

Abstract
Objective:
The aim of this study is to evaluate the effect of zinc and omega-3 supplements as adjunctive drugs in the treatment of attention-deficit/hyperactivity disorder (ADHD) of children.
Methods:
This study is a randomized, double-blind clinical trial conducted on 150 children aged 6–15 years old that diagnosed as new cases of ADHD. Study subjects were evaluated for 8 weeks. Besides of drug of choice (methylphenidate) for the ADHD, patients received placebo in the control group (n = 50), zinc sulfate in second group (n = 50), and omega-3 (n = 50) in third group. Clinical improvement was checking by Conners’ Parent and Teacher Rating Scales before and in 2nd, 4th, and 8th week of treatment. Results were analyzed with SPSS version 16 software.
Findings:
In this study, mean scores of Conners’ scale showed significant improvement during treatment in the zinc group compared to control group in children that affected to attention-deficit disorder subtype of ADHD (P = 0.02). Moreover, in omega-3 group, better clinical response was seen than other groups (P < 0.05). However, there was no significant difference between omega-3 group compared to placebo group in the mean scores of Conners’ scale (P = 0.89).
Conclusion:
Zinc supplementation accompanied by the main treatment significantly improves symptom of attention-deficit disorder subtype of ADHD. However, omega-3 supplementation was superior to zinc and placebo in the clinical improvement of ADHD.
Keywords: Attention-deficit/hyperactivity disorder, complementary treatment, Methylphenidate, Omega-3, Zinc
INTRODUCTION
Attention-deficit/hyperactivity disorder (ADHD) is the most common neurobehavioral disorder of childhood. This disorder is one of the most chronic common disorders, which influences school age children and indicates prevalence between 5% and 10% in various communities.[1]
This disorder has the most prevalence between 6 and 12 aged children which includes the 1st year of education. Lack of diagnosis and on time treatment of this disorder can cause irreparable effects in educational and the professional future of patients and can have devastating effects on surrounding networks including members, school classmates, and playmates.[2] Two branches of factors including background factors and environmental factors such as lack of some micronutrients have been propounded in the pathogenesis of disease.[3]
The main treatment of ADHD is the use of stimulant drugs such as methylphenidate. However, it is important to note that patients of this disorder also lack suitable clinical response after the beginning effects of the drug. In some cases, this is related to the lack of micronutrients such as omega-3 and zinc supplementation in diet.[4] Therefore, true treatment of the disease can create a suitable clinical response in affected children.[5] The vital role of zinc has been propounded in frequency, and it has shown a variety of signs among patients that were affected by ADHD.[6] Akhondzadeh et al. in a double-blind study used zinc and placebo as complementary therapy, which at the end of the experiment confirmed zinc as the complementary therapy cure for children with ADHD disorder.[7] Bilici et al. have performed a study that has proven zinc has a tendency preference lonely as compared with placebo in decrease of signs of hyperactivity and being social in affected children to ADHD.[8] Dodig-Curkovic et al., have performed a study which indicated that the remedy with zinc supplementation is effective in the improvement of signs of disease in children that affected to ADHD and suffering from lack of zinc (or blood zinc).[9] Arnold et al. suggested that the lack of zinc in blood, urine, red blood cell, hair, and nail of children with ADHD has been proved.[10]
Essential fatty acids including omega-3, omega-6, and arachidonic acid are necessary for nerve evolution. Omega-3 consists of two essential fatty acids which are eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). DHA is essential for nerve evolution in the period of pregnancy and suckling. Bélanger et al.[11] and Antalis et al.[12] conducted studies that proved consumption of omega-3 can be effective at improving sign of ADHD in diagnosed patients.[5,11,12,13] Unfortunately, as a result of the “dietary basket” of children in our country, many lacks in essential micronutrients in some of the social levels that have been observed.
Research has indicated and proved that in the frame of a clinical experiment the role of omega-3 and zinc supplementations serve as complementary therapy in ADHD. The current study aimed to evaluate the impact of zinc and omega-3 supplements as adjunctive drugs in the treatment of children affected with ADHD.
METHODS
This study was a randomized, double-blind clinical trial study including a placebo group which took 9 months to complete (from August to December 2012) in Amirkabir Hospital of Arak, Iran. It was registered with No. IRCT20110416201N1 at Iranian Registry of Clinical Trials (IRCT: http//www.irct.ir).
At first, during a screening project which was done by a trained team of staffs on primary and middle school students of Arak, children who diagnosed as ADHD based on 18-question questionnaire of Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition-Text Revised (DSM-IV-TR)[1,14] were selected, interviewed, and then referred to a psychiatrist for further confirmation. Finally, 150 children were selected and randomly assigned to one of the three subgroups. Before conducting the study, informed consent was shared with the children's parents, and sufficient explanations were presented such as the drugs used and their side effects. Inclusion criteria were set for children of 6–15 years old, with a recent diagnosis of ADHD based on DSM-IV-TR criteria, no history of psychiatric drug usage and no history of other psychiatric disorders, no limitation or sensitivity for the use of zinc sulfate and omega-3, and absence of mental retardation. Moreover, exclusion criteria included children who develop acute systemic diseases, who cannot use oral medication, who refuse the medication due to side effects, and whose method of treatment has been changed.
A demographic questionnaire for all children (including age, birth weight, previous medical history, family history, habitat specifications, and family income) was completed prior to the conduction of the study. For all children in each three groups, the main treatment of the disease (Methylphenidate, Ritalin®; Produced by Novartis Pharmaceutical Company in Switzerland) was prescribed based on child's weight (10 mg daily for children under 20 kg; 10 mg, twice a day for children over 20 kg).
Group C (control group; n = 50) was administered with daily Ritalin® plus placebo (whitish color capsule containing sugar, produced in one central pharmacy in Arak, as the same shape and volume of omega-3 capsules). Group O (omega-3 group; n = 50) was administered with daily Ritalin® plus one omega-3 capsule (produced by Zahravi Pharmaceutical Company in Iran) based on the instruction of 100 mg eicosapentaenoic fatty acid for children <25 kg, 200 mg for 26–35 kg, and 400 mg for children >35 kg/day, respectively. Group Z (zinc group; n = 50) was administered with daily Ritalin® plus one zinc sulfate capsule (containing 22 mg zinc sulfate, produced by Razak Pharmaceutical Company in Iran, and capsuled in one Central Pharmacy in Arak).
Selection of patients in all groups was done based on block randomization. The size of each block was considered as 6. In the meantime, with attention to the tests of DSM-IV-TR, all patients were located in one of three groups based on subgroup of disease (included attention disorder subgroup, hyperactivity subgroup, and mixed type).
The Conners’ Parent and Teacher Rating Scales were filled-out for each subject in the beginning of study and then every 2 weeks (0, 2, 4, and 8 weeks) after giving necessary explanations to the parents and teachers. Finally, the average scores of the questionnaire were calculated and considered as criterion of clinical response. Frequency tables and inferential statistics were used for identifying the relationship among qualitative variables. In addition, Chi-square test, analysis of variance, analysis of variance for repeated measurements, and paired t-test were used where applicable. P < 0.05 was considered significant.
RESULTS
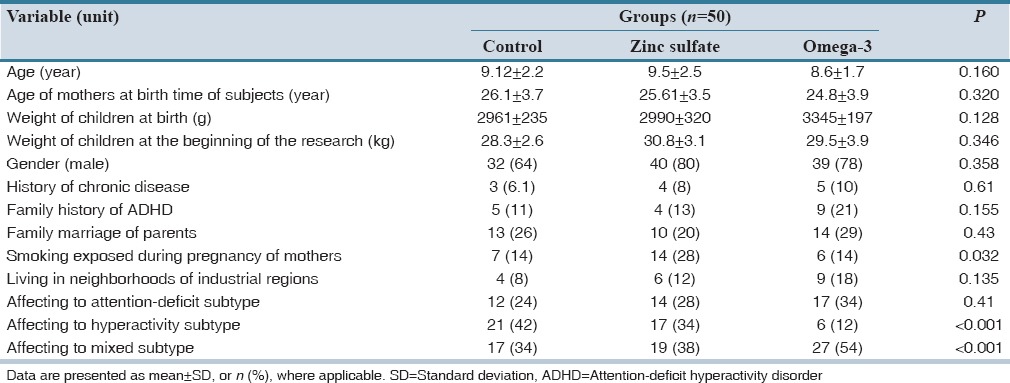
In this project, 150 children and adolescents participated. Details of participant's characteristics and baseline measurements are presented in Table 1. According to Table 1, the smoking exposure in pregnancy was higher in mothers of Z group (P = 0.032). Moreover, affecting to hyperactivity and mixed subtypes of ADHD was more prevalent in C and O groups, respectively (P < 0.001).
Table 1.
Baseline measurements comparison of study subjects
The average scores of Conners’ scale before beginning of drugs (week 0) were compared by the analysis of variance among three groups while there was no significant difference among these groups (P = 0.07). Furthermore, the differences between average scores of Conners’ scale in each time of 2nd, 4th, and 8th week after beginning of treatment in children was not significant among three groups (P > 0.05). However, the mean score changes in 2nd, 4th, and 8th week after beginning of the treatment were compared by analysis of variance for repeated measures and showed a significant decreasing trend in all three groups as presented in Table 2 (P < 0.01).
Table 2.
The average scores of Conners’ scale in omega-3, Zinc and control groups at baseline and 2nd, 4th, 8th weeks during treatment

Moreover, subgroup analysis in children with attention-deficit disorder showed that in comparison of C group with Z group, a significant difference was found in the average scores of Conners’ scales at 0, 2, 4, and 8 weeks (P = 0.02). In addition, in comparison of Z and O groups, better clinical response was seen in O group average scores of Conners’ scale in 0, 2, 4, and 8 weeks (P = 0.03). However, in comparison between Z and O groups in children with mixed subtype of ADHD, the difference between the average scores of Conners’ scale was not significant (P = 0.21).
DISCUSSION
The impact of lack in omega-3 fatty acid has been propounded in many clinical problems such as cognitive disorder, depression, neurotic disorders, asthma, and inflammatory diseases.[2,3,4,11] ADHD patients in an omega-3 group beside the main drug (methylphenidate) have not significant difference compared to C group in Conners’ scales mean in all periods during 8 weeks after treatment. However, according to our results, patients who had taken zinc with the main drug, showed a significant differences in mean scores of Conners’ scales during the time of treatment comparing to C group and this difference was more noticeable in subtype of attention-deficit. This finding was similar to Bilici et al.[8] study on 400 children with ADHD that treated with 150 mg/day zinc for 12 weeks and showed that signs of patients were decreased during treatment compared to placebo. Although that study showed a decreasing effect of zinc on signs of hyperactivity and was not effective on signs of attention-deficit subtype. Nevertheless, the effect of zinc was showed on improvement of children with attention-deficit subtype in our study. Another study by Akhondzadeh et al.[7] assessed the effect of zinc supplement on 44 children 5–11-year-old who affected to ADHD for 6 weeks and received the same results of our study. Moreover, other studies demonstrated that zinc is as a cofactor in over than 100 enzymes in the body and is effective on regulating the metabolism of melatonin. In addition, melatonin plays a significant role in regulation of dopamine that is effective in treating children with ADHD.[9,15] Yorbik et al. results also suggested that plasma level of zinc is effective on better information processing of children with ADHD and plays an important role in the improvement of the ADHD signs.[16] In addition, Oner et al. results showed that the impact of zinc in patients with hyperactivity symptoms of ADHD.[17]
According to our results, significant differences were seen in the scores by Conners’ scales during treatment in two type of ADHD. These results were in controversy with Bélanger et al.[11] results that showed the omega-3 has a better effect than placebo in controlling of ADHD signs. However, the intervention was EPA 20–25 mg/kg comparing to omega-3 and that study conducted on 26 patients, 6–11-year-old for 8 weeks. Other studies, which concluded regarding omega-3 and omega-6 compounds showed a significant reduction in symptoms of an attention-deficit subtype of ADHD and improvement in emotional and behavioral problems.[5,18,19] Moreover, a review article[20] founded that lack of essential fatty acids plays a role in the exacerbation of ADHD symptoms that are consistent with our study.
Regarding our results as well as due to lack of different micronutrients such as zinc in Iran, use of zinc supplement in addition to main medications (methylphenidate) in children with ADHD has been recommended. In addition, it seems that more studies are necessary in all subtypes of ADHD for more accurate results regarding obvious differences in the results of our study in hyperactivity, attention-deficit, and mixed subgroups. Moreover, since omega-3 is an effective supplement in low economic families, future studies suggested in to assess the omega-3 effect on ADHD patients.
AUTHORS’ CONTRIBUTION
SB: Contributions to the acquisition and analysis of data; drafting of the manuscript and final approval of the manuscript. MA: Contributions to the conception and design of the research; analysis and interpretation of data; final approval of the manuscript. H Sh: Contributions to the conception and design of the research analysis; interpretation of data; final approval of the manuscript. EM: Contributions to the conception and design of the research; interpretation of data; final approval of the manuscript. FD: Contributions to the conception and design of the research analysis; interpretation of data; final approval of the manuscript.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This study borrowed from project no. 522 of Arak University of Medical Sciences, it is necessary to appreciate of honored educational and research assistant of Arak University of Medical Sciences, the whole staff of Arak, Amirkabir Hospital, those children whose attended in the this project and their parents.
REFERENCES
- 1.Cunningham NR, Jensen P. Nelson Textbook of pediatrics. In: Kliegman RM, Stanton BF, Geme JW III, Schor NF, Behrman RE, editors. 19th ed. Philadelphia: WB Saunders; 2011. [Google Scholar]
- 2.Krull KR, Augustyn M, Torchia MM. Attention deficit hyperactivity disorder in children and adolescents: Epidemiology and pathogenesis. UpToDate. [Last Updated on 2015 Oct 13]. Available from: http://www.uptodate.com/contents/attention-deficithyperactivity-disorder-in-children-and-adolescentstreatment-with-medications .
- 3.Greenbaum LA. 18th ed. Philadelphia: Saunders; 2007. Micronutrient Mineral Deficiencies. Nelson Textbook of Pediatrics. [Google Scholar]
- 4.Stettler N, Bhatia J, Parish A, Stallings V. 19th ed. Philadelphia, PA: Elsevier Saunders; 2011. Feeding healthy infants, children, and adolescents. Nelson Textbook of Pediatrics. [Google Scholar]
- 5.Busch B. Polyunsaturated fatty acid supplementation for ADHD? Fishy, fascinating, and far from clear. J Dev Behav Pediatr. 2007;28:139–44. doi: 10.1097/01.DBP.0000267560.34199.e0. [DOI] [PubMed] [Google Scholar]
- 6.Abrams S. Zinc deficiency and supplementation in children and adolescents. UpToDate. 2007. [Last updated on 2014 Jul 24]. URL: http://www.uptodate.com/contents/zinc-deficiency-and-supplementation-inchildren-and-adolescents .
- 7.Akhondzadeh S, Mohammadi MR, Khademi M. Zinc sulfate as an adjunct to methylphenidate for the treatment of attention deficit hyperactivity disorder in children: A double blind and randomized trial. BMC Psychiatry. 2004;4:9. doi: 10.1186/1471-244X-4-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bilici M, Yildirim F, Kandil S, Bekaroglu M, Yildirmis S, Deger O, et al. Double-blind, placebo-controlled study of zinc sulfate in the treatment of attention deficit hyperactivity disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2004;28:181–90. doi: 10.1016/j.pnpbp.2003.09.034. [DOI] [PubMed] [Google Scholar]
- 9.Dodig-Curkovic K, Dovhanj J, Curkovic M, Dodig-Radic J, Degmecic D. The role of zinc in the treatment of hyperactivity disorder in children. Acta Med Croatica. 2009;63:307–13. [PubMed] [Google Scholar]
- 10.Arnold LE, Bozzolo H, Hollway J, Cook A, DiSilvestro RA, Bozzolo DR, et al. Serum zinc correlates with parent- and teacher- rated inattention in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2005;15:628–36. doi: 10.1089/cap.2005.15.628. [DOI] [PubMed] [Google Scholar]
- 11.Bélanger SA, Vanasse M, Spahis S, Sylvestre MP, Lippé S, L’heureux F, et al. Omega-3 fatty acid treatment of children with attention-deficit hyperactivity disorder: A randomized, double-blind, placebo-controlled study. Paediatr Child Health. 2009;14:89–98. doi: 10.1093/pch/14.2.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Antalis CJ, Stevens LJ, Campbell M, Pazdro R, Ericson K, Burgess JR. Omega-3 fatty acid status in attention-deficit/hyperactivity disorder. Prostaglandins Leukot Essent Fatty Acids. 2006;75:299–308. doi: 10.1016/j.plefa.2006.07.004. [DOI] [PubMed] [Google Scholar]
- 13.Schmidt S, Stahl F, Mutz KO, Scheper T, Hahn A, Schuchardt JP. Transcriptome-based identification of antioxidative gene expression after fish oil supplementation in normo-and dyslipidemic men. Nutr Metab. 2012;9:7075–9. doi: 10.1186/1743-7075-9-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Toplak ME, Pitch A, Flora DB, Iwenofu L, Ghelani K, Jain U, et al. The unity and diversity of inattention and hyperactivity/impulsivity in ADHD: Evidence for a general factor with separable dimensions. J Abnorm Child Psychol. 2009;37:1137–50. doi: 10.1007/s10802-009-9336-y. [DOI] [PubMed] [Google Scholar]
- 15.Lepping P, Huber M. Role of zinc in the pathogenesis of attention-deficit hyperactivity disorder: Implications for research and treatment. CNS Drugs. 2010;24:721–8. doi: 10.2165/11537610-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 16.Yorbik O, Ozdag MF, Olgun A, Senol MG, Bek S, Akman S. Potential effects of zinc on information processing in boys with attention deficit hyperactivity disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32:662–7. doi: 10.1016/j.pnpbp.2007.11.009. [DOI] [PubMed] [Google Scholar]
- 17.Oner O, Oner P, Bozkurt OH, Odabas E, Keser N, Karadag H, et al. Effects of zinc and ferritin levels on parent and teacher reported symptom scores in attention deficit hyperactivity disorder. Child Psychiatry Hum Dev. 2010;41:441–7. doi: 10.1007/s10578-010-0178-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Huss M, Völp A, Stauss-Grabo M. Supplementation of polyunsaturated fatty acids, magnesium and zinc in children seeking medical advice for attention-deficit/hyperactivity problems – An observational cohort study. Lipids Health Dis. 2010;9:105. doi: 10.1186/1476-511X-9-105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sinn N. Polyunsaturated fatty acid supplementation for ADHD symptoms: Response to commentary. J Dev Behav Pediatr. 2007;28:262–3. doi: 10.1097/DBP.0b013e3180de4cd5. [DOI] [PubMed] [Google Scholar]
- 20.Rojas NL, Chan E. Old and new controversies in the alternative treatment of attention-deficit hyperactivity disorder. Ment Retard Dev Disabil Res Rev. 2005;11:116–30. doi: 10.1002/mrdd.20064. [DOI] [PubMed] [Google Scholar]