

Abstract
Introduction
Although limited in empirical support, Alcohol Expectancy (AE) theory posits that AEs may overestimate subjective response (SR) to the positive effects of alcohol, which, in turn, confers alcohol-related risk (e.g., Darkes & Goldman, 1993). The recent development of the Anticipated Effects of Alcohol Scale (AEAS; Morean, Corbin, & Treat, 2012) and the Subjective Effects of Alcohol Scale (SEAS; Morean, Corbin, & Treat, 2013) now permits direct AE-SR comparisons using psychometrically sound assessments designed for this purpose.
Methods
We ran secondary data analyses (Morean et al., 2012; 2013) evaluating measurement invariance of AEs and SR; AE-SR relationships; the accuracy of AEs; and relations between AE-SR discrepancies and binge drinking, driving after drinking, and alcohol-related problems in a sample of 102 young adults (mean age 22.81 [2.25]; 74.5% male; 76.5% Caucasian) who consumed alcohol in a simulated bar setting (target blood alcohol level = .08g/dL).
Results
The AEAS and SEAS were scalar measurement invariant and that AEs generally overestimated SR (mean Cohen's d = .48). Relative to SR, inflated high arousal negative AEs (e.g., aggressive) were associated with frequent binge drinking and alcohol-related problems, whereas exaggerated low arousal negative AEs (e.g., woozy) served protective functions. As blood alcohol levels rose, inflated low arousal positive AEs (e.g., relaxed) and low arousal negative AEs (e.g., wobbly) were associated with less frequent driving after drinking.
Conclusions
Challenging AE-SR discrepancies for high arousal effects may have utility in treatment and prevention efforts, whereas maintaining overestimates of low arousal effects may serve protective functions.
Keywords: alcohol expectancies, subjective response to alcohol, binge drinking, alcohol-related problems, drunk driving, drink driving
Introduction
Reciprocal determinism (Bandura, 2004, 2012), a critical tenet of social learning models of alcohol use, posits that drinkers' expectations about the probable outcomes of drinking (alcohol expectancies; AE) and their subjective experience of acute alcohol effects during a drinking episode (subjective response; SR) are bidirectionally related determinants of drinking behavior. Specifically, drinking is thought to be motivated, in part, by the expectation that it will result in a positive experience via increasing positive affect or reducing negative affect. If pleasant effects are experienced, positive AEs are reinforced and poised to motivate further drinking. If negative alcohol effects are experienced, AEs should adjust accordingly, deterring future use. If this cycle is reliable, AEs and SR should accurately predict one another, especially with mounting drinking experience. However, relations among AEs, SR, and drinking are likely more complex.
Social Cognitive Theory (Bandura, 2012) suggests that cognitions (in this case AEs) can distort reality, and there is extensive evidence linking erroneous beliefs to poor outcomes (e.g., depression [Beck, 2008)], pathological gambling [Michalczuk, Bowden-Jones, Verdejo-Garcia, & Clark, 2011], and substance use [Shoal & Giancola, 2005]). Of central import, Expectancy Theory posits that AEs likely overestimate the positive effects of alcohol (e.g., Darkes & Goldman, 1993), a claim supported by several expectancy challenge studies in which reductions in drinking accompanied reductions in (presumably) inflated positive AEs (Darkes & Goldman, 1993, 1998; Wiers, van de Luitgaarden, van den Wildenberg, & Smulders, 2005). Drawing upon the tenets of Social Cognitive and Expectancy Theories, it seems plausible that AEs can inaccurately reflect SR, and that discrepant beliefs may confer risk for negative alcohol-related outcomes. However, very few published studies explicitly have evaluated the accuracy of AEs relative to SR. We review the two studies of which we are aware below.
Fromme and Dunn (1992) conducted a placebo-controlled laboratory study examining the influence of beverage condition, social context, drinking environment, and AEs on ad-libitum drinking and SR. AEs and SR were assessed via the Alcohol Effects Scale (Southwick et al., 1981), although it had not undergone psychometric evaluation for use as a SR measure. Participants reported their AEs one month prior to the lab session and were randomly assigned into the following conditions: Beverage condition (alcohol vs. placebo), social context (drinking with friendly vs. unfriendly confederates), and environmental setting (simulated bar vs. living room). Participants reported SR at the end of a 33-minute ad-lib consumption period. Only the findings of greatest relevance to the current study are reviewed here.
Participants generally expected more positive and negative alcohol effects than they experienced, leading the authors to conclude that AEs reflect exaggerations of SR. However, this conclusion must be considered cautiously for several reasons. First, the analyses examining AEs as predictors of SR were collapsed across all experimentally manipulated conditions, including beverage condition. Although mean SR levels did not differ by beverage condition, the magnitude of AE-SR discrepancies may have differed. Thus, the authors' approach may have led to underestimates or overestimates of discrepancies between AEs and SR to alcohol. Second, the average blood alcohol level (BAL) in the alcohol condition was .04 g%, approximating 2 drinks. When participants reported their AEs, the experimenters had not specified the number of drinks they should imagine consuming. Given their moderate to heavy drinking status (mean weekly drinks = 18 [range 11-45]), it seems likely that many participants' AEs corresponded to effects associated with consuming more than two drinks. If this were true, we would expect anticipated stimulant and impairing effects, which increase with BAL, to be stronger than the effects experienced.
In a more recent study, Wall and colleagues (2003) assessed AEs and SR in a licensed bar. Participants verbally confirmed that they had not consumed alcohol prior to their arrival. Participants stated how many drinks they intended to consume for the evening, reported their corresponding AEs using the Comprehensive Effects of Alcohol questionnaire (CEOA; Fromme et al., 1993), and proceeded with their nights as planned. As each participant finished drinking for the night, they reported their SR based on the number of drinks they had indicated at the onset of the study using a modified version of CEOA (note: there was a significant difference between the number of drinks participants intended to drink [3.82] and the number they consumed as verified by their bar tabs [4.22], and this effect was magnified for men). On average, participants' AEs and SRs correlated at .76. AE-SR discrepancies were observed on only one subscale; participants expected more risk and aggression than they experienced.
The study by Wall and colleagues (2003) provided important preliminary information about AE-SR relations in a naturalistic drinking setting, but it relied on a modified AE measure to assess SR that had not undergone appropriate psychometric evaluation. Further, many participants drank more than they had intended and differed with respect to the duration of their drinking episode, the peak BAL achieved, and their location on the BAC when they left the bar, which may have impacted the study results. Given that participants reported their SR immediately before leaving the bar, many reports of SR likely occurred as BALs were descending. In this case, the fact that participants overestimated risk and aggression may be expected given that these types of high arousal effects are less likely to occur as BALs fall.
In sum, although prior research provides preliminary evidence that AEs may exaggerate SR, the studies had a number of limitations including their reliance on assessment tools that had not been validated to assess both AEs and SR. To address this issue, we conducted a series of secondary data analyses (Morean et al., 2012; 2013) evaluating the relationships between AEs and SR across the ascending and descending limbs of the BAC using psychometrically sound, parallel measures of AEs (the Anticipated Effects and Alcohol Scale [AEAS]; Morean et al., 2012) and SR (the Subjective Effects of Alcohol Scale [SEAS]; Morean et al., 2013). Of note, these measures share a response format and assess 13 overlapping effects that vary with respect to valence (positive, negative) and arousal (stimulant, sedative). Among other strengths, assessing AEs and SRs that sample the full range of affective space affords a level of theoretical and methodological precision with respect to examining relationships between AEs and SR that prior assessment tools have not provided. Within the current study, we made the following hypotheses: 1) the AEAS and SEAS would evidence scalar measurement invariance, given their similarities, thereby ensuring our ability to make statistically meaningful AE-SR comparisons and to evaluate AE-SR discrepancies; 2) AEs and SR would be related yet distinct constructs, consistent with social learning theory; 3) AEs generally would represent nomothetic exaggerations of SR, consistent with Expectancy Theory; and 4) overestimating positive, stimulant alcohol effects would be associated ideographically with heavy drinking, driving after drinking, and the experience of alcohol-related problems, whereas overestimating negative, sedative alcohol effects would protect against these negative drinking outcomes. We did not make predictions regarding AE-SR discrepancies for positive sedative alcohol effects (e.g., relaxation) or negative stimulant alcohol effects (e.g., aggression) given the lack of prior research examining these domains of SR (and consequently their association with AEs).
Materials and Methods
A detailed description of study participants and procedures can be found in previously published work (Morean et al., 2012; 2013). However, we briefly describe key aspects of the study design below as background for the current study.
2.1 Participants
We recruited 215 individuals from college campuses and the greater communities of New Haven, CT (N=112) and Tempe, AZ (N=103) to participate in a placebo-controlled alcohol administration study in a simulated bar setting. Exclusion criteria included drinking < 3 drinks/week, adverse reactions to alcohol, lifetime enrollment in abstinence-based alcohol or gambling treatment, and pregnancy. Given the current study's focus on potential discrepancies between AEs and SR to alcohol, analyses were conducted using data from participants in the alcohol condition only (n = 102, mean age 22.81 [2.25]; 74.5% male; 76.5% Caucasian). AE-SR discrepancies were not examined in the placebo condition for the following reasons: 1) examining AE-SR discrepancies in the placebo condition would lack meaning as this condition does not occur in naturalistic drinking settings (i.e., drinkers do not anticipate consuming alcohol and subsequently consume placebo in the real world), 2) individuals' AEs as reported on self-report measures are based on what they expect to experience when they actually consume alcohol, and 3) examining discrepancies within the alcohol and placebo conditions would address a separate research question about the relationship between implicit and explicit AEs, and a discussion of the background literature on this topic is beyond the scope of the current study.
2.2 Procedure
Prior to conducting the study, we received approval from the human subjects committees of both participating universities. Groups of 2-4 participants attended two lab sessions separated by 2 weeks. Prior to beginning the beverage administration session (session 1), participants gave proof of their age via a valid photo ID, reviewed all informed consent materials, and provided consent. Meanwhile, overhead lights in the bar lab were dimmed, neon beer signs were illuminated, and popular music was cued. Participants and research assistants were blind to beverage condition; a supervisor collected all breath alcohol samples. Research assistants acted as bartenders and served participants 3 vodka-based drinks over 30-minutes (10 minutes per drink). SR was assessed for the first time at the end of a 15-minute absorption period based on prior research suggesting that SR may peak up to 25 minutes before BrAC levels reach their peak (Radlow & Hurst, 1985). To capture SR across the full drinking episode, SR was assessed four additional times post-beverage administration, each separated by 20 minutes. At the end of session 1, participants were scheduled to return to the lab in two weeks to complete session 2. During session 2, participants were interviewed about their drinking behavior and completed a number of self-report measures including the measure of alcohol expectancies.
2.3 Measures
2.3.1 Subjective Response (SEAS; Morean, et al., 2013)
Using an 11-point rating scale ranging from “not at all” to “extremely,” participants reported their SR of 14 alcohol effects. The SEAS subscales correspond to affective quadrants: high arousal positive (HIGH+; e.g., funny), high arousal negative (HIGH-; e.g., aggressive), low arousal positive (LOW+; e.g., relaxed), and low arousal negative (LOW-; e.g., woozy). The SEAS is a reliable and valid SR measure and is scalar-invariant by beverage condition; limb of the BAC; gender; and family history of alcoholism, drinking, and smoking status (Morean et al., 2013). Ascending and descending limb SR scores were calculated for each participant as described in Morean et al. (2013).
2.3.2 Alcohol Expectancies (AEAS; Morean et al., 2012)
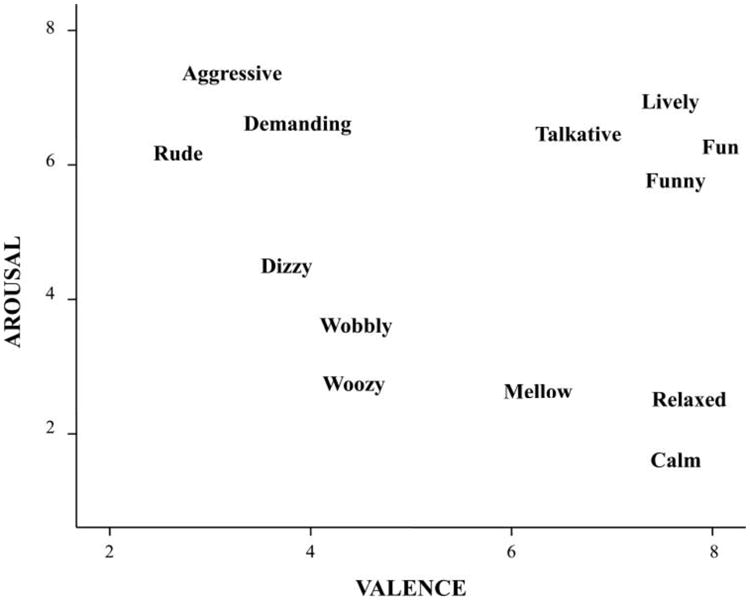
The AEAS is a 22-item self-report measure that was developed concurrently with the SEAS to facilitate AE-SR comparisons. The AEAS and SEAS employ the same 11-point response scale, share 13 overlapping items (see Figure 1), and assess AEs and SR corresponding to a blood alcohol level of .08%; prior to reporting their AEs, participants were asked to imagine consuming either 4 drinks (for women) or 5 drinks (for men) in a 2-hour period, an imagined dose that is comparable to the target peak BrAC in the alcohol administration study (.08g%). The AEAS and SEAS also assess the experience of alcohol effects corresponding to the ascending and descending limbs of the BAC; to capture AEs associated with the ascending limb, participants were asked to imagine and report how they would feel if they had just finished consuming either 4 or 5 drinks (i.e., immediately after the final hypothetical drink). To capture descending limb AEs, participants were prompted to report how they would feel 90 minutes after finishing their final drink. The AEAS comprises four subscales that mirror those of the SEAS and is a reliable and valid measure that is scalar invariant by limb of the BAC, gender, family history status, drinking status, and smoking status.
Figure 1. The 13 overlapping SEAS and AEAS items plotted in affective space.
2.3.3 Binge Drinking (Timeline Follow-Back [TLFB]; Sobell and Sobell, 2003)
Participants reported the number of drinks they consumed each day over the past month. The frequency of binge drinking was calculated based on the number of times participants reported drinking 4/5drinks in 2 hours or less for women/men. The TLFB is the gold standard for assessing drinking with well-established psychometrics (Fals-Stewart et al. 2000).
2.3.4 Driving after drinking
Participants reported how frequently in the past month they drove a motor vehicle after consuming 1) ≥ 2 drinks and 2) ≥ 4 drinks. Given relatively low endorsement rates, a composite variable reflecting the frequency of driving after any drinking was created.
2.3.5 Alcohol-Related Problems (The Rutgers Alcohol Problem Index [RAPI]; White & Labouvie, 1989; Neal, Corbin, & Fromme, 2006)
Participants reported how frequently over the past 3 months they experienced 23 alcohol-related problems using the following scale: never, 1–2 times, 3–5 times, 6–10 times, ≥ 10 times. Based on research by Neal and colleagues (2006) which indicated that an 18-item version of the RAPI was superior psychometrically to the original 23 item version, the 18 psychometrically sound items were recoded to 0 (did not experience consequence) or 1 (experienced the consequence at least once) and a summary score was created to reflect the total number of problems experienced.
Data Analytic Plan
3.1 Descriptive Statistics
Descriptive statistics were examined for the total number of drinks consumed in the past month, for the frequency of binge drinking in the past month, for the frequency of driving after drinking, and for the experience of alcohol related problems.
3.2 Manipulation Check
A simulated bar study is designed to approximate real-world drinking. Given that we aimed to create an enjoyable, social drinking experience, we anticipated that participants would report stronger positive than negative alcohol effects across the ascending and descending limbs of the BAC.
3.3 Measurement Invariance
To ensure that statistically meaningful AE-SR comparisons could be made, we employed a multiple-group confirmatory factor analytic approach (Vandenberg & Lance, 2000) to evaluate invariance of the latent factor structures (i.e., configural invariance), factor loadings (i.e., metric invariance), and intercepts (i.e., scalar invariance) across the SEAS and AEAS.
3.4 Internal Reliability of the AEAS and SEAS Subscales
Although the AEAS and SEAS are internally consistent measures (Morean et al., 2012; 2013), it was necessary to reevaluate internal consistency when only the 13 overlapping items were included.
3.5 Relations between AEs and SR
We used bivariate correlations to evaluate AE-SR relationships. Across the ascending and descending limbs, we expected: 1) moderate to large correlations between corresponding subscales (e.g., HIGH+ AEAS with HIGH+ SEAS), and 2) small to moderate correlations between subscales sharing valence (e.g., HIGH+ AEAS with LOW+ SEAS)
3.6 Accuracy of AEs
Using paired samples t-tests, we evaluated the extent to which the AEAS subscales accurately reflected their corresponding SEAS subscales.
3.7 Discrepancies between AEs and SR in relation to drinking outcomes
We calculated AE-SR discrepancy scores for each participant, reflecting the difference between AEs and SR on each subscale. We then ran separate multiple regression models examining AE-SR discrepancies on the ascending and descending limbs, respectively, as cross-sectional “predictors” of binge drinking, driving after drinking, and alcohol-related problems. Sex was included as a covariate in all regression models, and alcohol use was included in the model predicting problems.
Results
4.1 Descriptive statistics
Over the past month, participants reported drinking an average total of 59.70 (SD = 48.42) drinks, binge drinking an average of 5.46 (SD = 4.72) times, and driving after drinking an average of 1.5 times (SD = 2.06). Participants reported experiencing an average of 4.44 (SD = 3.27) problems over the past three months, with 17.0% of the sample reporting drinking at a level indicative of requiring treatment (cutoff of 8; Neal et al., 2006).
4.2 Manipulation Check
Consistent with hypotheses, paired samples t-tests indicated that participants reported significantly stronger HIGH+ and LOW+ effects than HIGH- and LOW- effects across the limbs of the BAC (mean values ascending limb: HIGH+ 5.79 [2.09]; LOW+ 7.94 [2.05]; HIGH- 1.38 [1.53]; LOW- 1.20 [1.45]; mean values descending limb: HIGH+ 4.35 [2.28]; LOW+ 7.07 [2.59]; HIGH- 1.13 [1.41]; LOW- 1.04 [1.04]; all p-values < .001).
4.3 Measurement Invariance
4.3.1 Configural Invariance
Using MPLUS, we specified a two-group CFA model (maximum likelihood with robust standard errors) in which the previously identified 4-factor structure was fit simultaneously to the AEAS and SEAS. We set the factor loadings of the metric-setting items to 1.0 and factor means to 0. Remaining model parameters were estimated freely. We used the following statistical cutoffs to determine adequate model fit: Bentler's Comparative Fit (CFI) > .90 (Bentler, 1990), Root Mean Square Error of Approximation (RMSEA) < .07 (Steiger, 2007), and Standardized Root Mean Square Residual (SRMR) < .08 (Hu & Bentler, 1999). Based on these criteria, configural invariance was established (χ2(116) = 184.99; RMSEA = .054; CFI = .956; SRMR = .055).
4.3.2 Metric invariance
We constrained the factor loadings of corresponding AEAS/SEAS items to equality and set latent factor means to zero. When sample sizes are small (i.e., < 200), metric invariance holds when the decrement in model fit between the model evaluating metric invariance and the configurally invariant model does not exceed the following criteria: RMSEA ≥ .010, CFI ≥ -.005, or SRMR ≥ .025 (Chen, 2007). Based on these criteria, AEs and SR were metric invariant (χ2 (126) = 201.87; RMSEA = .054 [Δ RMSEA = .000]; CFI = .952 [Δ CFI = -.004]; SRMR = .061 [Δ SRMR = .006]).
4.3.3 Scalar Invariance
We constrained the factor loadings and intercepts of corresponding AEAS and SEAS items to equality. Latent factor means were estimated freely. Scalar variance exists when the model testing scalar invariance results in a decrement in fit of CFI ≥ -.005, accompanied by a change in RMSEA ≥.010 or in SRMR ≥ .005. Based on these cutoffs, we demonstrated scalar invariance of AEs and SR (χ2 (135) = 218.47; RMSEA = .055 [Δ RMSEA = .001]; CFI = .947 [Δ CFI = -.005]; SRMR = .062 [Δ SRMR = .001]), suggesting that AEs and SR can be compared meaningfully using the AEAS and SEAS.
4.4 Internal Reliability of the AEAS and SEAS Subscales
The AEAS and SEAS subscales evidenced good internal reliability (Cronbach's α [SEAS] ranged from .77-.92 [mean = .85]; Cronbach's α [AEAS] ranged from .78-.94 [mean = .86]).
4.5 Relations between AEs and SR: Bivariate Correlations
Moderate to large correlations were observed between 1) corresponding subscales (See Table 1) and 2) positively valenced subscales. The negatively valued subscales were not correlated significantly.
Table 1. Bivariate Correlations between AEAS and SEAS Subscales.
| SUBJECTIVE RESPONSE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| ASCENDING LIMB | DESCENDING LIMB | |||||||||
|
|
|
|||||||||
| SEASA High+ | SEASA Low+ | SEASA High- | SEASA Low- | SEASD High+ | SEASD Low+ | SEASD High- | SEASD Low - | |||
|
|
|
|
|
|
|
|
|
|||
| EXPECTANCIES | AEASA High+ | .52*** | .29** | -.11 | .01 | AEASD High+ | .53*** | .30** | -.02 | -.08 |
| AEASA Low+ | .36*** | .51*** | -.11 | -.16 | AEASD Low+ | .35*** | .48*** | -.03 | .09 | |
| AEASA High- | .09 | -.12 | .50*** | .09 | AEASD High- | .06 | -.08 | .62*** | .11 | |
| AEASA Low - | .08 | .09 | -.06 | .44*** | AEASD Low - | -.04 | .09 | .07 | .48*** | |
Note.
p < .05
p < .10
p < .001
Sample sizes ranged from 101 to 102 participants for each correlation. Abbreviations are SEASA = Subjective Effects of Alcohol Scale, Ascending Limb; SEASD = Subjective Effects of Alcohol Scale, Descending Limb; AEASA = Anticipated Effects of Alcohol Scale, Ascending Limb; AEASD = Anticipated Effects of Alcohol Scale, Descending Limb.
Table 2. Paired Samples t-tests evaluating the accuracy of Alcohol Expectacncies by Limb of the Blood Alcohol Curve.
| ASCENDING LIMB | DESCENDINGLIMB | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
||||||||||
| Mean | Std. Dev. | t | df | Cohen's d | Mean | Std. Dev. | t | df | Cohen's d | ||
|
|
|
||||||||||
| AE HIGH + | 27.92 | 7.25 | AE HIGH + | 23.25 | 9.22 | ||||||
| SR HIGH + | 24.97 | 7.84 | 1.49 | 100 | .39*** | SR HIGH + | 19.67 | 8.03 | 1.91 | 100 | .41*** |
|
|
|
||||||||||
| AE LOW + | 16.17 | 5.78 | AE LOW + | 16.92 | 5.42 | ||||||
| SR LOW + | 18.08 | 5.81 | -3.05 | 100 | -.33*** | SR LOW + | 17.63 | 5.85 | -1.85 | 100 | -.13 |
|
|
|
||||||||||
| AE HIGH - | 7.28 | 5.50 | AE HIGH - | 6.66 | 5.58 | ||||||
| SR HIGH - | 4.61 | 5.08 | 1.62 | 100 | .50*** | SR HIGH - | 3.98 | 4.67 | 1.78 | 100 | .52*** |
|
|
|
||||||||||
| AE LOW - | 7.48 | 6.02 | AE LOW - | 7.70 | 7.25 | ||||||
| SR LOW - | 4.56 | 4.75 | 1.77 | 100 | .54*** | SR LOW - | 4.31 | 4.60 | 2.12 | 100 | .56*** |
Note.
p < .001
Bold denotes statistically significant higher average subscale scores
4.6 The Accuracy of Alcohol Expectancies: Paired Samples t-Tests
HIGH+, HIGH-, and LOW- AEs reflected moderate overestimates of SR (See Table 2). LOW+ AEs reflected modest underestimates of SR on the ascending limb and were relatively accurate on the descending limb.
4.7 Discrepancies between AEs and SR Predict Alcohol Outcomes
AE-SR discrepancies accounted for significant variance in binge drinking (13% ascending; 16% descending), driving after drinking (7% ascending), and alcohol-related problems (6% ascending; 8% descending; see Table 3). Overestimating HIGH- effects was associated with more frequent binge drinking and alcohol-related problems (both limbs) while overestimating LOW- effects on the ascending limb was associated with less frequent binge drinking and fewer alcohol-related problems (at a trend level, p = .09). Overestimating LOW+ and LOW- effects on the ascending limb was associated with less frequent driving after drinking, whereas overestimating HIGH+ effects was associated with more frequent driving after drinking (at a trend level, p = .06).
Table 3. AE-SR Discrepancies Predict Binge Drinking, Driving after Drinking, and Alcohol-Related Problems.
| ALCOHOL CONDITION | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| DISCREPANCIES ON ASCENDING LIMB SUBSCALES | ||||||||||||
|
| ||||||||||||
| Binge Drinking Episodes | Driving after Drinking | Alcohol-Related Problems | ||||||||||
|
|
|
|
||||||||||
| Predictors | ΔR2 | F | df | β | ΔR2 | F | df | β | ΔR2 | F | df | β |
| STEP 1 | .00 | 13.38 | (1, 97) | .01 | 1.30 | (2, 92) | .06* | 3.87 | (2, 96) | |||
| Sex (ref. female) | .35*** | .14 | .01 | |||||||||
| Drinking (Freq) | -- | .03 | .27** | |||||||||
| STEP 2 | .13** | 4.66 | (4, 93) | .07* | 2.78 | (4, 88) | .06* | 2.52 | (4, 92) | |||
| HIGH + | .09 | .22T | -.17 | |||||||||
| LOW + | -.15 | -.24* | .03 | |||||||||
| HIGH - | .26* | .14 | .30** | |||||||||
| LOW - | -.39*** | -.24* | -.18T | |||||||||
|
| ||||||||||||
| DISCREPANCIES ON DESCENDING LIMB SUBSCALES | ||||||||||||
|
| ||||||||||||
| STEP 2 | .16*** | 5.53 | (4, 93) | .00 | .77 | (4, 88) | .08* | 3.09 | (4, 92) | |||
| HIGH + | -.04 | .09 | .04 | |||||||||
| LOW + | -.02 | -.16 | -.16 | |||||||||
| HIGH - | .41*** | .11 | .29** | |||||||||
| LOW - | -.36*** | -.02 | -.16 | |||||||||
Note.
p < .001
p < .01
p < .05
superscript “T” p < .01. Abbreviations within the table are: AE-SR discrepancy between alcohol expectancies and subjective response; HIGH+ = high arousal positive; LOW+ = low arousal positive; HIGH- = high arousal negative; LOW- = low arousal negative. Step 1 variables included sex for all models, with females as the reference group. Drinking frequency was included in Step 1 for the models assessing driving after drinking and alcohol-related problems. Step 2 variables were the discrepancy scores. Demographic covariate information is not presented for the descending limb variables because it was the same as that presented for the ascending limb variables.
Discussion
The current study was the first to examine the AE-SR relationships using measures designed and validated specifically for this purpose. Consistent with nomothetic hypotheses, AEs and SR were related yet distinct constructs. Results indicated that the accuracy of AEs seems to depend on both the arousal and valence of the alcohol effects in question; while individuals generally overestimated HIGH+, LOW+, HIGH- effects, they modestly underestimated LOW+ effects on the ascending limb and were quite accurate on the descending limb. As hypothesized, there was considerable individual variability in the accuracy of AEs.
Importantly, individual differences in AE-SR discrepancies were cross-sectionally related to several alcohol outcomes. Results suggested that, where significant effects emerged, overestimating sedative effects, irrespective of their valence, was associated with less engagement in dangerous alcohol-related behaviors, whereas overestimating high arousal effects, irrespective of their valence, was associated with increased negative alcohol-related outcomes. Overestimates of HIGH+ effects on the ascending limb were associated with driving after drinking (at a trend level). If the observed pattern of findings were replicated in a real-world setting, it suggests that anticipating stronger HIGH+ effects may partially obscure experiences of alcohol-induced impairment, leading to misperceptions about driving ability. Finally, a particularly novel finding was that overestimating HIGH– effects universally was associated with more frequent binge drinking and with more alcohol-related problems. Given the lack of a precedent, it is unclear exactly why this pattern emerged. However, the results may reflect expectancy effects that drive aggression or risk taking behavior following alcohol use, leading to negative consequences.
These preliminary results regarding AE-SR discrepancies may have important implications for the development of future prevention and treatment efforts. Challenging the veracity of (presumably) inflated HIGH+ AEs has been shown to reduce college student drinking modestly across a number of Alcohol Expectancy Challenge Studies (Scott-Sheldon, Terry, Carey, Garey, & Carey, 2012), but the current study suggests that an Alcohol Expectancy Challenge paradigm that assesses and subsequently challenges AE-SR discrepancies for high arousal positive and negative effects may be more effective in reducing the prevalence of heavy drinking and related negative consequences. While challenging the veracity of inflated HIGH+ effects intuitively makes sense, as mentioned previously, it is not entirely clear why inflated HIGH- AEs are associated with heavy drinking and the experience of alcohol-related problems. If the development of HIGH- AEs is, in fact, linked to the previous experience of negative drinking consequences, social learning theory and principles of operant conditioning would suggest that if an individual were learning from his or her prior experiences, expecting HIGH-outcomes should decrease drinking behavior, and, in turn, negative alcohol-related consequences. However, the fact that overestimating these effects is associated with increased alcohol use and alcohol-related problems is problematic. Although future research is needed on this topic, it may be that a subset of individuals who experience HIGH- effects overestimate the influence that alcohol has on their behavior, perhaps serving as an explanation or even an excuse to engage in further aggressive behavior while under the influence of alcohol. Thus, challenging inflated HIGH- AEs may help to encourage personal responsibility and recognition of problematic drinking behavior.
While the current study has numerous strengths, several limitations merit note. First, the study relied on self-report data, which are limited by participants' insight and willingness to respond honestly. Second, the data were cross-sectional, and future research is needed to determine whether AE-SR discrepancies prospectively predict alcohol-related outcomes of interest. Third, study participants were relatively heavy drinkers, with the average participant binge drinking nearly 5.5 times per month, and the majority of study participants were male. Given the novelty of examining AE-SR discrepancies, it is impossible to know the extent to which these results generalize to other drinker types (e.g., light drinkers, dependent drinkers, women). Fourth, AE-SR discrepancies also were based on a BAL of .08, which may underestimate the peak BAL typically reached by a subset of heavy-drinking participants. Future work is needed to determine the extent to which AEs and SR are discrepant at lower and higher doses of alcohol and if these discrepancies relate differentially to typical drinking behavior and/or other alcohol use outcomes. Fifth, participants' AEs may be linked, in part, to their preferred alcoholic beverage (e.g., beer versus vodka). Thus, the discrepancies observed in the current study could be influenced by the fact that all participants consumed the same vodka-based drink. Future research can determine whether AEs and SR align more closely when participants consume their preferred beverage. Finally, our results are limited to AE-SR discrepancies associated with a single drinking episode. Expectancy theory indicates that AEs develop over the course of time, and thus, are thought to be relatively stable. However, actual drinking experiences may vary based on a number of situational factors (e.g., drinking in a bar versus at home; drinking alone versus with friends). Future research is needed to determine whether different patterns of discrepancies confer alcohol-related risk or protection depending on situational factors.
Conclusions
The current study is the first to evaluate the relationship between AEs and SR to alcohol using assessment tools explicitly designed and validated to permit comparisons of these constructs. Thus, we can assert with a sufficient level of statistical confidence that AEs and SR are related constructs, with modest to moderate overlap. Consistent with Expectancy Theory (e.g, Darkes & Goldman, 1993), participants generally anticipated stronger HIGH+ effects than they experienced in the lab, although novel study findings indicated that that overestimates appear to extend to negative effects as well. Extending prior research suggesting that overestimates of positive high arousal effects may confer risk for drinking (e.g., Darkes & Goldman, 1993), the current study indicates that overestimates of both high arousal positive and high arousal negative AEs were associated cross-sectionally with negative alcohol outcomes. These promising study results suggest that further meaningful gains can be achieved by examining the intersection of AEs and SR using the AEAS and SEAS.
Highlights.
Alcohol expectancies and subjective response are theoretically related constructs
New measures of these constructs were scalar measurement invariant
Expectancies generally overestimated subjective response to alcohol
Inaccurate beliefs for high arousal alcohol effects conferred alcohol-related risk
Inaccurate beliefs for low arousal alcohol effects served protective functions
Acknowledgments
This research was supported by a grant from NIH (1R21AA016386).
Statement 1: Role of Funding Sources: This research was supported by a grant from the NIH (1R21AA016386). The NIH had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Footnotes
Meghan E. Morean, Ph.D., Department of Psychology, Oberlin College and Department of Psychiatry, Yale University School of Medicine; William R. Cobin, Ph.D., Department of Psychology, Arizona State University; Teresa A Treat, Ph.D., Department of Psychology, University of Iowa
Statement 2: Contributors Dr. Corbin secured study funding and was responsible for the design of the larger study. Dr. Morean developed and tested the hypotheses reported in the manuscript, ran statistical analyses, and wrote the primary manuscript draft. Dr. Treat provided statistical support and Drs. Treat and Cobrin reviewed drafts of the manuscript. All authors have approved the submitted version of the manuscript.
Statement 3: Conflict of Interest Drs. Morean, Corbin, and Treat declare that they have no conflicts of interest.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Meghan E. Morean, Oberlin College, Department of Psychology, 120 W. Lorain St, Oberlin, OH 44074, 440-775-8257; Yale School of Medicine, Department of Psychiatry, 34 Park Street, New Haven, CT 06519
William R. Corbin, Arizona State University, Department of Psychology, 651 E. University Drive, P.O. Box 871104, Tempe, AZ 85287
Teresa A. Treat, University of Iowa, Department of Psychology, E11 Seashore Hall, Iowa City, Iowa 52242
References
- Bandura A. In: Model of causality in social learning theory, in Cognition and psychotherapy. Second. Freeman A, Mahoney MJ, Devito P, Martin D, editors. Springer; New York: 2004. pp. 25–44. [Google Scholar]
- Bandura A. In: Social cognitive theory, in Handbook of theories of social psychology Volume 1. Lange PAM, Kruglanski AW, Higgens ET, editors. Sage; Thousand Oaks: 2012. pp. 349–374. [Google Scholar]
- Barrett P. Structural equation modelling: adjudging model fit. Pers Indiv Differ. 2007;425:815–824. DOI: http://dx.doi.org/10.1016/j.paid.2006.09.018. [Google Scholar]
- Beck AT. The evolution of the cognitive model of depression and its neurobiological correlates. Am J Psychiat. 2008;165(8):969–977. doi: 10.1176/appi.ajp.2008.08050721. [DOI] [PubMed] [Google Scholar]
- Beck I, Smits DJ, Claes L, Vandereycken W, Bijttebier P. Psychometric evaluation of the behavioral inhibition/behavioral activation system scales and the sensitivity to punishment and sensitivity to reward questionnaire in a sample of eating disordered patients. Pers Indiv Differ. 2009;47(5):407–412. doi: http://dx.doi.org/10.1016/j.paid.2009.04.007. [Google Scholar]
- Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Brown SA, Goldman MS, Inn A, Anderson LR. Expectations of reinforcement from alcohol: Their domain and relation to drinking patterns. J Consult Clin Psych. 1980;48:419–426. doi: 10.1037//0022-006x.48.4.419. [DOI] [PubMed] [Google Scholar]
- Byrne BM, Watkins D. The issue of measurement invariance revisited. J Cross Cult Psychol. 2003;34(2):155–175. doi: 10.1177/0022022102250225. [DOI] [Google Scholar]
- Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equ Modeling. 2007;14(3):464–504. [Google Scholar]
- Chen FF. What Happens If We Compare Chopsticks With Forks? The Impact of Making Inappropriate Comparisons in Cross-Cultural Research. J Pers Soc Psychol. 2008;95(5):1005–1018. doi: 10.1037/A0013193. [DOI] [PubMed] [Google Scholar]
- Darkes J, Goldman MS. Expectancy challenge and drinking reduction: experimental evidence for a mediational process. J Consult Clin Psych. 1993;61(2):344–353. doi: 10.1037//0022-006x.61.2.344. [DOI] [PubMed] [Google Scholar]
- Darkes J, Goldman MS. Expectancy challenge and drinking reduction: process and structure in the alcohol expectancy network. Exp Clin Psychopharm. 1998;6(1):64–76. doi: 10.1037//1064-1297.6.1.64. [DOI] [PubMed] [Google Scholar]
- Fals-Stewart W, O'Farrell TJ, Freitas TT, McFarlin SK, Rutigliano P. The timeline followback reports of psychoactive substance use by drug-abusing patients: psychometric properties. J Consult Clin Psych. 2000;68(1):134–144. doi: 10.1037//0022-006x.68.1.134. [DOI] [PubMed] [Google Scholar]
- Fromme K, Dunn ME. Alcohol expectancies, social and environmental cues as determinants of drinking and perceived reinforcement. Addict Behav. 1992;17(2):167–177. doi: 10.1016/0306-4603(92)90021-m. [DOI] [PubMed] [Google Scholar]
- Fromme K, Stroot EA, Kaplan D. Comprehensive effects of alcohol: Development and psychometric assessment of a new expectancy questionnaire. Psychol Assessment. 1993;5(1):19–26. [Google Scholar]
- Hu LT, Bentler PM. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- Michalczuk R, Bowden-Jones H, Verdejo-Garcia A, Clark L. Impulsivity and cognitive distortions in pathological gamblers attending the UK National Problem Gambling Clinic: a preliminary report. Psychol Med. 2011;41(12):2625–35. doi: 10.1017/s003329171100095x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morean ME, Corbin WR, Treat TA. The Anticipated Effects of Alcohol Scale: Development and psychometric evaluation of a novel assessment tool for measuring alcohol expectancies. Psychol Assessment. 2012;24(4):1008–23. doi: 10.1037/a0028982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morean ME, Corbin WR, Treat TA. The Subjective Effects of Alcohol Scale: Development and Psychometric Evaluation of a Novel Assessment Tool for Measuring Subjective Response to Alcohol. Psychol Assessment. 2013;25(3):780–95. doi: 10.1037/a0032542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neal DJ, Corbin WR, Fromme K. Measurement of alcohol-related consequences among high school and college students: application of item response models to the Rutgers Alcohol Problem Index. Psychol Assessment. 2006;18(4):402–414. doi: 10.1037/1040-3590.18.4.402. [DOI] [PubMed] [Google Scholar]
- Scott-Sheldon LA, Terry DL, Carey KB, Garey L, Carey MP. Efficacy of expectancy challenge interventions to reduce college student drinking: a meta-analytic review. Psychol Addict Behav. 2012;26(3):393–405. doi: 10.1037/a0027565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shoal GD, Giancola PR. The relation between social problems and substance use in adolescent boys: an investigation of potential moderators. Exp Clin Psychopharm. 2005;13(4):357–366. doi: 10.1037/1064-1297.13.4.357. [DOI] [PubMed] [Google Scholar]
- Sobell LC, Sobell MB. Alcohol Consumption Measures. In: Allen JP, Wilson VB, editors. Assessing alcohol problems: a guide for clinicians and researchers. Second. U.S. Dept. of Health and Human Services, Public Health Service, National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism; Bethesda: 2003. pp. 78–99. [Google Scholar]
- Southwick LL, Steele CM, Marlatt GA, Lindell MK. Alcohol-related expectancies: Defined by phase of intoxication and drinking experience. J Consult Clin Psychol. 1981;49:713–721. doi: 10.1037//0022-006x.49.5.713. [DOI] [PubMed] [Google Scholar]
- Steiger JH. Understanding the limitations of global fit assessment in structural equation modeling. Pers Individ Dif. 2007;42:893–898. [Google Scholar]
- Vandenberg RJ, Lance CE. A review and synthesis of the measurement invariance literature: Suggestions, practices, and recommendations for organizational research. Organ Res Meth. 2000;3(1):4–69. [Google Scholar]
- Wall AM, Thrussell C, Lalonde RN. Do alcohol expectancies become intoxicated outcomes? A test of social-learning theory in a naturalistic bar setting. Addict Behav. 2003;28(7):1271–1283. doi: 10.1016/s0306-4603(02)00253-8. [DOI] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the Assessment of Adolescent Problem Drinking. J Stud Alcohol Drugs. 1989;50(1):30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]
- Wiers RW, van de Luitgaarden J, van den Wildenberg E, Smulders FT. Challenging implicit and explicit alcohol-related cognitions in young heavy drinkers. Addiction. 2005;100(6):806–819. doi: 10.1111/j.1360-0443.2005.01064.x. [DOI] [PubMed] [Google Scholar]