

Abstract
Bronchiolitis, an infection of the lower respiratory tract, is the leading cause of infant and child hospitalization in the United States. Therapeutic options for management of bronchiolitis are limited. Hypertonic saline inhalation therapy has been studied in numerous clinical trials with mixed results. In 2014, the American Academy of Pediatrics (AAP) published updated guidelines on the diagnosis and management of bronchiolitis, which include new recommendations on the use of hypertonic saline. We reviewed all published clinical trials mentioned in the 2014 AAP guidelines, as well as additional trials published since the guidelines, and critically evaluated each trial to determine efficacy, safety, and expectations of hypertonic saline inhalation therapy. A total of 2682 infants were studied over the course of 22 clinical trials. Nine trials were carried out in the outpatient/clinic/emergency department and 13 in the inpatient setting. We agree with the AAP guidelines regarding the recommendation to use nebulized hypertonic saline for infants hospitalized with bronchiolitis, with the expectation of reducing bronchiolitis scores and length of stay when it is expected to last more than 72 hours. However, we also believe there might be an advantage for hypertonic saline in reducing admission rates from the emergency department, based on close examination of the results of recent trials. This review also highlights important gaps in the available literature that need to be addressed in order to define the role of inhaled hypertonic saline therapy.
INDEX TERMS: bronchiolitis, hypertonic saline, infants, pediatrics, review
INTRODUCTION
Bronchiolitis, an infection of the lower respiratory tract, is the leading cause of infant and child hospitalization in the United States and is associated with increased costs overall. Therapeutic options are limited. Hypertonic saline inhalation therapy has been studied in clinical trials, and in 2014, the American Academy of Pediatrics (AAP) published updated guidelines on the diagnosis and management of bronchiolitis, which included new recommendations on the use of hypertonic saline.1 This article reviews the management of bronchiolitis, with a focus on the use of hypertonic saline.
DEFINITION AND PATHOPHYSIOLOGY
In its broadest definition, bronchiolitis is inflammation of the bronchioles. The AAP guidelines define bronchiolitis as a viral upper respiratory infection prodrome followed by respiratory effort and wheezing in children younger than 2 years of age.1
Within the first 2 years of life, more than one-third of children will develop bronchiolitis.2 Of these, 1 out of 10 children will be hospitalized. Approximately 100,000 bronchiolitis hospital admissions occur annually in the United States, leading to an estimated cost of $1.73 billion.1,2 Risk factors associated with increased infant mortality from bronchiolitis include prematurity and underlying cardiopulmonary disease or immunodeficiency.
Common viral causes of bronchiolitis include respiratory syncytial virus (RSV), parainfluenza virus, influenza, human metapneumovirus, and rhinovirus. Respiratory syncytial virus accounts for approximately 60% to 75% of bronchiolitis cases.1 Clinical signs and symptoms of bronchiolitis may include rhinitis, cough, wheezing, rales, tachypnea, nasal flaring, use of accessory muscles, and/or retractions.
Diagnosis of bronchiolitis is based on clinical signs and symptoms and a thorough history and physical exam.1 The recent expansion of polymerase chain reaction testing allows earlier confirmation of viral involvement. The AAP guidelines do not recommend the use of chest radiography as a result of its low yield and unnecessary exposure to radiation.1,2
Pathophysiology is important in order to understand the clinical manifestations and to manage this condition. Viral infection occurs through the upper respiratory tract and spreads to the lower tract within a few days; this results in acute inflammation and edema of the bronchiolar epithelium, necrosis of epithelial cells, and increased mucus production.3 Mucus plugs in the airway lead to partial or total obstruction of air flow. Impaired mucus clearance results from dehydration of airway surface liquid and increased sodium absorption. Obstruction can lead to atelectasis, which can further worsen breathing and respiratory function. Epidemiological studies4 have shown that bronchiolitis infection is associated with a high degree of morbidity but low mortality.
THERAPY AND MANAGEMENT
Although ribavirin has been used in the treatment of bronchiolitis, its effectiveness is limited in otherwise-healthy infants. All other therapeutic options are aimed at managing symptoms, but few of these options are specifically useful in the case of bronchiolitis. Pharmacologic options include oxygen (O2) therapy; beta2-adrenergic agonists, albuterol and levalbuterol; racemic epinephrine; corticosteroids; antibiotics; and, recently, hypertonic saline.
Oxygen therapy provides oxygen to the lungs and acts as a direct bronchodilator. Current AAP guidelines1 recommend the use of supplemental oxygen if oxygen saturations are less than 90% in order to avoid hypoxemia.
Short-acting beta2-agonists (albuterol and levalbuterol) dilate the bronchioles, improving oxygenation and breathing. The role of bronchodilators has been the subject of many meta-analyses and systematic reviews of the literature.5–10 These reviews showed that although bronchodilator use may improve clinical symptom scores, the effects are transient; they do not affect disease resolution, the need for hospitalization, or length of stay. Additionally, use of these medications is associated with adverse effects, including tachycardia and tremors. As a result, the 2014 AAP guidelines no longer recommend using albuterol and levalbuterol, even as a trial, in infants and children with bronchiolitis without a reactive airway component because the overall ineffectiveness outweighs any possible transient benefit.1 This is a departure from the previous AAP guidelines, which were published in 2006.1
Racemic epinephrine should be a useful therapeutic option as a result of its agonistic effects on alpha and beta receptors, helping to reduce edema and mucus plugging; however, its effects are transient, and studies as well as systematic reviews of the literature did not show a shortened length of hospital stay resulting from its use. As a result of possible improvement in patients with severe bronchiolitis, the 2014 AAP guidelines provided some support for racemic epinephrine as a rescue agent in the hospital setting.11–15
The use of corticosteroids in the treatment of bronchiolitis is controversial. A recent Cochrane Systematic Review16 showed that use of corticosteroids was not associated with significant reductions in clinical scores, hospitalization rates, or length of hospital stay, which is consistent with the AAP guidelines that do not recommend their use.1 The 2014 AAP guidelines also recommend against the use of antimicrobial agents unless there is a concomitant bacterial infection or a strong suspicion of one.1
Because of the paucity of therapeutic options available, recent literature has focused on novel therapies, such as hypertonic saline, for the management of bronchiolitis. Since the pathology of bronchiolitis involves airway inflammation and mucus plugging, improving mucus clearance should be beneficial in resolving bronchiolitis. Hypertonic saline shifts the flow of water into the mucus layer by osmosis, reducing submucosal edema, reducing viscosity of mucus, improving mucus clearance, and rehydrating the air surface liquid.17–20 The updated AAP guidelines support the use of hypertonic saline nebulization for infants and children hospitalized for bronchiolitis, except in the emergency department (ED) setting.1 This recommendation was made based on evidence from randomized controlled trials with inconsistent findings in the ED setting.
For this article, we have reviewed the current literature and the rationale behind the AAP recommendations for hypertonic saline in the management of bronchiolitis.
LITERATURE REVIEW
We performed a PubMed/Medline literature review using the following search terms: bronchiolitis and child and saline and hypertonic saline. We excluded languages other than English and indications for saline therapy other than bronchiolitis.
Tables 1 and 2 summarize the available literature on hypertonic saline for bronchiolitis in the outpatient/clinic/ED and hospitalized patients, respectively. The most commonly studied regimen was hypertonic saline 3% with a volume of 4 mL per dose, administered through a variety of nebulizers, in some trials with oxygen, while in others, home nebulization was described with no further details.
Table 1.
Summary of Clinical Trials for Hypertonic Saline in Ambulatory Setting (Outpatient/Clinic/Emergency Department) *
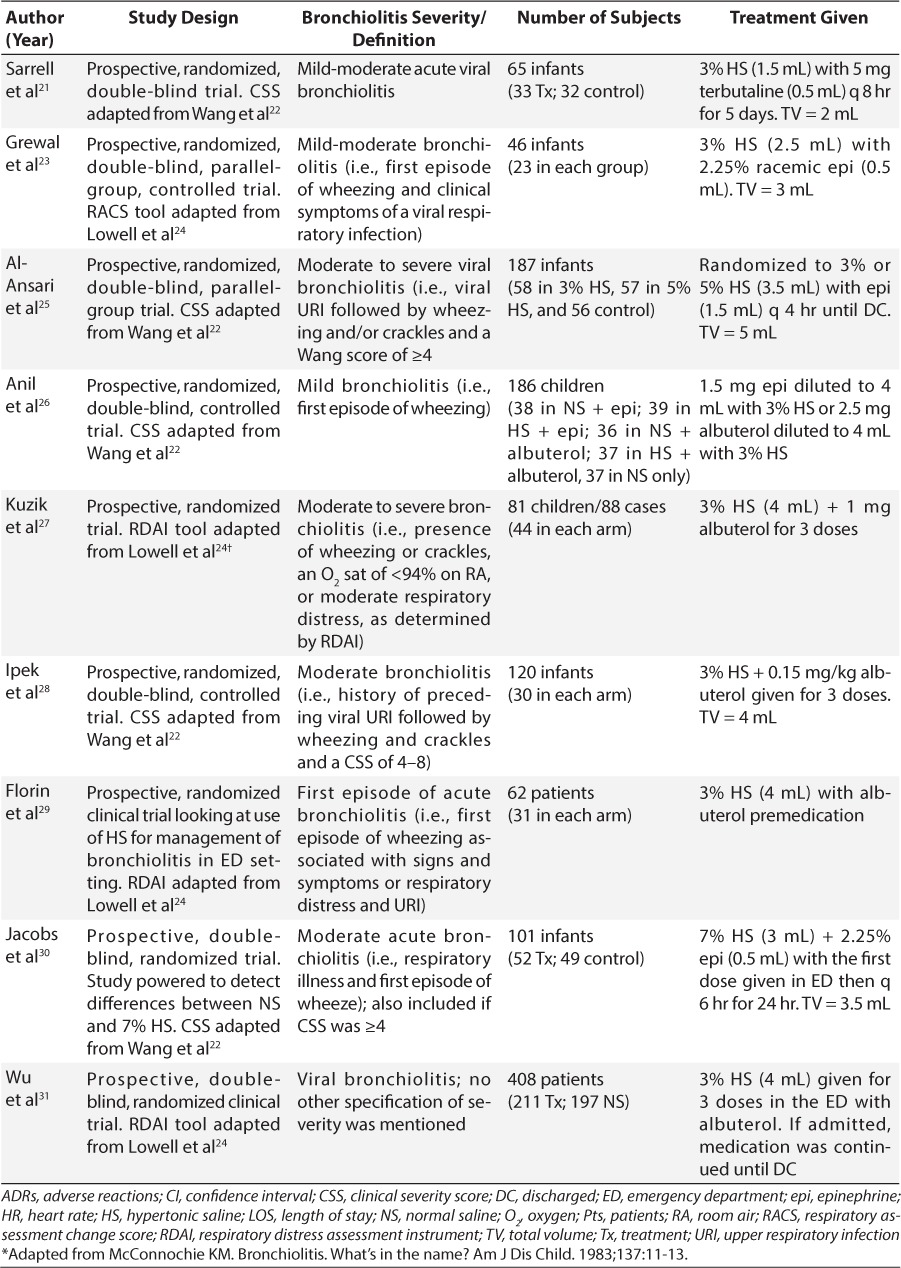
Table 2.
Summary of Clinical Trials for Hypertonic Saline in Hospitalized Patients *

Table 1.
Summary of Clinical Trials for Hypertonic Saline in Ambulatory Setting (Outpatient/Clinic/Emergency Department) *(cont.)
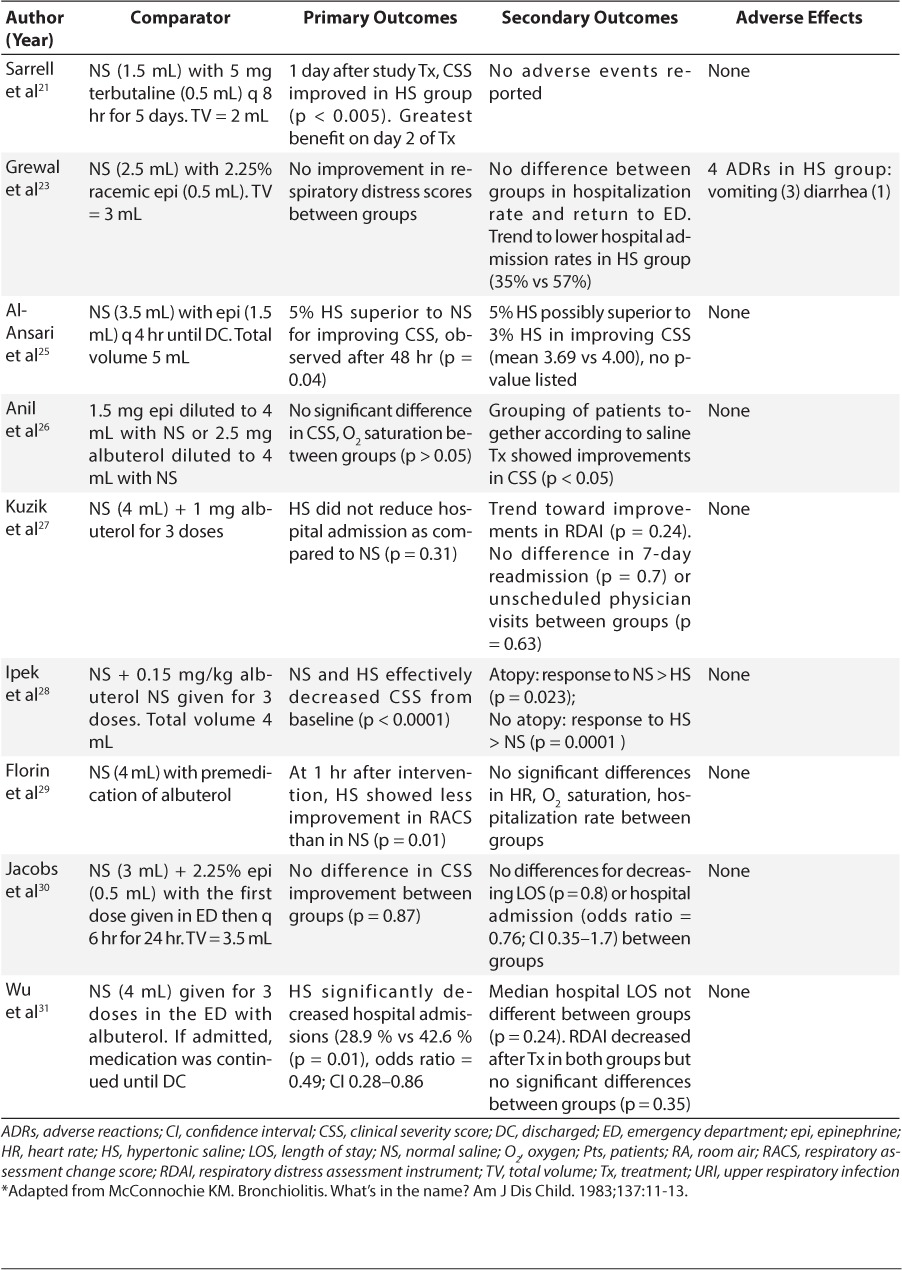
Table 2.
Summary of Clinical Trials for Hypertonic Saline in Hospitalized Patients *(cont.)

Table 2.
Summary of Clinical Trials for Hypertonic Saline in Hospitalized Patients *(cont.)

Clinical Trials Evaluating Hypertonic Saline Use in the Ambulatory Setting (Outpatient/Clinic/ED)
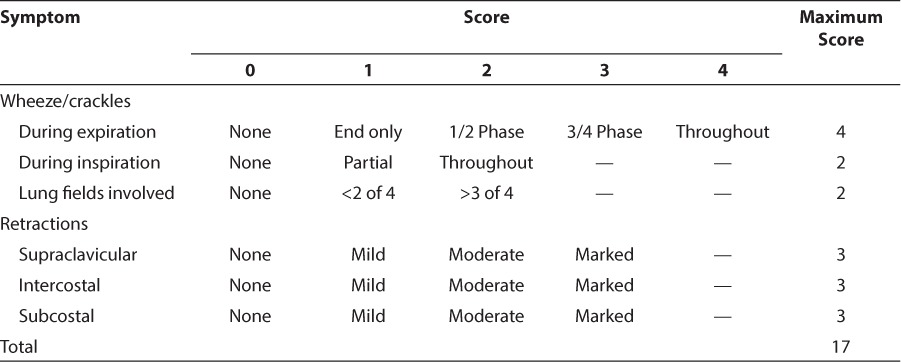
In 2002, Sarrell et al21 were the first to examine the role of terbutaline with hypertonic saline vs terbutaline with normal saline (NS) in a prospective, randomized, double-blind, controlled trial. Their primary goals were to determine whether hypertonic saline reduced clinical severity scores (CSS)22 (Table 3) and hospital admission rates in bronchiolitis. A secondary goal was to evaluate hypertonic saline safety. Children with mild to moderate viral bronchiolitis were included. Exclusion criteria included age of >24 months, chronic respiratory disease, cardiac disease, previous wheezing episode, oxygen saturation of <96% on room air (RA), and the need for hospitalization. Sarrell et al found that in non-asthmatic, non–severely ill ambulatory infants with viral bronchiolitis, use of 3% hypertonic saline in addition to terbutaline was safe and effective in decreasing symptoms, as compared to the use of NS with terbutaline. However, rates of hospitalization were too small to draw a conclusion for this outcome (3 in the control vs 2 in the treatment groups, respectively). Although this was the first article to examine the benefits of hypertonic saline, there are a few limitations associated with the study, including its applicability to mild bronchiolitis; a small sample size with no power analysis for the sample size; caregiver administration without confirmation of adherence; terbutaline use in both treatment and comparator groups, which might affect the interpretation of the true benefits of hypertonic saline; and, finally, the use of NS as a comparator, which may be effective alone.
Table 3.
Wang Clinical Severity Score22

In 2009, Grewal et al23 completed a single-center, randomized, double-blind, parallel-group, controlled trial that examined the use of nebulized 3% hypertonic saline with racemic epinephrine vs nebulized NS with racemic epinephrine for treatment of acute bronchiolitis in the ED. The primary outcome studied was a change in respiratory distress, using the Respiratory Assessment Change Score (RACS) from baseline to 120 minutes. The RACS is adapted from the Respiratory Distress Assessment Instrument (RDAI) (Table 4) and adds an evaluation of respiratory rate (RR).24 Secondary outcomes were the rates of hospital admission, return to the ED, and changes in oxygen saturation. Inclusion criteria included infants 6 weeks to 12 months of age, a clinical diagnosis of bronchiolitis (defined as first episode of wheezing and clinical symptoms of a viral respiratory infection), O2 saturations of ≥85% but ≤96% upon arrival to the ED, and an initial RDAI score of ≥4. Patients were excluded if they had preexisting cardiac or pulmonary disease, asthma, prior use of a bronchodilator, severe disease requiring resuscitation, or inability to use a nebulizer.
Table 4.
Respiratory Distress Assessment Instrument24
The authors found that at 120 minutes after nebulization, there was no improvement in RACS in the hypertonic saline group compared to the NS group. Hospital admission and return to ED were not different between the groups (no p-values reported), although a trend of lower hospital admission rates was seen in the hypertonic saline group (35% vs 57%). As determined a priori, the authors enrolled enough patients to show a reduction in RACS scores by at least 3. A greater number of children exposed to smoke in the hypertonic saline arm may have influenced the response in the study group, given that exposure to smoke exacerbates disease severity in bronchiolitis. Another limitation is that study medication was limited to 1 to 2 doses, whereas previous studies used repeated dosing.
In 2010, Al-Ansari et al25 compared the use of 5% hypertonic saline with epinephrine and 3% hypertonic saline with epinephrine. Their primary outcome was a reduction in mean CSS for each treatment group at 48 hours. Patients were included if they had an age of ≤18 months, a diagnosis of moderate to severe viral bronchiolitis, and a CSS of ≥4.22 Patients were excluded if they had a previous history of wheezing or apnea within 24 hours of presentation, were born at ≤34 weeks' gestation, used a steroid within 48 hours of presentation, had obtundation and progressive respiratory failure requiring intensive care unit (ICU) admission, had O2 saturation of ≤85% on RA at time of recruitment, or had a history of chronic lung disease, congenital heart disease, or immunodeficiency. Al-Ansari et al concluded that 5% hypertonic saline was effective and safe and may be superior to 3% hypertonic saline for early outpatient treatment of bronchiolitis; however, this study was not powered to show statistically significant differences between hypertonic saline groups.
In another 2010 study, Anil et al26 published a prospective, randomized, double-blind, controlled trial that compared albuterol, epinephrine, 3% hypertonic saline, and larger volume NS for patients with mild bronchiolitis. The primary outcome was a change in CSS. Other outcome measures included oxygen saturations and heart rate (HR) measured at 0, 30, and 120 minutes. Patients in the ED were included if they were between 6 weeks and 24 months of age, presented with a first episode of bronchiolitis, and had a CSS between 1 and 9, as adapted from Wang et al22 Exclusion criteria were allergic rhinitis, asthma, bronchopulmonary dysplasia, atopic dermatitis, prematurity, a history of cystic fibrosis, cardiac disease, renal disease, wheezing, O2 saturation of <85% on RA, CSS of >9, prior treatment with bronchodilators, steroid use within 2 weeks prior to study entry, loss of consciousness, and severe respiratory failure requiring mechanical ventilation. The study was powered to show differences in CSS between groups. The results did not show differences in CSS, O2 saturations, or HR between groups (p > 0.05) when evaluated as individual groups. When the authors grouped patients according to active medication, whether hypertonic saline or NS, all patients significantly improved their bronchiolitis score from baseline, starting 30 minutes after drug administration and persisting through 120 minutes postadministration. There were no adverse effects and no differences in readmission between groups. A strength of this study was separation of 5 parallel groups for comparison and grouping of all saline preparations together to compare against baseline.
Also in 2010, Kuzik et al27 conducted a prospective, randomized trial to determine the efficacy and safety of an intensive 3% hypertonic saline and albuterol vs NS and albuterol regimen in children with viral bronchiolitis. The primary outcome was hospital admission rate according to the attending physician. Secondary outcomes were RDAI score before and after treatment and need for subsequent intervention within 7 days after discharge. Children 24 months of age and younger who presented with moderate to severe viral bronchiolitis were eligible for inclusion. Patients were excluded if they had a history of Down syndrome; immunodeficiency; neurologic, metabolic, or cardiopulmonary disease; severe illness at presentation (defined as respiratory rate [RR] > 80, O2 saturations < 88% on RA, or need for assisted ventilation); prematurity (≤34 weeks gestation); or use of inhaled hypertonic saline 12 hours prior to admission. Admission rates were lower in the hypertonic saline group, though the difference was not significant. There was also a trend in greater improvement in reduction in RDAI scores (4.7 in hypertonic saline vs 3.7 in NS). There were no differences in the rate of readmissions after discharge between groups (7-day readmission or unscheduled physician visits) or in adverse reactions. The strengths of this study are the inclusion of moderately severe bronchiolitis and more intensive hypertonic saline treatment. This study found trends in improvements with hypertonic saline in bronchiolitis scores and hospitalization rates; however, according to their power analysis the authors did not enroll a sufficient number of patients to detect significant differences. In 2011, Ipek et al28 conducted a prospective, randomized, double-blind study to investigate the therapeutic benefit of nebulized 3% hypertonic saline for the treatment of bronchiolitis in the ED. The study investigated 4 different regimens: 1) albuterol 0.15 mg/kg plus NS; 2) albuterol 0.15 mg/kg plus 3% hypertonic saline; 3) 3% hypertonic saline alone; or 4) NS alone. The primary outcome was the change in CSS in each group after treatment, and the secondary outcome was the comparison of the improvement percentages of children with and without a history of atopy. Children 1 month to <2 years of age presenting with a clinical severity score22 of 4 to 8 were included. Exclusion criteria were a CSS outside of the range listed above, oxygen saturation of <85% on RA, chronic cardiac disease, premature birth, birth weight of <2500 g, history of recurrent wheezing episodes, immune deficiency, severe neurological disease, and chest radiograph findings of consolidation or atelectasis. The authors found that posttreatment mean CSS values were significantly lower than pretreatment scores in all groups (p = 0.0001), with no significant differences between groups. It was unclear when exactly these results were reported. Interestingly, infants with a history of atopy responded better to NS (p = 0.023), whereas those without a history of atopy responded better to hypertonic saline (p = 0.0001). Strengths of this study included the finding that either NS or hypertonic saline was effective in reducing CSS, the fact that multiple treatment groups were used to evaluate the efficacy of hypertonic saline alone and in combination with albuterol, and the fact that the study included a subgroup analysis of patients with a history of atopy. A limitation of this study is the absence of power analysis.
In 2014, Florin et al29 conducted a prospective, randomized clinical trial that evaluated the use of nebulized 3% hypertonic saline vs NS for bronchiolitis in the ED. The primary outcome was a change in respiratory distress 1 hour after the intervention, as measured by the RACS. Secondary outcomes included vital signs, oxygen saturation, hospitalization, perceptions of improvement from the ED physicians and parents, adverse events, and patient-related events 7 days after discharge from the ED. Children 2 to 23 months of age presenting to the ED with their first episode of bronchiolitis and having an RDAI24 score of 4 to 15 (moderate to severe) obtained after an albuterol treatment were included. Exclusion criteria included a history of asthma/wheezing, recent use of a bronchodilator, chronic lung or cardiovascular disease, critical illness, and inability to receive nebulized medication. At 1 hour after study medication administration, the hypertonic saline group had significantly less improvement in the median RACS compared with the NS group (hypertonic saline, −1 [interquartile range, −5 to 1] vs NS, −5 [interquartile range, −6 to −2]; p = 0.01]. The main difference between groups was a greater reduction in RRs in the NS group. There were no significant differences in secondary outcomes. The authors assessed patients 2 hours after study medication administration if they remained in the ED. The authors concluded that use of hypertonic saline, after standard treatment, in the ED showed less improvement than did use of NS. Based on these results, they recommended against a single dose of 3% hypertonic saline in the acute care setting, based on essentially one vital sign, RR, as a component of the RDAI score. Although not statistically different, the subjects with a high baseline severity score had improvements in both the hypertonic saline and NS groups. Additionally, differences in baseline characteristics between groups, use of a single dose of hypertonic saline, short assessment times (1 hour for most patients), and the use of an active control may have affected the outcomes of this study.
Jacobs et al30 were the first to evaluate the efficacy and safety of 7% hypertonic saline with racemic epinephrine vs 7% NS with racemic epinephrine in patients with acute bronchiolitis in the ED. Their primary hypothesis was that the use of hypertonic saline would improve the severity of bronchiolitis. Secondary outcomes included hospitalization rate, discharge rate at 23 hours, and length of hospital stay (LOS). Patients aged 6 weeks to ≤18 months with a first episode of wheeze who presented to the ED with bronchiolitis and a CSS score of ≥4 were included. Exclusion criteria included a prior history of wheezing, bronchodilator use within 2 hours of presentation, gestational age of ≤34 weeks, history of congenital heart disease or chronic pulmonary or chronic renal disease, oxygen saturation of 85% at the time of the study, and severe disease requiring ICU admission. Both study groups had a reduction in CSS, with no significant differences between groups for change in mean CSS. Length of stay in the ED was not significantly different between groups. The percentage of patients admitted was similar between groups. In this adequately powered study of patients with moderate to severe bronchiolitis, inhalation of both 7% hypertonic saline and NS plus epinephrine reduced CSSs. Limitations to this study were the use of a modified scoring measure that was internally, but not externally, validated; the use of epinephrine in both groups, which could confound the results; and the use of an active control, NS.
The most recent prospective, double-blind, randomized clinical trial31 to evaluate the use of albuterol plus either hypertonic saline or normal saline for bronchiolitis in the ED was conducted in a predominantly Hispanic population. Outcomes measures included hospital admission rate, LOS for admitted patients, and RDAI.24 Patients who were 24 months of age or younger with a primary diagnosis of viral bronchiolitis admitted from November through April were eligible for inclusion. Patients were excluded if they had a history of wheezing or bronchodilator use, had been born at <34 weeks' gestation, or had a history of cyanotic congenital heart disease, chronic lung disease, or tracheostomy.
The results of this study showed that hospital admission rates were significantly reduced for patients who received 3% hypertonic saline. To prevent one hospitalization, 8 patients would require treatment. The RDAI scores decreased after treatment in both groups, with no significant difference between them (p = 0.35). The authors did not disclose whether adverse effects were monitored. This is the first study that showed a reduction in hospital admission rates in the ED. The LOS, however, was not reduced. This may likely be due to a limited sample size for this outcome. To date, this is the largest clinical trial to evaluate the efficacy of hypertonic saline for treatment of bronchiolitis, especially in the ED setting.
Clinical Trials Evaluating Hypertonic Saline Use in Hospitals
Mandelberg et al32 conducted a prospective, randomized, double-blind, controlled trial that evaluated the effect of nebulized 3% hypertonic saline with 1.5 mg epinephrine vs nebulized NS with 1.5 mg epinephrine in hospitalized infants with viral bronchiolitis. They assessed CSS22 and LOS. Infants were included if they presented with clinical symptoms of viral bronchiolitis along with a temperature of >38°C. Infants were excluded if they had previous wheezing episodes, cardiac disease, chronic respiratory disease, were aged >12 months, had an O2 saturation of <85% on RA, obtunded consciousness, and/or advanced respiratory failure requiring mechanical ventilation. The authors reported a significant improvement in CSS in favor of hypertonic saline compared to the NS group; however, p-values were not provided. Length of stay was significantly shorter in the hypertonic saline group (3 ± 1.2 days) compared to the NS group (4 ± 1.9 days); this represented a 25% reduction in hospital LOS. Although this study was not powered, it showed a reduction in the LOS and bronchiolitis scores. In addition, the authors used an active placebo, epinephrine.
In a 2006, Tal et al33 conducted a prospective, randomized, double-blind, controlled trial study that expanded on the data reported by Mandelberg et al.32 They compared the efficacy of 1.5 mg epinephrine in 4 mL of NS vs epinephrine 1.5 mg in 4 mL of 3% hypertonic saline in patients with bronchiolitis.33 The authors conducted a follow-up study and a pooled analysis of 2 years' worth of experience to demonstrate the effectiveness of nebulized 3% hypertonic saline in hospitalized infants with viral bronchiolitis. The study assessed duration of hospitalization and change in clinical score after nebulization treatment. Inclusion and exclusion criteria were the same as the original study.32 For this study, patients in the hypertonic saline group had significant improvements in CSS over the NS group on hospitalization days 1 and 2. Length of stay, determined by an attending physician who was blinded to study groups, was significantly shorter in the hypertonic saline group than in the NS group. Improvements in CSS in the first 2 days of hospitalizations favored hypertonic saline treatment. This study confirmed the positive effects of hypertonic saline treatment, and the pooled analysis further supports the efficacy of 3% hypertonic saline in infants hospitalized with bronchiolitis. Given that both studies showed improvements with hypertonic saline, it is difficult to discern the impact of the delivery method on the result. Other limitations were the lack of data reporting after the first 2 days of hospitalization and reporting of adverse effects to ensure hypertonic saline safety.
Luo et al34 evaluated the efficacy and safety of 2.5 mg albuterol nebulized in either 3% hypertonic saline or NS in hospitalized children in China with mild to moderate bronchiolitis. This prospective, double-blind, randomized, controlled trial assessed LOS, CSS, and clinical symptoms (cough, wheezing, and pulmonary physical signs). Children were included if they were diagnosed for the first time with bronchiolitis and had mild to moderate presentation according to the CSS (5 to 8.9).22 Children were excluded if they were older than 24 months of age and had cardiac or pulmonary disease, respiratory failure requiring mechanical ventilation, immunodeficiency, prematurity (<34 weeks' gestation), and use of 3% hypertonic saline and/or albuterol 12 hours before enrollment. The authors found that crackles disappeared more quickly following 3% hypertonic saline plus 2.5 mg albuterol. For the first 3 days of treatment, CSS scores were lower in those given hypertonic saline, but there were no significant differences after this time. Mean LOS was significantly shorter as well, and there were no adverse events.
While this study showed improvements in bronchiolitis symptoms and LOS, the authors acknowledged that LOS was longer in their study as compared to others and that the study was not powered to show statistical significance. One important consideration is the different definition used for determining LOS. This study discharged patients when they had no respiratory signs/symptoms for 12 hours, while other studies used a discharge criteria of CSS < 4 and O2 saturation of at least 95% on RA for 4 hours. This may have led to the longer LOS in this study.
In a follow-up study, Luo et al35 conducted a prospective, randomized, controlled trial to determine the efficacy and safety of 4 mL of inhaled nebulized hypertonic saline vs 4 mL of inhaled nebulized NS in hospitalized infants with moderate to severe bronchiolitis. The authors compared signs and symptoms, CSS, and LOS of infants in the hypertonic saline group with those of the NS group. Patients were included if they were <24 months of age and presented with the first episode of wheezing. Patients were excluded for the following reasons: age greater than 24 months; prior episode of wheezing, chronic cardiac and pulmonary illness, immunodeficiency, or respiratory failure requiring mechanical ventilation; use of nebulized 3% hypertonic saline 12 hours before study entry; and prematurity (<34 weeks' gestation). Evaluation of signs and symptoms showed that wheezing and cough remission time were significantly shorter in the hypertonic saline group. A hoarse voice was reported equally between groups and resolved after 3 to 4 days.
As a result of this study Luo et al concluded that frequent inhalation of hypertonic saline is not only safe but also significantly reduces LOS. In addition, the authors concluded that hypertonic saline relieves signs and symptoms faster than does NS in patients with moderate to severe bronchiolitis. This is the first study that avoided the use of bronchodilators as a confounding variable and still demonstrated improvements in the hypertonic saline group. The limitations of this study include the fact that multiple outcomes were sought without power analysis.
Miraglia Del Giudice et al36 conducted a prospective, double-blind, randomized, controlled trial to assess the effects of nebulized epinephrine plus either 3% hypertonic saline or NS in hospitalized children with bronchiolitis in Italy. They assessed 2 main outcomes: 1) the difference in LOS between the 2 groups and 2) the change in CSS from baseline between the 2 groups. Children who were <2 years of age with a clinical diagnosis of bronchiolitis were included. Bronchiolitis was defined as first episode of wheezing and symptoms of a viral respiratory infection, significant respiratory distress measured using CSS,22 and O2 saturation of <94% without supplementation. Exclusion criteria were prematurity (<36 weeks' gestational age), preexisting cardiac or pulmonary disease, history of asthma, an initial O2 saturation of ≤85%, or severe respiratory distress requiring resuscitation. The authors determined that use of 3% hypertonic saline is more effective than NS in hospitalized children with bronchiolitis, resulting in improvements in CSS and LOS; however, the study was not powered to detect significant differences. It is important to note that nebulized medications were given every 6 hours, whereas other studies used every-8-hour administration, which could have affected the study outcomes. The lack of a difference in CSS on day 1 in the hypertonic saline group is not surprising given a lag time in improvements.
In 2013, Sharma et al37 conducted a randomized, controlled, double-blind trial to evaluate the efficacy of nebulized 2.5 mg of albuterol plus either 3% hypertonic saline or NS in children with bronchiolitis in India. The primary outcome was LOS, which was defined as time for CSS22 to reach <3. Patients were included if they were 1 to 24 months old and had been hospitalized with acute bronchiolitis of moderate severity, as defined by Wang et al.22 Bronchiolitis was defined as first episode of wheezing along with upper respiratory infection (i.e., rhinorrhea, cough, sometimes low-grade fever, and possible progression to dyspnea). Patients were excluded if they had received hypertonic saline within 12 hours of admission or had diminished consciousness, pulmonary or cardiac disease, previous wheezing, or severe respiratory distress. They reported that hypertonic saline was not superior to NS for the treatment of acute bronchiolitis and that there was no difference in mean LOS between the 2 groups. This study did not include a placebo group, which would have provided better data with which to assess the role of saline, in general, in bronchiolitis.
Recent years have seen an upsurge in interest in the use of hypertonic saline, with a corresponding uptick in the number of studies. A 2014 study38 examined a new, promising therapy. Bueno Campaña et al38 conducted a randomized, controlled trial to determine whether heated humidified high-flow nasal cannula (HHFNC) is superior to inhaled hypertonic saline for management of moderate bronchiolitis. HHHFNC involves providing warmed and humidified gas at high flow to improve breathing and patient comfort. To date, there are no studies demonstrating its use in the treatment of bronchiolitis; therefore, this study's primary outcome was to assess the change in mean RACS in 6 defined consecutive time periods, as described by Lowell et al.24 Secondary outcomes were comfort scores during the defined time periods, LOS, and rates of admission to the pediatric intensive care unit (PICU). Infants ≤ 6 months presenting with a first episode of mild bronchiolitis (RDAI score ≥ 4) who were admitted to the hospital were eligible for inclusion. Exclusion criteria were prematurity (gestational age of <37 weeks), chronic lung disease, congenital heart disease, cystic fibrosis, neuromuscular disease, immunodeficiency, the need for immediate intubation and ventilation, and airway anomalies. If not received previously, patients were given 0.5 mL/kg (maximum, 3 mL) of nebulized epinephrine, 1/1000, with 2 mL of NS one time only. Patients were then randomized to receive nebulized epinephrine 1/1000 plus 2 mL of NS, nebulized epinephrine 1/1000 with 2 mL of 3% hypertonic saline, or HHHFNC. HH-HFNC was given at flow rates of between 6 and 8 L/min. Bueno Campaña et al38 concluded that HHHFNC is no more effective than 3% hypertonic saline. Limitations of the study include the use of epinephrine prior to randomization, which could affect outcome, and a non-blinded study design, which could introduce bias.
In a 2014 Australian study, Everard et al39 conducted a multicenter, randomized, open control trial to evaluate the effect of the use of 3% hypertonic saline on time to hospital discharge in infants with acute bronchiolitis that required O2 supplementation. The primary outcome was the time until the infant was assessed as being “fit for discharge,” which was defined as the point at which an infant was feeding ≥ 75% of usual intake and having O2 saturation of ≥92% for 6 hours. Secondary outcomes included actual time to discharge, readmission within 28 days, and occurrence of adverse events. Infants admitted for acute bronchiolitis who required supplementary oxygen for an O2 saturation of <92% were included. The results of the study showed no difference between the treatment arms in terms of hospital discharge: “fit for discharge” or time to actual discharge. There were also no differences in the numbers of admissions to ICU or number of readmissions within 28 days of randomization. Children who tested positive for RSV had a longer time until fitness to discharge. While the authors did not find an association between treatment effect and viral status, 27% of children were never tested. It is unknown whether these data might have affected the results, since this analysis was underpowered because of lack of these data. Six adverse events were reported in the hypertonic saline arm. One serious adverse event was bradycardia with desaturation during medication administration, which resolved the following day. The 5 remaining events were bradycardia (self-correcting), desaturation, increased RR, coughing fit, and chest infection. All adverse events resolved within 6 days and were self-limiting. The authors concluded that the addition of 3% hypertonic saline has no beneficial or harmful consequences when compared with standard supportive care. The strengths of this study included a multicenter design, the use of a non-active control as a comparator, a more strict definition of bronchiolitis, and specific definitions for time to discharge; however, the lack of blinding may have introduced an element of bias. Additionally, authors did not evaluate clinical improvement, yet they commented on the lack of any clinically relevant outcome with hypertonic saline.
Also in 2014, Flores-Gonzalez et al40 conducted a prospective, randomized, double-blind, parallel-group study aimed at evaluating the efficacy of 7 mL of 3% hypertonic saline with 3 mL of epinephrine or 7 mL of 3% hypertonic saline and 3 mL of sterile water for the treatment of hospitalized infants and children with acute moderate bronchiolitis. The primary outcome was LOS. Secondary outcomes included Wood-Downes41 scores (rhonchi, retractions, RR, HR, air flow, and cyanosis; defined as mild [1–3 points], moderate [4–7 points]], or severe [8–14 points] exacerbation), vital signs, adverse events, need for admission to the PICU, and mechanical ventilation. Patients were included if they were <24 months old and presented for hospital admission for moderate bronchiolitis along with first episode of respiratory distress with wheezing following an upper respiratory tract infection. Exclusion criteria included a history of prematurity (corrected age of <6 weeks), chronic lung disease, heart disease, immunodeficiency, prior history of wheezing or asthma, previous treatment with mechanical ventilation at home, or a history of bronchiolitis requiring PICU admission. For the primary outcome, LOS, there were no significant differences found between groups for median LOS. Additionally, no significant differences were found between groups for CSS, oxygen saturation, RR, or HR. On the third day of hospitalization, disease severity and respiratory rate in the hypertonic saline with epinephrine group presented a non-significant trend toward earlier improvement. The authors concluded that use of nebulized epinephrine with hypertonic saline is safe and that there is a trend toward earlier clinical recovery. Limitations of this study include the use of sterile water, which is an irritant to the respiratory tract, as a placebo; lack of power due to limited enrollment; and the employment of a CSS that has been used in asthma, not bronchiolitis.
In another 2014 study, Nenna et al42 conducted a prospective, randomized, double-blind, controlled study to evaluate the efficacy of 2.5 mL of 7% hypertonic saline with 0.1% hyaluronic acid vs 2.5 mL of NS in infants <7 months of age who were hospitalized with mild to moderate bronchiolitis. Primary outcome was hospital LOS, while secondary outcomes included safety and reduction in the bronchiolitis severity score. Hyaluronic acid was used to prevent adverse effects, such as cough, that may be associated with hypertonic saline inhalation, a strategy previously used in patients with cystic fibrosis.43,44 Infants diagnosed with bronchiolitis with a CSS of ≥4, as adapted from Midulla et al,45 were enrolled. Patients with a previous episode of lower respiratory tract infection or wheezing, chronic cardiac or pulmonary diseases, immunodeficiency, and premature birth (<34 weeks' gestation) were excluded. The authors observed that hypertonic saline with hyaluronic acid reduced mean LOS by 0.7 days; however, the results were not statistically significant. Clinical scores were not different between groups during the first 3 days of hospitalization. More patients coughed in association with 7% hypertonic saline and hyaluronic acid than with NS (4 and 2 patients, respectively). This is the first study to use young infants exclusively, a patient population most vulnerable to bronchiolitis. Limitations of this study included use of a lower volume, which may not have been sufficient to distribute to all lung fields; the addition of hyaluronic acid, which may have influenced the outcome of the study; a small sample size that did not completely meet power analysis; and use of a different CSS compared to other studies, with no information on the reliability or clinical validity of the CSS used.
In a 2014 study of children in Nepal, Ojha et al46 conducted a randomized, controlled, double-blind trial to compare 3% hypertonic saline vs NS for the inpatient management of bronchiolitis. The primary outcome was LOS. Bronchiolitis was defined as the first episode of wheezing associated with tachypnea and increased respiratory effort with an upper respiratory infection. Children who were >6 weeks to <24 months of age with a clinical presentation of bronchiolitis for the first time were included in the study. Children were excluded if they had previous episodes of wheezing, cardiac or pulmonary disease, immunodeficiency, respiratory failure requiring mechanical ventilation, use of 3% hypertonic saline and albuterol 12 hours before enrollment, prematurity (<34 weeks' gestation), and O2 saturation of <85% on RA. This study showed that 3% hypertonic saline was not superior to NS in terms of improving bronchiolitis severity score and improving LOS. Limitations included a limited sample size and the inclusion of an active comparator.
Also in 2014, Teunissen et al47 conducted a prospective, multicenter, double-blind, randomized, controlled trial to evaluate a concentration-dependent effect of 3% vs 6% hypertonic saline vs NS, both with albuterol, in viral bronchiolitis. The primary study outcome was hospital LOS, which was defined as the time from drug administration to the clinician's decision to discharge the patient. Secondary outcomes included the need for and duration of supplemental oxygen or tube feeding. Hospitalized children aged 0 to 24 months diagnosed with moderate to severe bronchiolitis were eligible for the study if they had a Wang CSS of ≥3 at presentation.22 To exclude patients with atopic wheeze, children who improved their scores by a minimum of 2 points following the inhalation of albuterol 2.5 mg were not enrolled. Additional exclusion criteria included hemodynamically significant congenital heart disease, chronic preexisting lung disease, immunodeficiency, treatment with corticosteroids, previous wheezing, and food allergy or eczema. The authors found that median hospital LOS and need for supplemental oxygen or tube feeding did not differ significantly among groups. Adverse effects were similar between groups, except that cough was reported more commonly in the hypertonic saline groups. In this adequately powered study, hypertonic saline at 2 different concentrations was not different from NS in hospitalized children with moderate to severe bronchiolitis and was associated with cough. Limitations of this study included the use of an active control and lack of evaluation of bronchiolitis severity scores to assess the clinical benefits of hypertonic saline. This study's results are difficult to compare to those from other trials because of the authors' variation in terms of the calculation of the LOS.
In the most recent retrospective study of hypertonic saline, Florin et al48 examined patterns of use of 3% hypertonic saline and LOS in children in a multicenter, retrospective, observational cohort study in hospitalized infants across the United States. The authors collected data from children from 42 hospitals associated with the Pediatric Health Information System over a 3-year period. Patients were eligible for inclusion in the study if they were ≤12 months of age with a diagnosis of bronchiolitis. Children with cystic fibrosis, spinal muscular atrophy, or bronchiectasis were excluded. Based on the database used, the authors could not quantify how often hypertonic saline was administered in a single day; therefore, use of hypertonic saline was categorized into 4 use patterns: trial, rescue, daily, and sporadic. Trial use was defined as use for a single day on day 0 or day 1 of hospitalization, with no additional use for the remainder of the hospitalization. Rescue use was defined as use of hypertonic saline on the third day of hospitalization or beyond. Daily use was defined as use of hypertonic saline within the first 2 days of hospitalization and repeated use throughout hospital admission. Sporadic use was defined as hypertonic saline use in a random pattern that did not meet the other 3 categories. There were 63,337 hospitalizations for bronchiolitis during the study period. Hypertonic saline was used for bronchiolitis in 24 out of the 42 hospitals (57%), for 2.9% of hospitalizations. There was a large variation of use across the 24 hospitals. Of the hospitals that used hypertonic saline, 1115 (60%) reported daily use, 207 (11.3%) reported trial use, 326 (17.7%) reported rescue use, and 191 (10.4%) reported sporadic use. For the outcome of LOS, the authors used a propensity score-matched analysis to account for potential confounders. When comparing daily hypertonic saline recipients vs non-recipients, there was no difference in mean LOS. Those who used hypertonic saline daily had a 33% decreased likelihood of staying in the hospital more than 4 days compared to non-recipients. The authors concluded that use of hypertonic saline may be of benefit in those patients sick enough to remain in the hospital for more than 4 days. Limitations included a retrospective observational design, lack of precision for dosage administered and patient monitoring for symptomatic improvement, and the non-accuracy of the LOS as a measurement of drug efficacy due to the various confounders of this measure.
DISCUSSION/CONCLUSION
This article critically reviewed the literature on the efficacy, safety, and expectations of hypertonic saline in bronchiolitis in the outpatient, ED, and inpatient settings. A total number of 2682 children were included in the 22 trials reviewed (Tables 1 and 2). Numerous concentrations of saline were employed in these trials, ranging from 3% to 7%, with volumes ranging from 2 mL to 7 mL per dose. Frequency of dosing ranged from 2 to 3 single doses; however, it was more common to administer doses every 4 or 8 hours, often until the patient was discharged from the institution. Time to achieve efficacy was detected in as little as 20 minutes and for up to 72 hours after administration of hypertonic saline. Delayed efficacy was likely due to edema, inflammation, and mucus plugs of the bronchiolar epithelium in bronchiolitis, which may require exposure to multiple doses of saline over a longer period of time. The studies had various limitations; the most common was that, with the exception of 4 trials,34,35,42,46 a bronchodilator or vasoconstrictor/bronchodilator, and in one instance HA, were used in both arms of the studies, the active and control groups.
Hypertonic saline was shown to be more effective than NS in improving bronchiolitis clinical scores in 5 studies21,25,32,33,36 in both outpatient and inpatient settings, consistent with the results of Zhang et al.49
In the ED setting, both saline preparations, hypertonic or normal, were effective in reducing bronchiolitis scores.26,28,30,31 The determination by the AAP that hypertonic saline is not effective in this setting is intriguing in light of the effectiveness of both forms of saline (NS and hypertonic saline) in these trials.
Five studies32–36 noted that LOS for patients who received hypertonic saline was shorter than for those given NS, which is consistent with the results from Zhang et al,49 who reported a reduction in LOS by −1.15 days (95% confidence interval, −1.49 to −0.82), a 22.7% reduction. In 7 additional trials not included in the review by Zhang et al49 there was no difference between saline preparations in terms of LOS.31,40,42,47 This was also reported by Florin et al48 in their 2015 publication. This may reflect a benefit from any saline intervention, whether hypertonic or NS, since no comparison was made to patients who were not placed on a saline preparation. A comparison to patients who were not enrolled in these studies, carried out during the same bronchiolitis season, may be helpful in delineating the role of any saline preparation in the management of bronchiolitis for this outcome measure. In addition, LOS is a difficult outcome to correlate with the efficacy of an intervention as a result of its dependence on many factors according to institutional or caregiver situations. In one study47 in which the determination for patient discharge from the institution was calculated, rather than the length of time patients spent in the hospital, there was no difference in LOS. It would be helpful to study LOS using this method in more trials. The AAP guidelines1 stipulate that a LOS that is expected to last for 72 hours or longer may justify the use of hypertonic saline, a determination that may be clinically challenging to make.
Zhang et al49 described a non-significant reduction in hospitalization rates for hypertonic saline; however, this was not a primary outcome in any of the 4 studies they analyzed, and hence these studies were not powered to show a significant difference. Since Zhang's systematic review, 2 additional trials in the ED, with admission rates as a primary outcome, have been published.27,31 A larger study by Wu et al31 supported a reduction in hospital admissions of about 50%. Although this reached statistical significance, the number of patients enrolled did not meet the power criteria. More trials with the primary outcome of reducing hospital admissions are needed to determine the role of hypertonic saline.
Two studies25,47 evaluated different concentrations of hypertonic saline at the same time: 5% and 6%. Teunissen et al47 did not find a difference between 3% and 6% hypertonic saline in a study that was adequately powered. The question of the superiority of higher concentrations of hypertonic saline remains unanswered.
It is important to note common limitations among all published trials. These limitations include enrollment of patients who were not severely ill and in different settings (non-ICU, non–severely ill, patients with asthma, ED, ICU); inconsistencies in dosage, frequency of dosing, and concentration of hypertonic saline used; inconsistency in type of delivery device employed; and the use of different CSS criteria (Tables 3 and 4). In addition, albuterol, terbutaline, or racemic epinephrine were instituted equally between groups in most studies to minimize wheezing from the saline preparations. We were unable to identify any differences in outcomes according to the bronchodilator used across these trials.
The use of an active comparator, such as NS, deserves further comment. As a result of the theorized mechanism of action of hypertonic saline in improving airway inflammation, reducing mucus plugging, and improving mucus clearance, NS itself can be beneficial in managing bronchiolitis. Therefore, use of an active comparator such as NS, which was used in most trials, makes it difficult to discern the benefits of hypertonic saline alone. Designing a trial that employs a non-irritating inhaled placebo would be ideal and should allow one to distinguish between the roles of hypertonic saline and NS. However, the findings that NS was as effective as hypertonic saline in many trials begs the question: Does the concentration of saline for nebulization really matter?
From the trials reviewed in this article, the review by Zhang et al,49 and the AAP guidelines,1 hypertonic saline has been very well tolerated. The concomitant administration of a bronchodilator may not be necessary to reduce feared adverse effects.1
In conclusion, we agree with the AAP guidelines1 regarding the use of nebulized hypertonic saline to reduce bronchiolitis scores and LOS for infants with bronchiolitis who are expected to be hospitalized for more than 72 hours. We also note that recent trials21–31 suggest that hypertonic saline reduces admission rates from the ED, and we believe there may be a role for hypertonic saline in this setting. Given the safety of this therapy and the lack of other effective therapies for these patients, use of hypertonic saline should be attempted in multiple doses in all patient care settings where nebulization can be administered. Large, well-powered trials that use a consistent dosage and concentration of hypertonic saline, or perhaps NS, are needed to delineate the role of saline therapy in children with bronchiolitis using strictly defined outcomes, such as the determination of discharge from the institution rather than LOS, and there is a need for more trials in the ED, with the aim of confirming whether hypertonic saline therapy reduces hospitalization.
Acknowledgment
At the time of publication Dr Baron was a PGY1 resident at Winthrop University Hospital, Mineola, New York.
Abbreviations:
- AAP
American Academy of Pediatrics
- CSS
clinical severity score
- ED
emergency department
- HHHFNC
heated, humidified high-flow nasal cannula
- HR
heart rate
- ICU
intensive care unit
- ITT
intent-to-treat
- LOS
length of stay
- NS
normal saline
- O2
oxygen
- PICU
pediatric intensive care unit
- RA
room air
- RACS
respiratory assessment change score
- RDAI
respiratory distress assessment instrument
- RR
respiratory rate
- RSV
respiratory syncytial virus
Footnotes
FiO2, fraction of inspired oxygen; O2, oxygen; RA, room air; RR, respiratory rate
Disclosures The authors declare no conflicts or financial interests in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, gifts, or honoraria.
REFERENCES
- 1.Ralston SL, Lieberthal AS, Meissner HC et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):e1474–e1502. doi: 10.1542/peds.2014-2742. [DOI] [PubMed] [Google Scholar]
- 2.Hasegawa K, Tsugawa Y, Brown DF et al. Trends in bronchiolitis hospitalizations in the United States, 2000–2009. Pediatrics. 2013;132(1):28–36. doi: 10.1542/peds.2012-3877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Piedimonte G, Perez MK. Respiratory syncytial virus infection and bronchiolitis. Pediatr Rev. 2014;35(12):519–530. doi: 10.1542/pir.35-12-519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Holman RC, Shay DK, Curns AT et al. Risk factors for bronchiolitis-associated deaths among infants in the United States. Pediatr Infect Dis J. 2003;22(6):483–490. doi: 10.1097/01.inf.0000069765.43405.3b. [DOI] [PubMed] [Google Scholar]
- 5.Chavasse R, Seddon P, Bara A, McKean M. Short acting beta agonists for recurrent wheeze in children under 2 years of age. Cochrane Database Syst Rev. 2002;3:CD002873. doi: 10.1002/14651858.CD002873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Flores G, Horwitz RI. Efficacy of beta2-agonists in bronchiolitis: a reappraisal and meta-analysis. Pediatrics. 1997;100(2 Pt 1):233–239. doi: 10.1542/peds.100.2.233. [DOI] [PubMed] [Google Scholar]
- 7.Gadomski AM, Scribani MB. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev. 2014;6:CD001266. doi: 10.1002/14651858.CD001266.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kellner JD, Ohlsson A, Gadomski AM, Wang EE. Efficacy of bronchodilator therapy in bronchiolitis. A meta-analysis. Arch Pediatr Adolesc Med. 1996;150(11):1166–1172. doi: 10.1001/archpedi.1996.02170360056009. [DOI] [PubMed] [Google Scholar]
- 9.King VJ, Viswanathan M, Bordley WC et al. Pharmacologic treatment of bronchiolitis in infants and children: a systematic review. Arch Pediatr Adolesc Med. 2004;158(2):127–137. doi: 10.1001/archpedi.158.2.127. [DOI] [PubMed] [Google Scholar]
- 10.Wainwright C. Acute viral bronchiolitis in children—a very common condition with few therapeutic options. Paediatr Respir Rev. 2010;11(1):39–45. doi: 10.1016/j.prrv.2009.10.001. quiz 45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hartling L, Fernandes RM, Bialy L et al. Steroids and bronchodilators for acute bronchiolitis in the first two years of life: systematic review and meta-analysis. BMJ. 2011;342:d1714. doi: 10.1136/bmj.d1714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hartling L, Wiebe N, Russell K et al. A meta-analysis of randomized controlled trials evaluating the efficacy of epinephrine for the treatment of acute viral bronchiolitis. Arch Pediatr Adolesc Med. 2003;157(10):957–964. doi: 10.1001/archpedi.157.10.957. [DOI] [PubMed] [Google Scholar]
- 13.Patel H, Gouin S, Platt RW. Randomized, double-blind, placebo-controlled trial of oral albuterol in infants with mild-to-moderate acute viral bronchiolitis. J Pediatr. 2003;142(5):509–514. doi: 10.1067/mpd.2003.196. [DOI] [PubMed] [Google Scholar]
- 14.Skjerven HO, Hunderi JO, Brugmann-Pieper SK et al. Racemic adrenaline and inhalation strategies in acute bronchiolitis. N Engl J Med. 2013;368(24):2286–2293. doi: 10.1056/NEJMoa1301839. [DOI] [PubMed] [Google Scholar]
- 15.Wainwright C, Altamirano L, Cheney M et al. A multicenter, randomized, double-blind, controlled trial of nebulized epinephrine in infants with acute bronchiolitis. N Engl J Med. 2003;349(1):27–35. doi: 10.1056/NEJMoa022226. [DOI] [PubMed] [Google Scholar]
- 16.Fernandes RM, Bialy LM, Vandermeer B et al. Glucocorticoids for acute viral bronchiolitis in infants and young children. Cochrane Database Syst Rev. 2013;6:CD004878. doi: 10.1002/14651858.CD004878.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Daviskas E, Anderson SD, Gonda I et al. Inhalation of hypertonic saline aerosol enhances mucociliary clearance in asthmatic and healthy subjects. Eur Respir J. 1996;9(4):725–732. doi: 10.1183/09031936.96.09040725. [DOI] [PubMed] [Google Scholar]
- 18.Mandelberg A, Amirav I. Hypertonic saline or high volume normal saline for viral bronchiolitis: mechanisms and rationale. Pediatr Pulmonol. 2010;45(1):36–40. doi: 10.1002/ppul.21185. [DOI] [PubMed] [Google Scholar]
- 19.Sood N, Bennett WD, Zeman K et al. Increasing concentration of inhaled saline with or without amiloride: effect on mucociliary clearance in normal subjects. Am J Respir Crit Care Med. 2003;167(2):158–163. doi: 10.1164/rccm.200204-293OC. [DOI] [PubMed] [Google Scholar]
- 20.Wark P, McDonald VM. Nebulised hypertonic saline for cystic fibrosis. Cochrane Database Syst Rev. 2009;2:CD001506. doi: 10.1002/14651858.CD001506.pub3. [DOI] [PubMed] [Google Scholar]
- 21.Sarrell EM, Tal G, Witzling M et al. Nebulized 3% hypertonic saline solution treatment in ambulatory children with viral bronchiolitis decreases symptoms. Chest. 2002;122(6):2015–2020. doi: 10.1378/chest.122.6.2015. [DOI] [PubMed] [Google Scholar]
- 22.Wang EE, Milner RA, Navas L, Maj H. Observer agreement for respiratory signs and oximetry in infants hospitalized with lower respiratory infections. Am Rev Respir Dis. 1992;145(1):106–109. doi: 10.1164/ajrccm/145.1.106. [DOI] [PubMed] [Google Scholar]
- 23.Grewal S, Ali S, McConnell DW et al. A randomized trial of nebulized 3% hypertonic saline with epinephrine in the treatment of acute bronchiolitis in the emergency department. Arch Pediatr Adolesc Med. 2009;163(11):1007–1012. doi: 10.1001/archpediatrics.2009.196. [DOI] [PubMed] [Google Scholar]
- 24.Lowell DI, Lister G, Von Koss H, McCarthy P. Wheezing in infants: the response to epinephrine. Pediatrics. 1987;79(6):939–945. [PubMed] [Google Scholar]
- 25.Al-Ansari K, Sakran M, Davidson BL et al. Nebulized 5% or 3% hypertonic or 0.9% saline for treating acute bronchiolitis in infants. J Pediatr. 2010;157(4):630–634. e634. doi: 10.1016/j.jpeds.2010.04.074. [DOI] [PubMed] [Google Scholar]
- 26.Anil AB, Anil M, Saglam AB et al. High volume normal saline alone is as effective as nebulized salbutamol-normal saline, epinephrine-normal saline, and 3% saline in mild bronchiolitis. Pediatr Pulmonol. 2010;45(1):41–47. doi: 10.1002/ppul.21108. [DOI] [PubMed] [Google Scholar]
- 27.Kuzik BA, Flavin MP, Kent S et al. Effect of inhaled hypertonic saline on hospital admission rate in children with viral bronchiolitis: a randomized trial. CJEM. 2010;12(6):477–484. doi: 10.1017/s1481803500012690. [DOI] [PubMed] [Google Scholar]
- 28.Ipek IO, Yalcin EU, Sezer RG, Bozaykut A. The efficacy of nebulized salbutamol, hypertonic saline and salbutamol/hypertonic saline combination in moderate bronchiolitis. Pulm Pharmacol Ther. 2011;24(6):633–637. doi: 10.1016/j.pupt.2011.09.004. [DOI] [PubMed] [Google Scholar]
- 29.Florin TA, Shaw KN, Kittick M et al. Nebulized hypertonic saline for bronchiolitis in the emergency department: a randomized clinical trial. JAMA Pediatr. 2014;168(7):664–670. doi: 10.1001/jamapediatrics.2013.5306. [DOI] [PubMed] [Google Scholar]
- 30.Jacobs JD, Foster M, Wan J, Pershad J. 7% Hypertonic saline in acute bronchiolitis: a randomized controlled trial. Pediatrics. 2014;133(1):e8–e13. doi: 10.1542/peds.2013-1646. [DOI] [PubMed] [Google Scholar]
- 31.Wu S, Baker C, Lang ME et al. Nebulized hypertonic saline for bronchiolitis: a randomized clinical trial. JAMA Pediatr. 2014;168(7):657–663. doi: 10.1001/jamapediatrics.2014.301. [DOI] [PubMed] [Google Scholar]
- 32.Mandelberg A, Tal G, Witzling M et al. Nebulized 3% hypertonic saline solution treatment in hospitalized infants with viral bronchiolitis. Chest. 2003;123(2):481–487. doi: 10.1378/chest.123.2.481. [DOI] [PubMed] [Google Scholar]
- 33.Tal G, Cesar K, Oron A et al. Hypertonic saline/epinephrine treatment in hospitalized infants with viral bronchiolitis reduces hospitalization stay: 2 years' experience. Isr Med Assoc J. 2006;8(3):169–173. [PubMed] [Google Scholar]
- 34.Luo Z, Liu E, Luo J et al. Nebulized hypertonic saline/salbutamol solution treatment in hospitalized children with mild to moderate bronchiolitis. Pediatr Int. 2010;52(2):199–202. doi: 10.1111/j.1442-200X.2009.02941.x. [DOI] [PubMed] [Google Scholar]
- 35.Luo Z, Fu Z, Liu E et al. Nebulized hypertonic saline treatment in hospitalized children with moderate to severe viral bronchiolitis. Clin Microbiol Infect. 2011;17(12):1829–1833. doi: 10.1111/j.1469-0691.2010.03304.x. [DOI] [PubMed] [Google Scholar]
- 36.Miraglia Del Giudice M, Saitta F, Leonardi S et al. Effectiveness of nebulized hypertonic saline and epinephrine in hospitalized infants with bronchiolitis. Int J Immunopathol Pharmacol. 2012;25(2):485–491. doi: 10.1177/039463201202500218. [DOI] [PubMed] [Google Scholar]
- 37.Sharma BS, Gupta MK, Rafik SP. Hypertonic (3%) saline vs 0.93% saline nebulization for acute viral bronchiolitis: a randomized controlled trial. Indian Pediatr. 2013;50(8):743–747. doi: 10.1007/s13312-013-0216-8. [DOI] [PubMed] [Google Scholar]
- 38.Bueno Campaña M, Olivares Ortiz J, Notario Munoz C et al. High flow therapy versus hypertonic saline in bronchiolitis: randomised controlled trial. Arch Dis Child. 2014;99(6):511–515. doi: 10.1136/archdischild-2013-305443. [DOI] [PubMed] [Google Scholar]
- 39.Everard ML, Hind D, Ugonna K et al. SABRE: a multicentre randomised control trial of nebulised hypertonic saline in infants hospitalised with acute bronchiolitis. Thorax. 2014;69(12):1105–1112. doi: 10.1136/thoraxjnl-2014-205953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Flores-Gonzalez JC, Dominguez-Coronel MT, Matamala-Morillo MA et al. Does nebulized epinephrine improve the efficacy of hypertonic saline solution in the treatment of hospitalized moderate acute bronchiolitis? A double blind, randomized clinical trial. Minerva Pediatr. 2014 [PubMed] [Google Scholar]
- 41.Gonzalez Caballero D, Gonzalez Perez-Yarza E. Acute bronchiolitis: fundamentals of a rational protocol. Ann Esp Pediatr. 2001;55(4):355–364. [PubMed] [Google Scholar]
- 42.Nenna R, Papoff P, Moretti C et al. Seven percent hypertonic saline—0.1% hyaluronic acid in infants with mild-to-moderate bronchiolitis. Pediatr Pulmonol. 2014;49(9):919–925. doi: 10.1002/ppul.22935. [DOI] [PubMed] [Google Scholar]
- 43.Petrigni G, Allegra L. Aerosolised hyaluronic acid prevents exercise-induced bronchoconstriction, suggesting novel hypotheses on the correction of matrix defects in asthma. Pulm Pharmacol Ther. 2006;19(3):166–171. doi: 10.1016/j.pupt.2005.03.002. [DOI] [PubMed] [Google Scholar]
- 44.Buonpensiero P, De Gregorio F, Sepe A et al. Hyaluronic acid improves “pleasantness” and tolerability of nebulized hypertonic saline in a cohort of patients with cystic fibrosis. Adv Ther. 2010;27(11):870–878. doi: 10.1007/s12325-010-0076-8. [DOI] [PubMed] [Google Scholar]
- 45.Midulla F, Scagnolari C, Bonci E et al. Respiratory syncytial virus, human bocavirus and rhinovirus bronchiolitis in infants. Arch Dis Child. 2010;95(1):35–41. doi: 10.1136/adc.2008.153361. [DOI] [PubMed] [Google Scholar]
- 46.Ojha AR, Mathema S, Sah S, Aryal UR. A comparative study on use of 3% saline versus 0.9% saline nebulization in children with bronchiolitis. J Nepal Health Res Counc. 2014;12(26):39–43. [PubMed] [Google Scholar]
- 47.Teunissen J, Hochs AH, Vaessen-Verberne A et al. The effect of 3% and 6% hypertonic saline in viral bronchiolitis: a randomised controlled trial. Eur Respir J. 2014;44(4):913–921. doi: 10.1183/09031936.00159613. [DOI] [PubMed] [Google Scholar]
- 48.Florin TA, Byczkowski T, Ruddy RM et al. Utilization of nebulized 3% saline in infants hospitalized with bronchiolitis. J Pediatr. 2015;166(5):1168–1174. doi: 10.1016/j.jpeds.2015.01.045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Zhang L, Mendoza-Sassi RA, Wainwright C, Klassen TP. Nebulised hypertonic saline solution for acute bronchiolitis in infants. Cochrane Database Syst Rev. 2013;7:CD006458. doi: 10.1002/14651858.CD006458.pub3. [DOI] [PubMed] [Google Scholar]