

Abstract
Despite the huge body of research on social support, literature has been primarily focused on its beneficial role for both physical and mental health. It is still unclear why people with mental and neurological disorders experience low levels of social support. The main objective of this study was to explore what are the strongest factors related to social support and how do they interact with each other in neuropsychiatric disorders. The study used cross-sectional data from 722 persons suffering from dementia, depression, epilepsy, migraine, multiple sclerosis, Parkinson's disease, schizophrenia, stroke, and substance use disorders. Multiple linear regressions showed that disability was the strongest factor for social support. Extraversion and agreeableness were significant personality variables, but when the interaction terms between personality traits and disability were included, disability remained the only significant variable. Moreover, level of disability mediated the relationship between personality (extraversion and agreeableness) and level of social support. Moderation analysis revealed that people that had mental disorders experienced lower levels of support when being highly disabled compared to people with neurological disorders. Unlike previous literature, focused on increasing social support as the origin of improving disability, this study suggested that interventions improving day-to-day functioning or maladaptive personality styles might also have an effect on the way people perceive social support. Future longitudinal research, however, is warranted to explore causality.
Introduction
The concept of social support varies from objective social life (group memberships, family, spouse, etc.) to subjective experience (e.g., emotional support, loneliness). Research on social support has primarily focused on its protective role against the negative effects of stressful life events or its positive impact on psychological well-being, mortality and disease severity [1–5]. Lower social support has been associated with poor treatment outcomes [6] and has predicted higher health care utilization in mental disorders [7]. Enhancement of social support has been recommended as an important part of the treatment for mental and neurological disorders [8].
Some studies agree that people with neuropsychiatric disorders have smaller and poor quality social networks [5, 9–11]. Literature so far has investigated certain personality, disease and disability related factors as potential variables explaining this phenomenon. On one hand, studies in some neuropsychiatric disorders have shown associations between personality types and level of social support [12]. More specifically, three of the “Big Five” personality traits—extraversion, agreeableness and conscientiousness have shown positive correlation with variables related to social support in depression, whereas a negative correlation has been found for neuroticism and openness [13]. Furthermore, association between gender and social support is evident in epilepsy [14], whereas quality of life has shown significant relation with social support in schizophrenia [15]. However, many personality related variables like resilience, or socio-demographic factors such as level of education, marital status or age, are still under-researched as potential factors for social support in number of neuropsychiatric conditions.
Another line in research postulates that certain disability or disease-specific factors might be also associated with social support. High functional disability has been associated with lower social support in depression [16] and migraine [17]. Social support has also moderated the relationship between depressive symptoms and functional disability. Adults with higher functional impairment benefited less from increased social support in the context of higher symptom severity in depression [7, 18, 19].
Despite all published studies so far, there are still four issues that remain unresolved. First, literature exploring social support as dependent variable is scarce. Many relevant personality disability and disease-specific factors for social support are under-researched. Although some evidence mainly on the independent effect of personality and disability in neurological and mental disorders exists, it is somehow limited and focuses mainly on one single condition. Second, we still do not know which the most important factor for social support is. Personality, clinical and disability factors included in a single model have not been studied. Third, no study has analyzed whether the interaction effect of personality and health condition related factors is stronger than these factors alone. Moreover, no mediation effects have been explored. Finally, social support in mental and neurological disorders has not been compared so far. It is still unknown whether people with mental disorders experience different levels of social support compared to neurological disorder when the level of functioning is included in the interaction.
In attempt to address all these issues and investigate why people with neuropsychiatric disorders experience poor social support, this study aimed to explore 1) what are the strongest factors related to social support in neuropsychiatric disorders, 2), whether there is a specific interaction between the most important personality and health related factors for social support 3) whether the level of disability mediates the relationship between personality and social support and 4) whether type of health condition (mental or neurological) is a moderator between level of disability and social support.
Methods
Procedure
This cross-sectional study was carried out using data from the European Union (EU) funded coordinated project “Psychosocial fActors Relevant to brAin DISorders in Europe (PARADISE)” [20], (http://paradiseproject.eu/). The study was conducted according to the ethical principles of the European Commission (EC) Research Ethics Committee and approved by the Ethics Committee of the Ludwig-Maximilian University, Munich, Germany, as a coordinating center, and by the local Ethics Committees of each recruiting institution.
Sample
Data was gathered from 722 participants: patients with stroke (n = 80), multiple sclerosis (n = 80), epilepsy (n = 80), migraine (n = 80) and Parkinson Disease (n = 80) were recruited at the Neurological Institute Carlo Besta IRCCS Foundation in Milan, Italy, while patients with dementia (n = 80) and schizophrenia (n = 81) were recruited at the Institute of Psychiatry and Neurology in Warsaw, Poland; finally, patients with depressive disorders (n = 81) and substance-use disorders (n = 80) were recruited, respectively, at La Princesa University Hospital in Madrid, Spain, and the Järvenpää Addiction Hospital in Järvenpää, Finland.
The participants were referred by their main health professionals. All the interviews were face to face and conducted by mental health professionals trained to use the PARADISE protocol. The inclusion criteria were broad in order to catch the full range of psychosocial difficulties experienced by individuals: ≥ 18 years of age and a main diagnosis established according to ICD-10 [21]. The majority of patients had comorbid disorders, some of which among the ones included in this study, but this was not a reason for exclusion. Every patient was listed in one of the nine groups of disorders according to his primary diagnosis. Participants were informed of the rationale of the study and asked to sign an informed consent form. For sufferers of dementia not able to provide consent, caregivers were asked to do it and participate in the interviews as proxies.
Measures
Since a global score was obtained for each of the scales considered in the study, Confirmatory Factor Analyses (CFA) were conducted in order to obtain evidence for one-factor solutions and to assume unidimensionality before obtaining these global scores. Goodness-of-fit of the proposed model was evaluated according to the standard recommendations [22, 23]. Values of the Comparative Fit Index (CFI) above 0.90 were considered to represent an adequate fit; values of Root Mean Square Error of Approximation (RMSEA) less than 0.08 indicated a good fit [24].
Social support was measured using the Oslo 3-item Social Support Scale [25], covering three items on primary support group (“How many people are you so close to that you can count on them if you have great personal problems?”), interest and concern shown by others (“How much interest and concern do people show in what you do?”), and ease of obtaining practical help (“How easy is it to get practical help from neighbors if you should need it?”). The instrument has been used in various studies thus proving its feasibility [26]. A global score was created by adding up the raw scores, ranging from 3 to 14 with higher scores indicating higher social support. Since this instrument comprised three items, the overall fit of a one-factor model could not be ascertained because there were no degrees of freedom. However, the three items representing social support had significant loadings on the latent construct (factor loadings higher than .45). This finding suggests that the three items of the scale represent social support and a global score can be obtained from these three items.
Disability was assessed by World Health Organization Disability Assessment Schedule short-form 12 (WHODAS-12) [27]. The questionnaire measures global disability and is suitable for epidemiological studies and outcome assessments. Its psychometric properties have been measured in dozens of studies in diverse cross-cultural settings [28, 29]. The total score ranges between 0 and 100 as higher scores indicate higher levels of disability, i.e., lower levels of functioning. A CFA was performed over the WHODAS items on the overall sample and evidence for a one-factor solution was found (CFI = 0.961, RMSEA = 0.067).
Another instrument developed by WHO (EUROHIS-QOL 8-item index) was used to measure the quality of life [30]. It is a shortened version of the World Health Organization Quality of Life Instrument-Abbreviated Version (WHOQOL-BREF). It was designed as a short and concise instrument of eight items reporting subjective well-being and satisfaction with different life aspects. Psychological, social, physical and environmental domains were assessed each with two items. The overall quality of life score is formed by the sum of the scores of the eight items, with higher scores indicating better quality of life. EUROHIS-QOL has also shown adequate cross-cultural validity [31]. A CFA was conducted in order to test the unidimensionality of the eight items of the EUROHIS-QOL. The CFA performed on the overall sample presented acceptable values in the goodness-of-fit indices: CFI = 0.978 and RMSEA = 0.063.
Resilience was assessed with the Brief Resilient Coping Scale [32]. The questionnaire was designed to capture tendencies of individuals to cope with stress. The instrument captures the following themes: tenacity, optimism, creativity, an aggressive approach to problem solving, and commitment to positive growth from difficult situations. The questionnaire has 4 items giving a range of 4–20 with higher scores indicating higher resilience. The CFA performed on the overall sample provided support for a one-factor solution: CFI = 0.983 and RMSEA = 0.025.
Personality style was measured with the short version of the Big Five Inventory (BFI), BFI-10 [33, 34]. The instrument is a self-report inventory designed to measure the Big Five personality dimensions—conscientiousness, agreeableness, neuroticism, extraversion and openness. It consists of 10 items in total (2 for each personality trait) and has been previously used in a number of studies [35].
Severity of symptoms was a composite variable. The severity score of each disease, measured by a previously used instrument, was combined in one new variable. The new severity of symptoms index variable was created according to three previously established cut-off points (mild, moderate and severe), amalgamating scores for depression (Hamilton Depression Rating Scale (HAM-D; [36]); dementia (Mini-Mental State Examination (MMSE; [37]); migraine (The Migraine Disability Assessment Test (MIDAS); [38]); multiple sclerosis (Expanded Disability Status Scale (EDSS); [39, 40]; Parkinson’s disease (Hoehn & Yahr Staging scale; [41]); schizophrenia (Brief Psychiatric Rating Scale (BPRS); [42]); stroke (National Institutes of Health Stroke Scale (NIHSS); [43]) and alcohol dependence (Alcohol Dependence Scale (ADS); [44]. Data on substance use disorders was collected with the ‘Severity of Dependence Scale’ and the “Alcohol Dependence Scale (ADS)”. Our intention was to use the collected data from the ‘Severity of Dependence Scale’, but due to the large number of missing data we report here only the alcohol dependent participants, filled out the ADS questionnaire.
Comorbidity was assessed with Self-reported Comorbidities Questionnaire (SCQ) [45]. The summary score represents the addition up to three points derived from each reported health condition: a point for its presence, point if treatment is received, and point if it causes decrements in functioning. Demographic variables such as gender, age, education and marital status were included in the analysis.
Statistical analysis
First, descriptive statistics were obtained, including summary of the socio-demographic data of the participants and means and standard deviations (SDs) of the survey scale scores. Second, a multiple linear regression analysis was conducted to explore the relationships between the two groups of independent variables considered: personality related variables (personality type, resilience, quality of life, gender, age, education and marital status) and health condition related factors (disability, severity of symptoms, and comorbidity) and the score of social support. All the independent variables were introduced simultaneously in the model because we were exploring potential predictors of social support rather than comparing them or introducing previously established models. The ordinary least squares (OLS) estimation was employed; the use of OLS trades robustness for some improvement in efficiency [46] and has been shown to yield the best fit of data [47]. Beta coefficients were reported and can be interpreted as change in the outcome (in standard deviations) per standard deviation change in the predictors; they were used to assess which variables had the highest association with the outcome variable. 95% confidence intervals (CI) were reported.
We assessed three regression models. The first model included all the independent variables. In the second model, dummy variables for type of health condition (dementia, epilepsy, migraine, multiple sclerosis, Parkinson, schizophrenia, stroke and substance use disorders) were added to check for their association with social support and to control for their potential effect. In a third model, the interaction terms between the most significant personality and health condition related factors were added to model 2. Since we entered multiple independent variables, the presence of multicollinearity was assessed by means of the Variance Inflation Factor (VIF). Values below 5 have been considered adequate [48].
Mediation and moderation analyses were conducted, respectively, to: 1) assess if disability mediates the relationship between the personality traits which were found significant on the previous regression models and social support; 2) assess if the relationship between disability and social support is moderated by the type of health condition (mental vs. neurological). In each mediation analysis, two linear regression models were considered: one for the relationship between the independent and the mediating variable, and another for the relationship between the mediating and the dependent variable. In the moderation analysis, the interaction term (the independent multiplied by the moderating variable) was calculated, and then by means of a "simple slope" analysis was assessed whether the gradient of both lines for mental and neurological conditions differed from 0. All the health conditions were merged into two groups: mental (depression, substance use disorders, schizophrenia) and neurological health conditions (dementia, epilepsy, migraine, multiple sclerosis, Parkinson’s disease and stroke).
SPSS 21.0 software [49] was used to analyse socio-demographic data and to conduct the regression models. For testing mediation, online MedGraph programme was used to compute the correlations and regressions [50]. We introduced the values of the unstandardized regression coefficients and standard errors of path a and path b to MedGraph. Path a represents the unstandardized regression coefficient for the path from the independent variable (personality type) to mediating variable (disability); path b is the coefficient for the path from the mediating variable (disability) to the dependent variable (social support) controlling for the independent variable. Sobel’s z-score and p-values for significance were then computed. Indirect to Total ratio was also computed, reporting the estimated size of the indirect effect in relation to the total effect. The indirect to total ratio explains the amount of variance in the relationship between the independent and the dependent variables which is due to the mediation variable. Values fall between .00 and 1.00, with higher values indicating higher relative indirect effects [51]. For the moderation analysis the process was identical and conducted by means of the online ModGraph programme [52].
Results
Descriptive statistics
Demographics, socio-economic and clinical characteristics are presented in Table 1. The mean age of the total sample was 51.29 years (SD = 14.25). There were a similar proportion of men and women, and most of the participants had at least completed high school. A greater number of people with epilepsy, migraine and multiple sclerosis were still working despite their condition. In some conditions like schizophrenia and substance use disorders people were not employed although they were younger. As for the clinical characteristics, people with depression and substance use disorders showed the greatest number of comorbid conditions. Table 1 shows descriptively that the level of social support and quality of life among the conditions was relatively equal, but people suffering from depression, schizophrenia and substance use disorders had a higher result on the disability scale.
Table 1. Demographic, socio-economic and clinical characteristics of the sample.
| Epilepsy | Migraine | Multiple Sclerosis | Parkinson | Stroke | Dementia | Depression | Schizophrenia | Substance Use | |
|---|---|---|---|---|---|---|---|---|---|
| N | 80 | 80 | 80 | 80 | 80 | 80 | 81 | 81 | 80 |
| Age (years) | |||||||||
| Mean (SD) | 41.23 (11.99) | 44.54 (12.12) | 41.03 (8.74) | 61.24 (10.45) | 59.84 (14.36) | 81.03 (5.49) | 54.81 (14.73) | 38.38 (14.03) | 39.56 (13.15) |
| Gender (%) | |||||||||
| Female | 50.0 | 86.3 | 65.0 | 40.0 | 43.8 | 78.8 | 82.7 | 53.1 | 37.5 |
| Marital status (N) | |||||||||
| Married or in a relationship | 42 | 53 | 50 | 65 | 62 | 25 | 37 | 10 | 29 |
| Not married | 38 | 27 | 30 | 15 | 18 | 55 | 44 | 71 | 51 |
| Less than primary school | 0.0 | 0.0 | 1.3 | 1.3 | 0.0 | 3.8 | 17.3 | 0.0 | 3.8 |
| Primary school completed | 1.3 | 1.3 | 1.3 | 13.8 | 22.5 | 18.8 | 16.0 | 4.9 | 35.0 |
| Education (%) | |||||||||
| Secondary school completed | 28.8 | 18.8 | 23.8 | 26.3 | 22.5 | 3.8 | 11.1 | 4.9 | 32.5 |
| High school completed | 50.0 | 48.8 | 51.3 | 43.8 | 40.0 | 40.0 | 17.3 | 44.4 | 17.5 |
| University or postgraduate degree completed | 20.0 | 31.3 | 22.5 | 15.1 | 10.0 | 33.8 | 38.3 | 45.7 | 11.3 |
| Working sample (%) | 66.3 | 67.5 | 72.5 | 33.8 | 25.0 | 0.0 | 27.2 | 8.6 | 6.3 |
| Disease duration (years) | |||||||||
| Mean (SD) | 18.67 (12.32) | 21.13 (14.60) | 7.66 (6.94) | 6.26 (4.40) | 4.00 (6.48) | 3.69 (2.70) | 12.63 (11.57) | 13.03 (11.83) | 12.16 (8.67) |
| Comorbidity score (SCQ score) | |||||||||
| Mean (SD) | 2.36 (2.97) | 2.36 (2.55) | 1.18 (2.17) | 3.00 (2.63) | 5.87 (4.87) | 5.86 (4.17) | 12.56 (5.09) | 2.72 (3.14) | 8.84 (4.76) |
| Social Support (OSS) | |||||||||
| Mean (SD) | 10.92 (1.32) | 10.05 (2.30) | 10.46 (2.05) | 10.02 (1.99) | 10.32 (1.49) | 9.45 (2.18) | 10.09 (2.55) | 8.93 (2.63) | 9.64 (2.04) |
| Quality of Life (WHOQOL) | |||||||||
| Mean (SD) | 14.02 (2.31) | 14.30 (2.61) | 13.43 (2.47) | 14.43 (2.22) | 13.80 (2.48) | 15.27 (2.12) | 16.41 (3.05) | 15.15 (2.81) | 14.40 (2.67) |
| Extraversion | |||||||||
| Mean (SD) | 2.98 (0.88) | 3.02 (1.09) | 3.28 (1.01) | 2.90 (0.94) | 3.05 (0.88) | 3.14 (0.84) | 3.16 (1.33) | 2.89 (1.03) | 3.11 (1.02) |
| Agreeableness | |||||||||
| Mean (SD) | 3.57 (0.71) | 3.66 (0.89) | 3.80 (0.90) | 4.01 (0.89) | 3.55 (0.76) | 3.76 (0.92) | 4.00 (1.12) | 3.33 (1.12) | 3.24 (0.84) |
| Disability (WHODAS) | |||||||||
| Mean (SD) | 10.88 (10.45) | 21.56 (13.13) | 15.75 (15.06) | 18.65 (15.85) | 19.17 (15.43) | 30.93 (18.13) | 42.40 (18.05) | 35.05 (22.06) | 39.62 (20.25) |
Factors, associated with social support
The models of regression conducted are shown in Table 2. In the first model disability, extraversion, agreeableness, gender, age and comorbidity were significantly related with social support. In the second model the type of health condition was added, but the increase in the variance explained was not significant (ΔR2 = 0.016, p = .21). The results revealed that disability (ß = .19, = .002), agreeableness (ß = .17, p < .001) and extraversion (ß = .15, p = .001) were the strongest factors for social support. Gender, age and comorbidity were significant in Model 1, but when the health conditions were introduced to the model, only gender remained significant (ß = .10, p = .027), meaning that men experienced higher social support than women. Quality of life, marital status, level of education and type of health condition were not significant factors. All the variables considered in the models had an associated VIF value lower than 5 (mean VIF of 2.20), indicating that the assumption of no perfect multicollinearity can be assumed to conduct the regression model. A post hoc power analysis was performed for the total sample of 722 individuals, considering a significance level of .05, and obtaining a statistical power higher than .90.
Table 2. Multiple linear regression analysis assessing the relationships between the independent variables considered and social support.
| Variables | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B (95% CI) | p | |ß| | B (95% CI) | p | |ß| | B (95% CI) | p | |ß| | |
| Severity of symptoms (Ref. = Mild) | |||||||||
| Moderate | 0.22 (-0.21, 0.66) | .31 | 0.05 | 0.19 (-0.28, 0.66) | .42 | 0.04 | 0.21 (-0.26, 0.68) | .38 | 0.05 |
| Severe | 0.55 (0.05, 1.04) | .029 | 0.11 | 0.42 (0.16, 1.01) | .15 | 0.09 | 0.42 (0.16, 0.99) | .15 | 0.09 |
| Disability | -0.03 (-0.04, -0.01) | <.001 | 0.24 | -0.02 (-0.03, -0.01) | .002 | 0.19 | -0.07 (-0.11, -0.03) | .001 | 0.66 |
| Resilience | 0.01 (-0.07, 0.06) | .90 | 0.01 | 0.02 (-0.04, 0.09) | .49 | 0.03 | 0.02 (-0.05, 0.08) | .60 | 0.03 |
| Quality of Life | -0.07 (-0.14, 0.01) | .08 | 0.08 | 0.06 (-0.13, 0.02) | .13 | 0.07 | -0.06 (-0.14, 0.01) | .11 | 0.07 |
| Extraversion | 0.34 (0.16, 0.52) | <.001 | 0.16 | 0.32 (0.13, 0.49) | .001 | 0.15 | 0.01 (-0.30, 0.27) | .92 | 0.01 |
| Openness | -0.01 (-0.19, 0.17) | .91 | 0.01 | 0.01 (-0.18, 0.19) | .95 | 0.01 | -0.02 (-0.20, 0.16) | .86 | 0.01 |
| Neuroticism | -0.11 (-0.29, 0.08) | .26 | 0.05 | -0.10 (-0.29, 0.09) | .29 | 0.05 | -0.08 (-0.27, 0.10) | .37 | 0.04 |
| Conscientiousness | 0.19 (-0.01, 0.39) | .07 | 0.08 | 0.20 (-0.02, 0.41) | .07 | 0.08 | 0.21 (-0.01, 0.42) | .05 | 0.09 |
| Agreeableness | 0.36 (0.16, 0.55) | <.001 | 0.16 | 0.38 (0.18, 0.59) | <.001 | 0.17 | 0.26 (-0.06, 0.59) | .11 | 0.11 |
| Disability*Agreeableness | 0.004 (-0.005, 0.01) | .35 | 0.16 | ||||||
| Disability*Extraversion | 0.01 (0.004, 0.02) | .004 | 0.37 | ||||||
| Controlling variables | |||||||||
| Marital status | -0.21 (-0.57, 0.15) | .25 | 0.05 | -0.17 (-0.56, 0.21) | .37 | 0.04 | -0.14 (-0.53, 0.24) | .47 | 0.03 |
| Education | -0.01 (-0.18, 0.17) | .96 | 0.01 | 0.01 (-0.17, 0.19) | .92 | 0.01 | 0.003 (-0.18, 0.18) | .99 | 0.01 |
| Gender | 0.50 (0.13, 0.86) | .008 | 0.11 | 0.44 (-0.05, 0.83) | .027 | 0.10 | 0.45 (0.06, 0.84) | .024 | 0.10 |
| Age | -0.01 (-0.02, -0.001) | .031 | 0.10 | -0.01 (-0.03, 0.01) | .07 | 0.12 | -0.01 (-0.03, 0.001) | .05 | 0.13 |
| Comorbidity | 0.05 (-0.01, 0.09) | .031 | 0.11 | 0.02 (-0.03, 0.07) | .43 | 0.05 | 0.02 (-0.03, 0.07) | .51 | 0.04 |
| Health Condition (Ref. Depression) | |||||||||
| Epilepsy | 0.12 (-0.80, 1.04) | .79 | 0.02 | 0.20 (-0.72, 1.12) | .67 | 0.03 | |||
| Migraine | 0.46 (-1.35, 0.43) | .31 | 0.08 | -0.41 (-1.29, 0.47) | .36 | 0.07 | |||
| Multiple Sclerosis | -0.45 (-1.53, 0.62) | .41 | 0.06 | -0.31 (-1.39, 0.77) | .57 | 0.04 | |||
| Parkinson Disease | 0.46 (-1.39, 0.46) | .33 | 0.07 | -0.35 (-1.27, 0.58) | .46 | 0.06 | |||
| Stroke | 0.23 (-0.70, 1.16) | .63 | 0.03 | 0.32 (-0.61, 1.25) | .50 | 0.05 | |||
| Schizophrenia | 1.05 (-2.01, -0.01) | .05 | 0.12 | -0.90 (-1.95, 0.15) | .09 | 0.11 | |||
| Dementia | -0.08 (-1.05, 0.89) | .87 | 0.13 | -0.10 (-1.05, 0.86) | .84 | 0.01 | |||
| Substance Use | -0.04 (-1.99, 0.92) | .94 | 0.01 | 0.06 (-0.89, 1.01) | .90 | 0.01 |
Note: Model 2 was controlled for health conditions as dummy variables (depression, dementia, epilepsy, migraine, multiple sclerosis, Parkinson’s disease, schizophrenia, stroke and substance use disorders).
*The significant associations are in bold
Interaction between personality and disability
We additionally assessed in model 3 whether there was a specific interaction between the most important personality and health related factors for social support. The results revealed that the interaction between disability and extraversion was significant (ß = .37, p = .004) as opposed to the interaction between disability and agreeableness (p = .35). However, disability alone remained the most important factor for social support (ß = .66, p = .001) in the model.
Mediation and Moderation
Two mediation analyses were conducted including the significant personality traits found in the main multiple regression analysis as independent variables and disability as a mediator. In the first case, presented in Fig 1, disability significantly mediated the relationship between agreeableness and social support (Sobel’s z = 3.18, p = .001). The standardized indirect to total ratio was .154, demonstrating that about 15% of the basic relationship between agreeableness and social support was explained partially by the involvement of disability. In the second analysis, shown in Fig 2, a mediation model was tested to determine whether disability significantly mediated the relation between extraversion and social support. The results indicated that disability was a significant mediator (Sobel’s z = 2.77, p = .006). The standardized indirect to total ratio was .130, suggesting that about 13% of the link between extraversion and social support can be partially explained by the level of disability of individuals.
Fig 1. Mediation between agreeableness (IV), disability (MedV) and social support (DV).
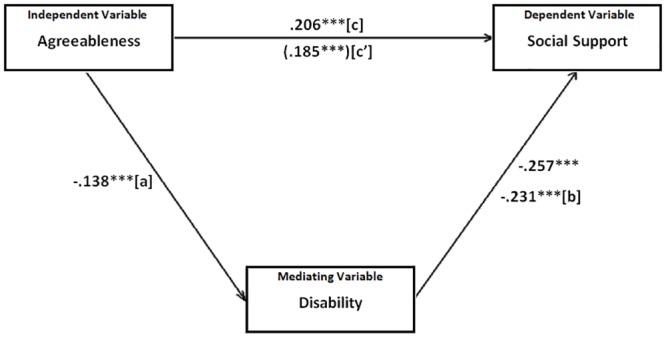
Note: ***p < .001 The numerical values are zero order correlations. Path c' represents the beta weight for the independent-to-dependent variable relationship adjusted for the inclusion of the mediating variable.
Fig 2. Mediation between extraversion (IV), disability (MedV) and social support (DV).
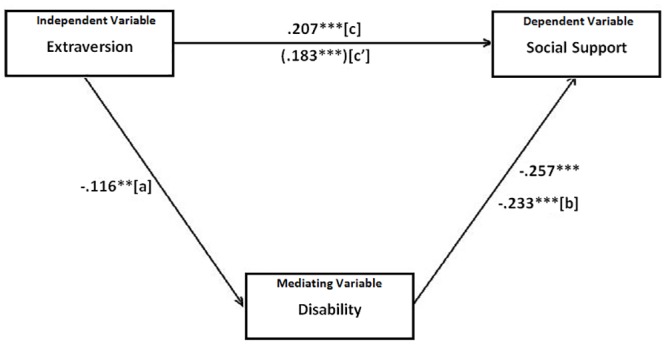
Note: ***p < .001 The numerical values are zero order correlations. Path c' represents the beta weight for the independent-to-dependent relationship adjusted for the inclusion of the mediating variable
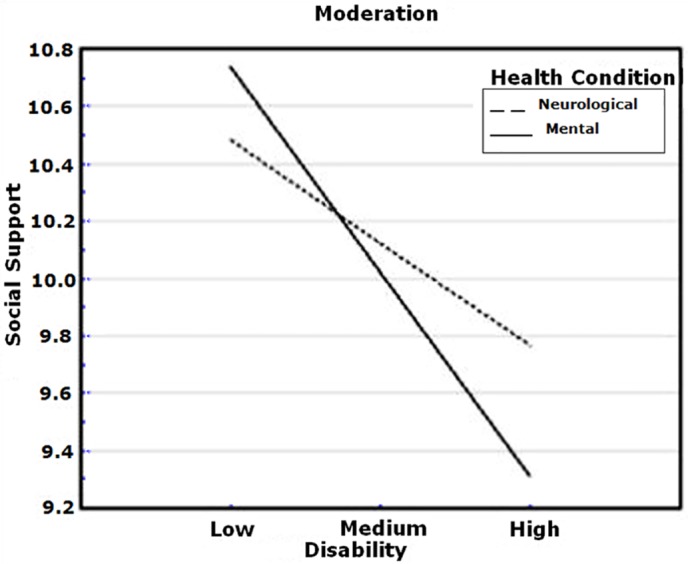
Health condition (mental and neurological) was examined as a moderator in the relation between disability and social support. The analysis revealed that it was a significant determinant (interaction effect: ß = .13, p = .05). Thus, although higher disability levels were related to lower social support in both groups of health condition, higher levels of disability still decreased the social support in people with mental problems more than in individuals suffering from neurological diseases. Fig 3 shows the simple slopes of the mental and neurological conditions. Both were significantly different from zero (simple slope associated to mental health condition = -0.03, t = -5.30, p < .001; simple slope associated to neurological health condition = -0.02, t = -2.91, p = .004).
Fig 3. Simple slopes of disability predicting social support for people with mental and neurological health conditions.
Discussion
This study was set to analyze the strongest factors for social support in neuropsychiatric disorders. Disability was the strongest factor associated with social support. As hypothesized, lower levels of disability were strongly associated with higher level of social support. The general direction in previous literature has been towards social support as a predictor or mediator of disability. Yet, the few studies exploring the opposite relationship confirm our finding. Baseman, Fisher [53] found that functional status is a significant predictor of social integration in survivors of stroke. High functional disability has been found to be associated with low social support in depression [16]. Consequently, our results show that the level of social support depends primarily on day-to-day problems that the individuals experience. However, longitudinal research should explore whether the disability leads people to feel they are not supported enough or they feel more disabled because they are not supported.
Disability remained the most significant factor for social support even when the interaction effects with extraversion and agreeableness were added to the model. Extraversion and agreeableness were found to be highly associated with social support and this outcome was consistent with preceding literature [13]. However both variables were no longer significant when the interaction terms were introduced, whilst the interaction term between disability and extraversion was significant.
These results suggest that the interaction between disability and certain personality traits is an important correlate of social support. The cross-sectional design of the study does not allow us to draw causality or explore further the direction of association, but our findings suggest that improving day-to-day functioning and certain maladaptive personality styles may improve individual’s perception of social support and not only vice versa [54]. Literature has already demonstrated that psychological treatment is efficacious in improving functional domains such as interpersonal relationships, social participation, etc.[55, 56], which, in turn, we found to have a strong relationship with social support. On the other hand, modifying certain maladaptive personality styles, reducing Interpersonal Sensitivity or Interpersonal Aggression is possible with long-term therapy (e.g. dialectical behavioral therapy) [57]. Extraversion, for example, which we found to interact with disability, significantly influences character adaptations associated with interpersonal relationships [13]. Thus, clinicians should be aware that modifying certain features of this personality trait might also change the perception of social support by others. Future longitudinal research, however, is warranted to explore in depth this finding.
The present study aimed to investigate the interrelations between personality traits and disability further. The two strongest factors—personality and disability were examined in mediation analyses. The two analyses indicated that disability partially explained the relationship between agreeableness, extraversion, and social support. Extraversion and agreeableness were negatively related to disability, showing that the more agreeable/extraverted a person is the less disability he/she experiences. On other hand, disability negatively predicted social support, indicating that the lower the level of disability is, the higher the social support is. Although the mediations were only partial and other indirect effects could have an empirical importance in the relationship between personality and social support, this outcome implies the importance of disability as a factor that has to be taken into account in future longitudinal analyses.
Finally, the moderation analysis revealed that both sufferers from mental and neurological disorders experienced lower social support when their level of disability was high. In the lower range of disability both mental and neurological disorders experienced similar levels of social support. However, people with mental disorders had lower levels of support compared to neurological disorders in case of high disability. First, this might be because both neurological and mental disorders differ substantially in certain aspects—duration, persistence, recurrence, number of episodes, chronicity. Another possibility may be that mental health problems are socially stigmatized to some extent and severe disability in these health conditions is still not highly recognized as opposed to neurological diseases [19]. The relevance of the finding, although considerable, should be seen cautiously, because of the cross-sectional design of the study.
Limitations
The study has three main limitations. First, the design is cross-sectional, thus not allowing firm conclusions on causality. The overall sample size, wide scope and innovativeness, yet, do make the findings of the current study relevant. The second limitation is that the data for each disorder was collected in one single country, hence not allowing for more generalizability of the results. This was driven by the fact that the data collection was done according to the expertise of the research centers. Another possible limitation is the use of proxies to obtain data for some of the individuals with dementia. Reports from proxies may have biased the results to some extent in this group. However, 64 individuals were capable of giving their consent and we used proxies for only 16 persons.
Conclusion
The current paper shed light on an under-researched niche, namely factors for social support in people with neuropsychiatric disorders. Our findings showed that disability was the strongest factor for social support. Extraversion and agreeableness were significant personality variables, but the analyses revealed that they were dependent on the level of disability. Furthermore, findings revealed that the health conditions were not related factors to social support. The study is beneficial for clinicians to tailor support interventions in primary or secondary health care and implement programs encouraging social support in the community. Unlike the previous line of mental health actions, focused on increasing social support as the origin of bettering disability, this study suggests that future interventions should focus effectively on improving disability and maladaptive personality styles as a source of enhancing social support.
Data Availability
Due to ethical restrictions imposed by Järvenpää Addiction Hospital, one of the partner institutions of the PARADISE consortium of which the authors are a part, data are available upon request to Dr. Alarcos Cieza at a.cieza@soton.ac.uk.
Funding Statement
This study used data for secondary analysis from the international project Psychosocial fActors Relevant to brAin DISorders in Europe (PARADISE). The project was supported by a grant of the European Commission under the Seventh Framework Programme, Grant Agreement no. HEALTH-F2-2009-241572.
References
- 1.Kruithof WJ, van Mierlo ML, Visser-Meily JM, van Heugten CM, Post MW. Associations between social support and stroke survivors' health-related quality of life—a systematic review. Patient Educ Couns. 2013;93(2):169–76. Epub 2013/07/23. 10.1016/j.pec.2013.06.003 . [DOI] [PubMed] [Google Scholar]
- 2.Taylor SE. Social support: A Review In Friedman M.S.. The Handbook of Health Psychology. NY: Oxford UniversityPress; pp 189–214. 2011. [Google Scholar]
- 3.Uchino B. Social Support and Physical Health: Understanding the Health Consequences of Relationships. New Haven, CT: Yale University Press; 2004. [Google Scholar]
- 4.Lakey B, Cronin A. Low social support and major depression: Research, theory, and methodological issues" In Dobson K.S., & Dozois D.. Risk factors for depression. Academic Press; pp 385–408. 2008. [Google Scholar]
- 5.Stronks DL, Tulen JH, Pepplinkhuizen L, Verheij R, Mantel GW, Spinhoven P, et al. Personality traits and psychological reactions to mental stress of female migraine patients. Cephalalgia: an international journal of headache. 1999;19(6):566–74. Epub 1999/08/17. . [DOI] [PubMed] [Google Scholar]
- 6.Lindfors O, Ojanen S, Jaaskelainen T, Knekt P. Social support as a predictor of the outcome of depressive and anxiety disorder in short-term and long-term psychotherapy. Psychiatry research. 2014;216(1):44–51. Epub 2014/02/11. 10.1016/j.psychres.2013.12.050 . [DOI] [PubMed] [Google Scholar]
- 7.ten HM, Vollebergh W, Bijl R, Ormel J. Combined effect of mental disorder and low social support on care service use for mental health problems in the Dutch general population. Psychological medicine. 2002;32(2):311–23. Epub 2002/02/28. . [DOI] [PubMed] [Google Scholar]
- 8.World Health Organization. mhGAP intervention guide for mental, neurological and substance use disorders in non-specialized health settings: mental health Gap Action Programme (mhGAP). Geneva: World Health Organization; 2010. [PubMed] [Google Scholar]
- 9.Santini ZI, Koyanagi A, Tyrovolas S, Mason C, Haro JM. The association between social relationships and depression: a systematic review. Journal of affective disorders. 2015;175:53–65. Epub 2015/01/17. 10.1016/j.jad.2014.12.049 . [DOI] [PubMed] [Google Scholar]
- 10.Souza JD, Villar Luis MA, Ventura CA, Barbosa SP, Santos CBD. Perception of social support: a comparative study between men with and without substance-related disorders. Journal of Substance Use, (0), 1–6. 2014. [Google Scholar]
- 11.Cresswell CM, Kuipers L, Power MJ. Social networks and support in long-term psychiatric patients. Psychological medicine. 1992;22(4):1019–26. Epub 1992/11/01. . [DOI] [PubMed] [Google Scholar]
- 12.Kitamura T, Watanabe K, Takara N, Hiyama K, Yasumiya R, Fujihara S. Precedents of perceived social support: personality, early life experiences and gender. Psychiatry Clin Neurosci. 2002;56(2):169–76. Epub 2002/04/16. 10.1046/j.1440-1819.2002.00951.x . [DOI] [PubMed] [Google Scholar]
- 13.Cukrowicz KC, Franzese AT, Thorp SR, Cheavens JS, Lynch TR. Personality traits and perceived social support among depressed older adults. Aging Ment Health. 2008;12(5):662–9. Epub 2008/10/16. 10.1080/13607860802343258 . [DOI] [PubMed] [Google Scholar]
- 14.Burkert S, Kendel F, Kiep H, Holtkamp M, Gaus V. Gender differences in social support in persons with epilepsy. Epilepsy & behavior: E&B. 2015. Epub 2015/04/08. . [DOI] [PubMed] [Google Scholar]
- 15.Hamaideh S, Al-Magaireh D, Abu-Farsakh B, Al-Omari H. Quality of life, social support, and severity of psychiatric symptoms in Jordanian patients with schizophrenia. Journal of psychiatric and mental health nursing. 2014;21(5):455–65. Epub 2013/10/15. 10.1111/jpm.12112 . [DOI] [PubMed] [Google Scholar]
- 16.Chao SF. Functional disability and depressive symptoms: longitudinal effects of activity restriction, perceived stress, and social support. Aging Ment Health. 2014;18(6):767–76. Epub 2014/02/01. 10.1080/13607863.2013.878308 . [DOI] [PubMed] [Google Scholar]
- 17.D'Amico D, Grazzi L, Bussone G, Curone M, Di Fiore P, Usai S, et al. Are Depressive Symptomatology, Self-Efficacy, and Perceived Social Support Related to Disability and Quality of Life in Patients With Chronic Migraine Associated to Medication Overuse? Data From a Cross-Sectional Study. Headache, Vol 55, 5, 636–645. 2015. [DOI] [PubMed] [Google Scholar]
- 18.Travis LA, Lyness JM, Shields CG, King DA, Cox C. Social support, depression, and functional disability in older adult primary-care patients. Am J Geriatr Psychiatry. 2004;12(3):265–71. Epub 2004/05/06. . [PubMed] [Google Scholar]
- 19.Van Orden KA, Li Y, Podgorski CA, Conwell Y. The association between higher social support and lower depressive symptoms among aging services clients is attenuated at higher levels of functional impairment. International journal of geriatric psychiatry. 2015. Epub 2015/02/11. 10.1002/gps.4266 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hartley S, McArthur M, Coenen M, Cabello M, Covelli V, Roszczynska-Michta J, et al. Narratives reflecting the lived experiences of people with brain disorders: common psychosocial difficulties and determinants. PloS one. 2014;9(5):e96890 Epub 2014/05/09. 10.1371/journal.pone.0096890 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.World Health Organization. International Classification of Diseases and Related Health Problems. 10th edition Geneva, Switzerland: World Health Organization; 1992. [Google Scholar]
- 22.Hu L, Bentler P. Cutoff criteria for fit indices in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model, 6:1–55. 1999. [Google Scholar]
- 23.Reise SP, Widaman KF, Pugh RH. Confirmatory factor analysis and item response theory: two approaches for exploring measurement invariance. Psychological bulletin. 1993;114(3):552–66. Epub 1993/11/01. . [DOI] [PubMed] [Google Scholar]
- 24.Steiger J. Understanding the limitations of global fit assessment in structural equation modelling. Personal Individ Differ, 42:893–898 2007. [Google Scholar]
- 25.Dalgard OS. Community health profile as tool for psychiatric prevention In: Trent D.R. & Reed C., ed. Promotion of mental health, Vol. 5. Aldershot, Avebury: 1996. [Google Scholar]
- 26.Dalgard OS, Dowrick C, Lehtinen V, Vazquez-Barquero JL, Casey P, Wilkinson G, et al. Negative life events, social support and gender difference in depression: a multinational community survey with data from the ODIN study. Soc Psychiatry Psychiatr Epidemiol. 2006;41(6):444–51. Epub 2006/03/31. 10.1007/s00127-006-0051-5 . [DOI] [PubMed] [Google Scholar]
- 27.World Health Organization. WHODAS II Disability Assessment Schedule http://who.int/icidh/whodas/index.html accessed 7 July 2008. 2001.
- 28.Luciano JV, Ayuso-Mateos JL, Fernandez A, Serrano-Blanco A, Roca M, Haro JM. Psychometric properties of the twelve item World Health Organization Disability Assessment Schedule II (WHO-DAS II) in Spanish primary care patients with a first major depressive episode. Journal of affective disorders. 2010;121(1–2):52–8. Epub 2009/05/26. 10.1016/j.jad.2009.05.008 . [DOI] [PubMed] [Google Scholar]
- 29.Andrews G, Kemp A, Sunderland M, Von Korff M, Ustun TB. Normative data for the 12 item WHO Disability Assessment Schedule 2.0. PloS one. 2009;4(12):e8343 Epub 2009/12/19. 10.1371/journal.pone.0008343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schmidt S, Muhlan H, Power M. The EUROHIS-QOL 8-item index: psychometric results of a cross-cultural field study. Eur J Public Health. 2006;16(4):420–8. Epub 2005/09/06. 10.1093/eurpub/cki155 . [DOI] [PubMed] [Google Scholar]
- 31.da Rocha NS, Power MJ, Bushnell DM, Fleck MP. The EUROHIS-QOL 8-item index: comparative psychometric properties to its parent WHOQOL-BREF. Value Health. 2012;15(3):449–57. Epub 2012/05/16. 10.1016/j.jval.2011.11.035 . [DOI] [PubMed] [Google Scholar]
- 32.Sinclair VG, Wallston KA. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assessment. 2004;11(1):94–101. Epub 2004/03/05. . [DOI] [PubMed] [Google Scholar]
- 33.John OP, Donahue EM, Kentle RL. The ‘‘Big Five”inventory: Versions 4a and 5. Berkeley, CA: Institute for Personality and Social Research; 1991. [Google Scholar]
- 34.John OP, Srivastava S. The Big-Five trait taxonomy: History, measurement, and theoretical perspectives In Pervin L. A. & John O. P. (Eds.), Handbook of personality: Theory and research (Vol. 2, pp. 102–138). New York: Guilford Press; 1999. [Google Scholar]
- 35.Rammstedt B, John O. Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. Journal of research in Personality, 41(1), 203–212. 2007. [Google Scholar]
- 36.Hamilton M. A rating scale for depression. Journal of Neurology, Neurosurgery, and Psychiatry 23:56–62. 1960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Mungas D. In-office mental status testing: a practical guide. Geriatrics. 1991;46(7):54–8, 63,, 6 Epub 1991/07/01. . [PubMed] [Google Scholar]
- 38.Stewart WF, Lipton RB, Simon D, Von Korff M, Liberman J. Reliability of an illness severity measure for headache in a population sample of migraine sufferers. Cephalalgia: an international journal of headache. 1998;18(1):44–51. Epub 1998/05/28. . [DOI] [PubMed] [Google Scholar]
- 39.Kurtzke JF. Rating neurological impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33:1444–1452. 1983. [DOI] [PubMed] [Google Scholar]
- 40.Hobart J, Freeman J, Lamping D, Fitzpatrick R, Thompson A. The SF-36 in multiple sclerosis: why basic assumptions must be tested. J Neurol Neurosurg Psychiatry. 2001;71(3):363–70. Epub 2001/08/21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Goetz CG, Poewe W, Rascol O, Sampaio C, Stebbins GT, Counsell C, et al. Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: status and recommendations. Mov Disord. 2004;19(9):1020–8. Epub 2004/09/17. 10.1002/mds.20213 . [DOI] [PubMed] [Google Scholar]
- 42.Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. Clinical implications of Brief Psychiatric Rating Scale scores. The British journal of psychiatry: the journal of mental science. 2005;187:366–71. Epub 2005/10/04. 10.1192/bjp.187.4.366 . [DOI] [PubMed] [Google Scholar]
- 43.Goldstein LB, Bertels C, Davis JN. Interrater reliability of the NIH stroke scale. Arch Neurol. 1989;46(6):660–2. Epub 1989/06/01. . [DOI] [PubMed] [Google Scholar]
- 44.Skinner HA, Allen BA. Alcohol dependence syndrome: measurement and validation. J Abnorm Psychol. 1982;91(3):199–209. Epub 1982/06/01. . [DOI] [PubMed] [Google Scholar]
- 45.Sangha O, Stucki G, Liang MH, Fossel AH, Katz JN. The Self-Administered Comorbidity Questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Rheum. 2003;49(2):156–63. Epub 2003/04/11. 10.1002/art.10993 . [DOI] [PubMed] [Google Scholar]
- 46.Buntin MB, Zaslavsky AM. Too much ado about two-part models and transformation? Comparing methods of modeling Medicare expenditures. J Health Econ. 2004;23(3):525–42. Epub 2004/05/04. . [DOI] [PubMed] [Google Scholar]
- 47.Alonso J, Petukhova M, Vilagut G, Chatterji S, Heeringa S, Ustun TB, et al. Days out of role due to common physical and mental conditions: results from the WHO World Mental Health surveys. Mol Psychiatry. 2011;16(12):1234–46. Epub 2010/10/13. 10.1038/mp.2010.101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Rogerson PA. Statistical methods for geography. London: Sage; 2001. [Google Scholar]
- 49.IBM. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp; 2012. [Google Scholar]
- 50.Jose PE. MedGraph-I: A programme to graphically depict mediation among three variables: The internet version, version 3.0. Victoria University of Wellington, Wellington, New Zealand. Retrieved [date] from http://pavlovpsycvuwacnz/paul-jose/medgraph/. 2013.
- 51.Jose PE. Doing statistical mediation and moderation. Guilford Press; 2012. [Google Scholar]
- 52.Jose PE. ModGraph-I: A programme to compute cell means for the graphical display of moderational analyses: The internet version, Version 3.0. Victoria University of Wellington, Wellington, New Zealand Retrieved [date] from http://pavlovpsycvuwacnz/paul-jose/modgraph/. 2013.
- 53.Baseman S, Fisher K, Ward L, Bhattacharya A. The relationship of physical function to social integration after stroke. J Neurosci Nurs. 2010;42(5):237–44. Epub 2010/10/26. . [DOI] [PubMed] [Google Scholar]
- 54.McCorkle BH, Rogers ES, Dunn EC, Lyass A, Wan YM. Increasing social support for individuals with serious mental illness: evaluating the compeer model of intentional friendship. Community mental health journal. 2008;44(5):359–66. Epub 2008/05/16. 10.1007/s10597-008-9137-8 . [DOI] [PubMed] [Google Scholar]
- 55.De Silva MJ, Cooper S, Li HL, Lund C, Patel V. Effect of psychosocial interventions on social functioning in depression and schizophrenia: meta-analysis. The British journal of psychiatry: the journal of mental science. 2013;202(4):253–60. Epub 2013/04/04. 10.1192/bjp.bp.112.118018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Renner F, Cuijpers P, Huibers MJ. The effect of psychotherapy for depression on improvements in social functioning: a meta-analysis. Psychological medicine. 2014;44(14):2913–26. Epub 2014/01/30. 10.1017/S0033291713003152 . [DOI] [PubMed] [Google Scholar]
- 57.Lynch TR, Cheavens JS, Cukrowicz KC, Thorp SR, Bronner L, Beyer J. Treatment of older adults with co-morbid personality disorder and depression: a dialectical behavior therapy approach. International journal of geriatric psychiatry. 2007;22(2):131–43. Epub 2006/11/11. 10.1002/gps.1703 . [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Due to ethical restrictions imposed by Järvenpää Addiction Hospital, one of the partner institutions of the PARADISE consortium of which the authors are a part, data are available upon request to Dr. Alarcos Cieza at a.cieza@soton.ac.uk.