

Abstract
Background:
Human immunodeficiency virus (HIV)-positive adolescents by virtue of their position are prone to dangerous behaviors including risk-taking for HIV transmission.
Objective:
To determine the awareness of HIV status and risk factors for HIV transmission among HIV-positive adolescents, and how these impact their behavior.
Materials and Methods:
A case study approach was used to study a random sample of 400 HIV-positive adolescent children attending an antiretroviral (ART) clinic in Kano, Kano State, Nigeria. Data were analyzed using Statistical Package for the Social Sciences (SPSS) 16.0 computer statistical software.
Result:
The mean age of the adolescents was 14.9 ± 3.15 years. The majority were females (54.8%) from a polygamous family (57.5%). About two-thirds or 251 (62.8%) patients knew their HIV status. The age of 14 years and above (z = 11.36, P = 0.0001) and having at least secondary school level of education (z = 2.78, P = 0.005) were significantly associated with awareness of HIV status on binary logistic regression. Up to 311 (77.8%) patients had good awareness of the risks of HIV transmission. Awareness of risk of HIV transmission was associated with awareness of HIV status (X2 = 166.2, P = 0.0001). There was a significant variation in the behaviors between those who were aware of their HIV status and those who were not. Paradoxically, the percentage differences in risk-taking were remarkably high in all the variables examined, and were all in the direction of the adolescents who had good knowledge of the risk factors for HIV transmission.
Conclusion and Recommendation:
Health ministries, development partners working in this field, and behavioral change communication experts should develop formidable strategies for addressing this menace. There is also a dire need for further research in this area.
Keywords: Human immunodeficiency virus (HIV) disclosure, HIV positive adolescents, HIV risk behavior, Kano, Nigeria, risk factors for HIV
Introduction
Adolescence is a vulnerable stage of human development characterized by experimentations and risk-taking. Thus, HIV-positive adolescents by virtue of their position are prone to dangerous behaviors including risk-taking for HIV transmission.
By the end of 2012, the World Health Organization reported that there were approximately 2.1 million adolescents living with HIV globally, and this vulnerable population accounted for about one-seventh of all new HIV infections.(1) Over 90% of these infected adolescents live in sub-Saharan Africa where the burden of the disease is huge and only a few lessons have been learnt on the management of HIV-infected adolescents.(2)
Prevention and control of the spread of HIV has aroused global public health interest with a special focus on the developing world that is worst hit by the epidemic. Improving HIV awareness, safer sex. and healthy living are strategies for controlling the spread of this devastating virus within the adolescent population. Through counseling sessions in the clinics or during disclosure by parents or caregivers, infected adolescents get to know of their HIV status, how to cope with HIV, and about safer sex where necessary. Alarmingly, not all HIV-infected adolescents attend these counseling sessions or get disclosed their HIV status. Growing evidence suggests that many HIV-infected children under medical care are uninformed about their status.(3,4) The stigma attached to HIV and knowing when and how to talk to children about HIV are major reasons that make disclosure to children so sensitive.(5,6)
The World Health Organization recommends that HIV-positive children be gradually disclosed their status by 6-12 years.(7) Empirical evidence suggests that disclosure of HIV diagnosis in children is associated with positive and negative outcomes.(8,9) Positive outcomes include among others, promotion of trust, fewer behavioral challenges, better performance at school, better adherence to medications, and clinical support services, and coping better with the social environment.(3,9,10) Also, many of the children who know of their HIV status avoid behaviors that are risky for the transmission of the virus.(3) Interestingly, increase in behavioral problems and stress levels soon after disclosure are among the reported negative outcomes.(9,10,11) The divergent nature of reports challenge the effectiveness of HIV counseling and disclosure sessions.
This study sought to examine, through the lens of the health belief model (HBM), the disclosure status and awareness of HIV-positive adolescents accessing medical care regarding the risk factors of HIV transmission, and how these impacted their behavior. Findings from this study will be useful to HIV program managers, development partners, and researchers in packaging strategies and/or interventions for promoting healthy living and behavior of the adolescents and for normalizing HIV-related stigma and discrimination within the general public.
Theoretical framework
The HBM was used as the theoretical underpinning for this work. It is a psychological model that was first developed in the 1950s by social psychologists Hochbaum, Rosenstock, and Kegels working in the US Public Health Services.(12) It attempts to explain and predict health behaviors by focusing on the attitudes and beliefs of individuals. According to Jans and Becker, the model suggests that people's beliefs about health problems, perceived benefits of action and barriers to action, and self-efficacy explain the engagement (or lack of engagement) in health-promoting behavior. A stimulus or cue to action must also be present in order to trigger the health-promoting behavior.(13)
Materials and Methods
Setting
Murtala Muhammad Specialist Hospital (MMSH) is the largest and most attended secondary health facility in northern Nigeria, patronized by people from within and outside Kano State as well as the neighboring Niger Republic. The antiretroviral (ART) clinic in MMSH is one of earliest ART centers established by the Global Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) Initiative (GHAIN) project in Nigeria. It operates a full range of HIV treatment, care, and support services during the 5 working days of every week. There are approximately 8,000 adults and 10,000 pediatric clients presently on ART. On an average, 40 adolescent children attend the clinic during each working day.
Study design, subjects and sample size
We used a case study approach to study a sample of 400 HIV-positive adolescent children attending the ART clinic in MMSH. The sample size was determined using an appropriate statistical formula for estimating the minimum sample size for descriptive studies;(14) and ‘p’ equals 0.54 (prevalence of good knowledge of HIV and its transmission among adolescents) obtained from a previous study in Kano.(15) The calculated sample size was inflated to 400 to compensate for incomplete responses and other contingencies.
Sampling
A systematic sampling technique was used to select the subjects based on the number of monthly clinic attendance (800). With a sampling interval of two (i.e., 800/400), one in every two adolescent children was selected until the required sample size was met. The starting point for selection was determined by picking a random number from the clinic register between one and two. Subsequent respondents were identified by adding the sampling interval to the preceding respondents’ serial number until the required sample size was met.
Instrument and method of data collection
A pretested structured interviewer-administered questionnaire that was constructed based on reported findings from the literature was used for data collection. The questionnaire consisted of sections that elicited the sociodemographic characteristics of the respondents, their awareness of HIV and risks for HIV transmission, and the transmission behavior of the adolescents. The questionnaires were administered by four trained interviewers after obtaining informed consent and/or assent from the parents or adolescents as appropriate. Literate respondents indicated acceptance by signing the consent form while nonliterate participants affixed their thumbprint impressions. Permission and ethical clearance for the study were also sought and obtained from Murtala Mohammed Specialist Hospital (MMSH), Kano, Kano State, Nigeria and Health Research Ethics Committee of Aminu Kano Teaching Hospital (AKTH) Kano, Kano State, Nigeria. Data collection spanned from June 2014 to July 2014.
Data analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 16.0 (SPSS for Windows, Version 16.0. Chicago, SPSS Inc)computer statistical software. Absolute numbers and simple percentages were used to summarize categorical variables, whereas quantitative variables were summarized using means and standard deviation. The adolescents’ awareness of the risks of HIV transmission was scored and graded using a scoring system adapted from a past study where each correct answer was given one point and each wrong response was allocated no point.(15) The accrued points were subsequently graded in percentages. Out of the total of 9 points, respondents who scored 5 to 9 points were adjudged as having “good awareness,” whereas those who scored 0 to 4 points had “poor awareness” of the risks of HIV transmission. The chi-square test, Yates-corrected chi-square test, and Fisher's exact probability test were used for bivariate analysis involving categorical variables, and percentage difference was used to quantify the difference in measured variables between the adolescents who were aware of their status and those who were not aware. A P value ≤ 0.05 was considered to be statistically significant.
Results
Sociodemographic characteristics of the respondents
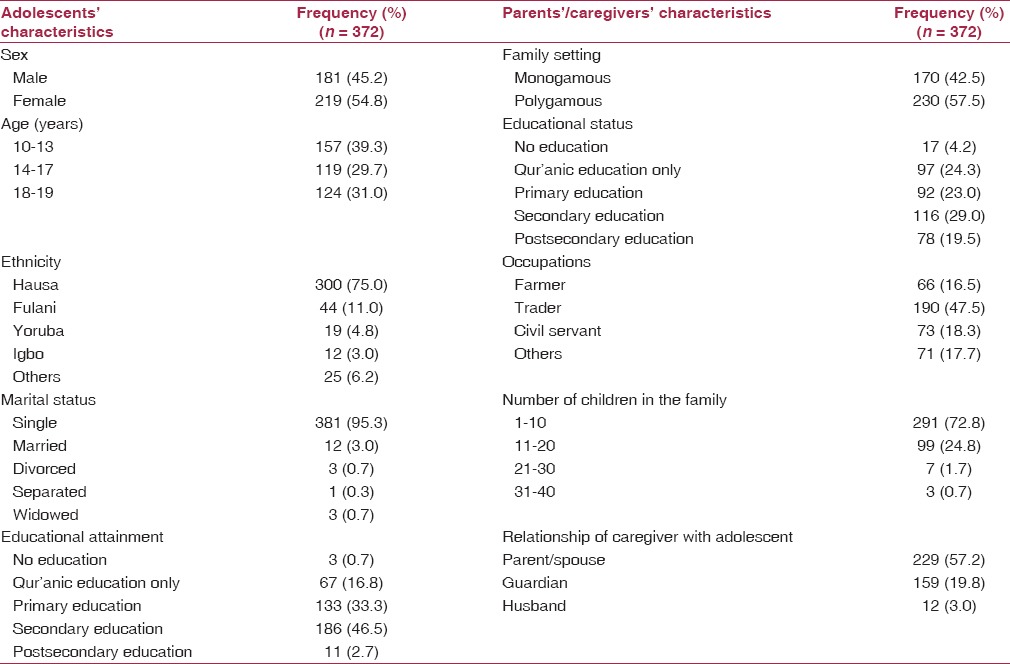
The majority of the adolescents studied were females (54.8%) and were from a polygamous family setting (57.5%). Their age ranged from 10 years to 19 years with a mean and standard deviation of 14.9 ± 3.15 years. Most of them came from the Hausa/Fulani tribes (86.0%) and were single (95.3%). About half (49.2%) had attained at least secondary school level of education.
The adolescents had been attending the ART clinic for an average duration of 46.1 ± 35.2 months (3.8 ± 2.9 years), with the majority (86.5%) attending the ART clinic for 1-80 months (6.7 years). The sociodemographic profile of the adolescents is as shown in Table 1.
Table 1.
Sociodemographic characteristics of the adolescents and their caregivers
Awareness of human immunodeficiency virus status and risks factors for human immunodeficiency virus transmission
About two-thirds of the adolescents, i.e., 251 (62.8%) knew of their HIV status, whereas the remaining 149 (37.2) did not know their status. The adolescents’ awareness of their HIV status was significantly associated with age (X2 = 290.8, P = 0.0001), the sex of the clients (X2 = 14.9, P = 0.0001), the level of education (X2 = 80.5, P = 0.0001), and the educational attainment of their mothers (X2 = 5.2, P = 0.02). However, it was not associated with their duration of attending the HIV clinic (X2 = 2.19, P = 0.139), ethnicity (X2 = 1.32, P = 0.250), and the educational status of their fathers (X2 = 3.27, P = 0.071).
On binary logistic regression using a model consisting of the factors significantly associated with the HIV adolescents’ awareness of HIV status, it was observed that older adolescents aged 14 years and above [z = 11.36, P = 0.0001, odds ratio (OR) {95% confidence interval (CI)} − 0.01(0.00; 0.020)] and having at least secondary school level of education [z = 2.78, P = 0.005, OR (95% CI) − 0.30 (0.13; 0.70)] were the only factors that emerged as independent predictors of their awareness of HIV status.
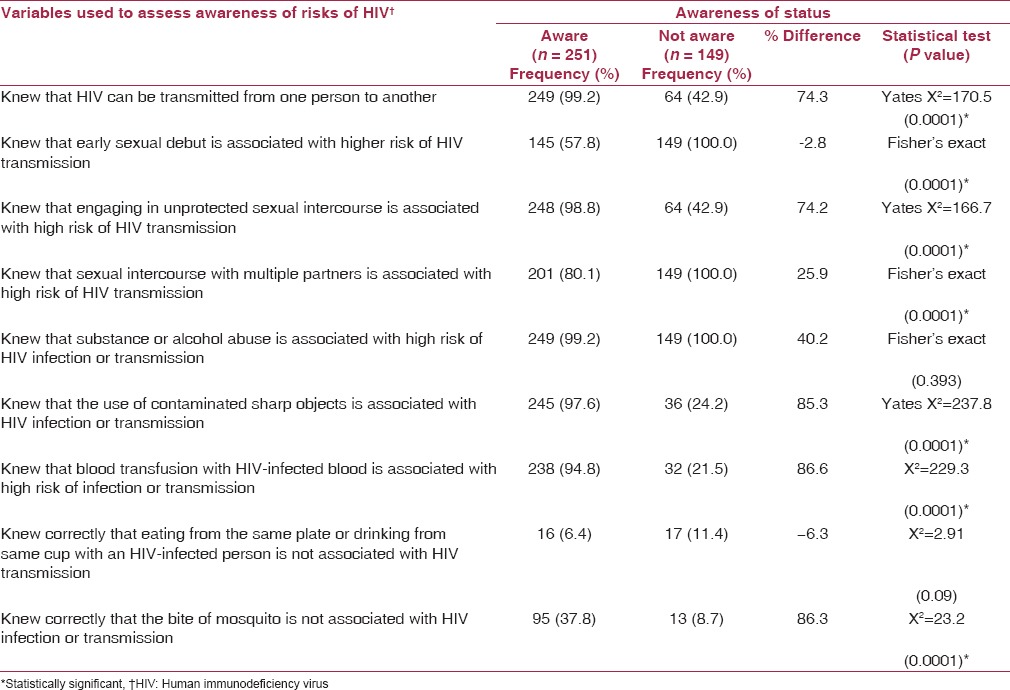
Awareness of the risks of HIV transmission between the adolescents who were aware of their HIV status and those who were not aware was significantly different in most of the variables used for the assessment. The percentage difference in awareness between the two groups was more than 70% and in favor of the group aware of their status in a majority of the variables used, as summarized in Table 2.
Table 2.
Relationship between the adolescents’ awareness of the risks of HIV transmission and their awareness of HIV status
When the adolescents’ awareness of the risks of HIV transmission was scored and graded, it was observed that 311 (77.8%) had good awareness of the risks of HIV transmission, whereas the remaining 89 (22.2%) had poor awareness. The result of cross-tabulating the awareness of risk of HIV transmission with the adolescents’ awareness of their HIV status showed that the two variables were significantly associated (X2 = 166.2, P = 0.0001). The adolescents who knew of their HIV status were more likely to have good knowledge of the risks of HIV transmission compared to their counterparts who did not know of their status [OR (95% C1) = 82 (28; 232)].
High risk behavior for transmission of human immunodeficiency virus
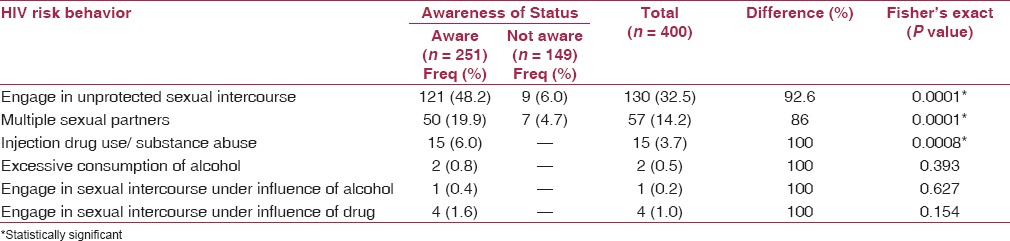
We examined the adolescents with respect to HIV high risk behavior including engaging in unprotected sexual intercourse, having multiple sexual partners, injection drug use/substance abuse, excessive consumption of alcohol, engaging in sexual intercourse under the influence of alcohol or under drug influence. We found a statistically significant variation in the behavior between those who were aware of their HIV status and those who were not. The percentage differences in the risky behaviors were very remarkable, and in the direction of the adolescents who were aware of their HIV status in all the variables examined [Table 3].
Table 3.
Relationship between the adolescents’ HIV risk behavior and their awareness of HIV status
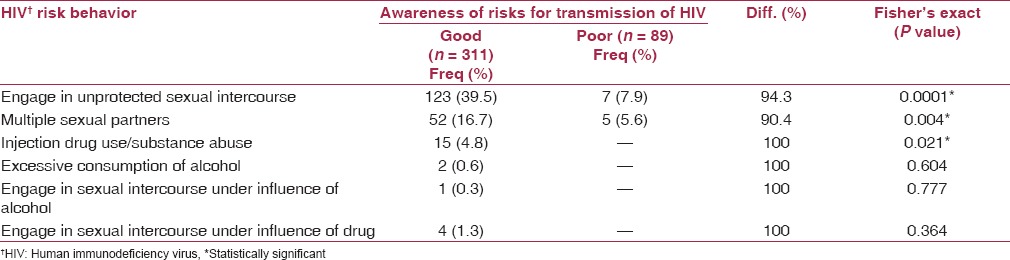
This study went further to examine the relationship between the adolescents’ awareness of the risk factors for transmission of HIV and their indulgence in HIV risk behavior. It also observed statistically significant variations in the risk-taking between the adolescents who had good awareness of the risk factors and those without it. Paradoxically, the percentage differences in the risk-taking was remarkably high in all the variables examined, and were all in the direction of the adolescents who had good knowledge of the risk factors for HIV transmission as shown in Table 4.
Table 4.
Relationship between awareness of risk factors for HIV transmission and HIV risk behavior
Discussion
HIV is more prevalent among the younger age group globally because of their sexually active nature, even though a proportion of this age group would have contacted the disease through mother to child transmission.(16) Although the study was conducted among adolescents of both sexes, the classes of adolescents that were predominant in the study were females, those within the mean age of 14.9 years, from polygamous homes, and those who were mostly single. This was not different from the picture seen in other studies were a majority of the young people with HIV were seen to be within this age group.(5,6,17) It is increasingly seen even in countries such as Zambia that women are disproportionately affected by HIV for many reasons ranging from biological to gender-based inequalities.(18)
The awareness of HIV status has been seen to play a key role in the prevention and control of HIV, especially among the sexually active group, for the adolescents in this study; some factors that were found to be significantly associated with the level of awareness of HIV status among others were age where the older ones with a higher level of education were more aware of their status than the others.(19) The importance of the awareness of one's HIV status has been highly linked to the knowledge of HIV prevention and this has been demonstrated in studies such as that conducted in Mozambique and the findings from this study.(20)
It has also been shown that people living with HIV who were aware of their HIV status engaged in less risky sexual behavior resulting in lower chances of HIV transmission compared to those who were unaware of their HIV status; and that the knowledge of the risk of sexual behavior among adolescents reduces their involvement in risky sexual behavior forming the platform on which educational programs on prevention are organized. However, some studies have shown that there is no relationship between HIV knowledge and risky sexual behavior.(21,22) The adolescents in this study who were aware of their HIV status demonstrated a significantly higher level of awareness of the risk of HIV transmission. Unfortunately, it did not translate into behavior change as quite a number of those who were aware of their status still engaged in high-risk behavior, a significant number of them had multiple sexual partners and had unprotected sex. The awareness of HIV status did not change the fact of adolescents still engaging in high-risk sexual behavior; and as reported in some studies, there is a growing increase in the rate of premarital and unprotected sex despite the high awareness of HIV while others have reported a low or inconsistent condom use among sexually active teenagers.(23,24) According to the HBT, the desire to avoid a negative health consequence is the prime motivator for positive health action.(25) The observed high risk sexual behavior of the adolescents in this study and others despite their awareness of the risks involved may perhaps be premised by the fact that the fear of getting infected with HIV has ceased to be a deterrent as they are already infected. This has serious consequences for the prevention and control of this deadly virus.
The question now is — what are the innovative strategies of reaching the adolescents and effecting a positive behavioral change if awareness of HIV status and counseling done in the HIV treatment centers seem not to have significantly changed high-risk sexual behavior among infected adolescents? It is therefore, recommended that health ministries, development partners working in this field, and behavioral change communication experts gear up toward packaging formidable strategies for addressing this menace. There is also a dire need for further research in this area.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Geneva: Joint United Nations Programme on HIV/AIDS; 2013. [Last accessed on 2014 Oct 20]. UNAIDS. HIV and Adolescents: Guidance for HIV Testing and Counseling and Care for Adolescents Living with HIV. Global Report: UNAIDS Report on the Global AIDS Epidemic 2013. Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2013/gr2013/UNAIDS_Global_Report_2013_en.pdf . [Google Scholar]
- 2.FMOH. National HIV/AIDS and Reproductive Health Survey (NARHS Plus, 2012). Federal Republic of Nigeria. Abuja, Nigeria. 2013. [Last accessed on 2014 Oct 20]. Available from: http://nascp.gov.ng/demo/wp-content/uploads/2014/02/NARHS-Plus-2012-Final-18112013.pdf .
- 3.Abadia-Barrero CE, Larusso MD. The disclosure model versus a developmental illness experience model for children and adolescents living with HIV/AIDS in São Paulo, Brazil. AIDS Patient Care STDS. 2006;20:36–43. doi: 10.1089/apc.2006.20.36. [DOI] [PubMed] [Google Scholar]
- 4.Heeren GA, Jemmott JB, 3rd, Sidloyi L, Ngwane Z. Disclosure of HIV diagnosis to HIV-infected children in South Africa: Focus group for intervention development. Vulnerable Child Youth Stud. 2012;7:47–54. doi: 10.1080/17450128.2012.656733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kennedy DP, Cowgill BO, Bogart LM, Corona R, Ryan GW, Murphy DA, et al. Parents’ disclosure of their HIV infection to their children in the context of the family. AIDS Behav. 2010;14:1095–105. doi: 10.1007/s10461-010-9715-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kallem S, Renner L, Ghebremichael M, Paintsil E. Prevalence and pattern of disclosure of HIV status in HIV-infected children in Ghana. AIDS Behav. 2011;15:1121–7. doi: 10.1007/s10461-010-9741-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Geneva: 2011. [Last accessed on 2015 Mar 11]. The World Health Organization. Guidelines for HIV Disclosure Counseling for Children Up To 12 Years of Age. WHO HIV/AIDS Programme. Available from: http://whqlibdoc.who.int/publications/2011/9789241502863_eng.pdf . [Google Scholar]
- 8.Vaz LM, Eng E, Maman S, Tshikandu T, Behets F. Telling children they have HIV: Lessons learned from findings of a qualitative study in sub-Saharan Africa. AIDS Patient Care STDS. 2010;24:247–56. doi: 10.1089/apc.2009.0217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wiener L, Mellins CA, Marhefka S, Battles HB. Disclosure of an HIV diagnosis to children: History, current research, and future directions. J Dev Behav Pediatr. 2007;28:155–66. doi: 10.1097/01.DBP.0000267570.87564.cd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.New York State Department of Health AIDS Institute/John Hopkins University. Disclosure of HIV to perinatally infected Children and Adolescents. [Last accessed on 2015 Mar 11]. Available from: http://www.hivguidelines.org/clinical-guidelines/infants-children/disclosure-of-hiv-to-perinatally-infected-children-and-adolescents/
- 11.Marini I, Stebnicky M. New York: Springer Publishing Company, LLC; 2012. Problem Behavior. Psychological and Social Impact of Illness and Disability; p. 256. [Google Scholar]
- 12.University of Twente. Health Belief Model. [Last accessed on 2015 Sep 10]. Available from: http://www.utwente.nl/cw/theorieenoverzicht/Theory%20Clusters/Health%20Communication/Health_Belief_Model/
- 13.Janz NK, Becker MH. The Health Belief Model: A Decade Later. [Last accessed on 2015 Sep 10]. Available from: http://deepblue.lib.umich.edu/bitstream/handle/2027.42/66877/10.1177_109019818401100101.pdf?sequence=2&isAllowed=y . [DOI] [PubMed]
- 14.Lwanga SK, Lemeshow S. Sample Size Determination in Health Studies, a Practical Manual. Publication of World Health Organization. 1991. [Last accessed on 2013 Nov 11]. pp. 1–3. Available from: http://apps.who.int/iris/handle/10665/40062 .
- 15.Lawan UM, Abubakar S, Gambo MD. HIV risk behaviors and knowledge of HIV/AIDS and its prevention among unmarried adolescents in Kano Metropolis, Northwestern Nigeria. J Behav Health. 2012;1:252–9. [Google Scholar]
- 16.UNAIDS. Fact Sheet: Adolescents, Young People and HIV. 2012. [Last accessed on 2014 Oct 18]. Available from: http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/factsheet/2012/20120417_FS_adolescentsyoungpeoplehiv_en.pdf .
- 17.Vaz L, Corneli A, Dulyx J, Rennie S, Omba S, Kitetele F, et al. AD Research Group.The process of HIV status disclosure to HIV-positive youth in Kinshasa, Democratic Republic of the Congo. AIDS Care. 2008;20:842–52. doi: 10.1080/09540120701742276. [DOI] [PubMed] [Google Scholar]
- 18.Fidelli US, Allen SA, Musonda R, Trask S, Hahn BH, Weiss H, et al. Virologic and immunologic determinants of heterosexual transmission of human immunodeficiency virus type 1 in Africa. AIDS Res Hum Retroviruses. 2001;17:901–10. doi: 10.1089/088922201750290023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Micek MA, Gimbel-Sherr K, Baptista AJ, Matediana E, Montoya P, Pfeiffer J, et al. Loss to follow-up of adults in public HIV care systems in central Mozambique: Identifying obstacles to treatment. J Acquir Immune Defic Syndr. 2009;52:397–405. doi: 10.1097/QAI.0b013e3181ab73e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dokubo EK, Shiraishi RW, Young PW, Neal JJ, Aberle-Grasse J, Honwana N, et al. Awareness of HIV status, prevention knowledge and condom use among people living with HIV in Mozambique. PLoS One. 2014;9:e106760. doi: 10.1371/journal.pone.0106760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kwara PA, Madise NJ, Hinde A. Perception of risk of HIV/AIDS and sexual behaviour in Kenya. J Biosoc Sci. 2003;35:385–411. doi: 10.1017/s0021932003003857. [DOI] [PubMed] [Google Scholar]
- 22.Guiella G, Madise NJ. HIV/AIDS and sexual-risk behaviors among adolescents: Factors influencing the use of condoms in Burkina Faso. Afr J Reprod Health. 2007;11:182–96. [PMC free article] [PubMed] [Google Scholar]
- 23.Rosenberg NE, Pettifor AE, De Bruyn G, Westreich D, Delany-Moretlwe S, Behets F, et al. HIV testing and counseling leads to immediate consistent condom use among South African stable HIV-discordant couples. J Acquir Immune Defic Syndr. 2013;62:226–33. doi: 10.1097/QAI.0b013e31827971ca. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Agha S. Factors associated with HIV testing and condom use in Mozambique: Implications for programs. Reprod Health. 2012;9:20. doi: 10.1186/1742-4755-9-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Resource Centre for Adolescent Pregnancy Prevention. Theories and Approaches: The Health Belief Model (HBM) [Last assessed on 2015 May 15]. Available from: http://recapp.etr.org/recapp/index.cfm?fuseaction=pages.theoriesdetail&PageID=13#definition .