survival rate of kidney graft and associated prognostic factors: A retrospective cohort study, 1994-2011. Ann Transplant. 2013;18:153–60. doi: 10.12659/AOT.883873. [DOI] [PubMed] [Google Scholar]
- 20.Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81:515–26. [Google Scholar]
- 21.Einollahi B, Pourfarziani V, Ahmadzad-Asl M, Davoudi F, Lessan-Pezeshki M, Davoudi A, et al. Iranian model of renal allograft transplantation in 3028 recipients: Survival and risk factors. Transplant Proc. 2007;39:907–10. doi: 10.1016/j.transproceed.2007.03.033. [DOI] [PubMed] [Google Scholar]
- 22.Einollahi B, Bahaeloo-Horeh S, Assari S, Ghanei M. Iranian kidney transplantation society seeks to answer its questions through a link between scientists and young researchers. Saudi J Kidney Dis Transpl. 2008;19:1015–9. [PubMed] [Google Scholar]
- 23.Chen PD, Tsai MK, Lee CY, Yang CY, Hu RH, Lee PH, et al. Gender differences in renal transplant graft survival. J Formos Med Assoc. 2013;112:783–8. doi: 10.1016/j.jfma.2013.10.011. [DOI] [PubMed] [Google Scholar]
- 24.Kwon OJ, Kwak JY, Kang CM. The impact of sex and age matching for long-term graft survival in living donor renal transplantation. Transplant Proc. 2005;37:726–8. doi: 10.1016/j.transproceed.2004.12.137. [DOI] [PubMed] [Google Scholar]
- 25.Bozkurt B, Kumru AÖ, Dumlu EG, Tokaç M, Koçak H, Süleymanlar G, et al. Patient and graft survival after pre-emptive versus non-pre-emptive kidney transplantation: A single-center experience from turkey. Transplant Proc. 2013;45:932–4. doi: 10.1016/j.transproceed.2013.02.064. [DOI] [PubMed] [Google Scholar]
- 26.Meier-Kriesche HU, Ojo AO, Leavey SF, Hanson JA, Leichtman AB, Magee JC, et al. Gender differences in the risk for chronic renal allograft failure. Transplantation. 2001;71:429–32. doi: 10.1097/00007890-200102150-00016. [DOI] [PubMed] [Google Scholar]
- 27.Briganti EM, Wolfe R, Russ GR, Eris JM, Walker RG, McNeil JJ. Graft loss following renal transplantation in Australia: Is there a centre effect? Nephrol Dial Transplant. 2002;17:1099–104. doi: 10.1093/ndt/17.6.1099. [DOI] [PubMed] [Google Scholar]
- 28.El-Husseini AA, Foda MA, Shokeir AA, Shehab El-Din AB, Sobh MA, Ghoneim MA, et al. Determinants of graft survival in pediatric and adolescent live donor kidney transplant recipients: A single center experience. Pediatr Transplant. 2005;9:763–9. doi: 10.1111/j.1399-3046.2005.00376.x. [DOI] [PubMed] [Google Scholar]
- 29.Tang H, Chelamcharla M, Baird BC, Shihab FS, Koford JK, Goldfarb-Rumyantzev AS. Factors affecting kidney-transplant outcome in recipients with lupus nephritis. Clin Transplant. 2008;22:263–72. doi: 10.1111/j.1399-0012.2007.00781.x. [DOI] [PubMed] [Google Scholar]
- 30.Barba Abad J, Tolosa Eizaguirre E, Rincón Mayans A, Rosell Costa D, Robles García J, Zudaire Bergera J, et al. Influence of donor age on graft survival. Actas Urol Esp. 2010;34:719–25. [PubMed] [Google Scholar]
- 31.Pascual J, Zamora J, Pirsch JD. A systematic review of kidney transplantation from expanded criteria donors. Am J Kidney Dis. 2008;52:553–86. doi: 10.1053/j.ajkd.2008.06.005. [DOI] [PubMed] [Google Scholar]
- 32.Hiesse C, Pessione F, Cohen S. Kidney grafts from elderly donors. Presse Med. 2003;32:942–51. [PubMed] [Google Scholar]
- 33.Courtney A, McNamee P, Maxwell A. The evolution of renal transplantation in clinical practice: For better, for worse? QJM. 2008;101:967–78. doi: 10.1093/qjmed/hcn136. [DOI] [PubMed] [Google Scholar]
- 34.Orsenigo E, Socci C, Carlucci M, Zuber V, Fiorina P, Gavazzi F, et al. Multivariate analysis of factors affecting patient and graft survival after renal transplant. Transplant Proc. 2005;37:2461–3. doi: 10.1016/j.transproceed.2005.06.099. [DOI] [PubMed] [Google Scholar]
- 35.Knoll GA. Kidney transplantation in the older adult. Am J Kidney Dis. 2013;61:790–7. doi: 10.1053/j.ajkd.2012.08.049. [DOI] [PubMed] [Google Scholar]
- 36.Bakr MA, Ghoneim MA. Living donor renal transplantation, 1976-2003: The mansoura experience. Saudi J Kidney Dis Transpl. 2005;16:573–83. [PubMed] [Google Scholar]
- 37.Kaplan B, Schold JD, Meier-Kriesche HU. Long-term graft survival with neoral and tacrolimus: A paired kidney analysis. J Am Soc Nephrol. 2003;14:2980–4. doi: 10.1097/01.asn.0000095250.92361.d5. [DOI] [PubMed] [Google Scholar]
- 38.Meier-Kriesche HU, Kaplan B. Waiting time on dialysis as the strongest modifiable risk factor for renal transplant outcomes: A paired donor kidney analysis 1. Transplantation. 2002;74:1377–81. doi: 10.1097/00007890-200211270-00005. [DOI] [PubMed] [Google Scholar]