

Abstract
Quantification of minimal residual disease may guide therapeutic strategies in mantle cell lymphoma. While multiparameter flow cytometry is used for diagnosis, the gold standard method for minimal residual disease analysis is real-time quantitative polymerase chain reaction (RQ-PCR). In this European Mantle Cell Lymphoma network (EU-MCL) pilot study, we compared flow cytometry with RQ-PCR for minimal residual disease detection. Of 113 patients with at least one minimal residual disease sample, RQ-PCR was applicable in 97 (86%). A total of 284 minimal residual disease samples from 61 patients were analyzed in parallel by flow cytometry and RQ-PCR. A single, 8-color, 10-antibody flow cytometry tube allowed specific minimal residual disease assessment in all patients, with a robust sensitivity of 0.01%. Using this cut-off level, the true-positive-rate of flow cytometry with respect to RQ-PCR was 80%, whereas the true-negative-rate was 92%. As expected, RQ-PCR frequently detected positivity below this 0.01% threshold, which is insufficiently sensitive for prognostic evaluation and would ideally be replaced with robust quantification down to a 0.001% (10-5) threshold. In 10 relapsing patients, the transition from negative to positive by RQ-PCR (median 22.5 months before relapse) nearly always preceded transition by flow cytometry (4.5 months), but transition to RQ-PCR positivity above 0.01% (5 months) was simultaneous. Pre-emptive rituximab treatment of 2 patients at minimal residual disease relapse allowed re-establishment of molecular and phenotypic complete remission. Flow cytometry minimal residual disease is a complementary approach to RQ-PCR and a promising tool in individual mantle cell lymphoma therapeutic management.
Introduction
Mantle cell lymphoma (MCL) is characterized by an advanced stage of disease at diagnosis, with most patients demonstrating peripheral blood or bone marrow infiltration. Historically, overall survival was short, but use of monoclonal anti-CD20 antibody and intensive treatment, including high-dose cytarabine and autologous stem cell transplantation (ASCT) have improved prognosis.1–7 Novel strategies, such as maintenance or pre-emptive treatment, may improve progression-free survival and prevent clinical relapse8–10 but are best used in combination with precise, reproducible, quantification of minimal residual disease (MRD).11 In the European Mantle Cell Lymphoma network (EU-MCL) study, multivariate analysis showed that MRD status at the end of induction is one of the strongest independent prognostic factors.2,11 Moreover, MRD-based pre-emptive rituximab therapy restored PCR-negativity in 81% of MCL patients.8
The gold standard for monitoring MRD in MCL is real-time quantitative polymerase chain reaction (RQ-PCR) amplification of clonal immunoglobulin heavy chain (IgH) VDJ or IgH-BCL1 rearrangements, which are informative in 90% and 40% of patients, respectively.8,12 Classical IgH or BCL1-IgH allele specific oligonucleotide (ASO)-based strategies use diagnostic DNA with a known level of infiltration,13 as defined by multiparameter flow cytometry (MFC) for construction of a standard curve. This approach can be difficult for samples in which the infiltration is very low (<1%), not known, (e.g. lymph node DNA), or in samples with unreliable MFC. It is necessary to distinguish quantifiable positivity from low-level MRD positivity. For this reason, it is common practice to specify for each patient undergoing RQ-PCR both the level of sensitivity of detection and the quantifiable range (QR), with values below the quantifiable range (BQR) but above sensitivity being positive but unquantifiable. These techniques are relatively long procedures, are costly and require significant expertise, justifying alternative MRD quantification techniques.
Multi-color flow cytometry assays with at least 6 colors have been applied to MRD monitoring in acute lymphoblastic leukemia,14,15 multiple myeloma,16–18 chronic lymphocytic leukemia,19 and hairy cell leukemia.20 To date, there are no established criteria for MRD quantification by MFC in MCL. An MCL 4-color panel using surface light chain restriction in the CD19+CD5+ subpopulation lacked sensitivity for MRD quantification, being inferior to consensus, qualitative PCR.21
We, therefore, developed a single, 8-color MFC tube for use in MCL and performed a pilot study on samples collected prospectively for molecular RQ-PCR MRD monitoring in EU-MCL patients. We analyzed the suitability of 8-color MFC for regular MRD evaluation, with a view to pre-emptive treatment on MRD relapse.
Methods
Patients’ characteristics and samples
Patients with previously untreated, histologically confirmed MCL of Ann Arbor stages II–IV were registered to one of two randomized EU-MCL clinical trials according to age and eligibility to receive an ASCT: patients up to 65 years of age to the MCL Younger trial (clinicaltrials.gov identifier: 00209222)2 and patients older than 60 years to the MCL Elderly trial (clinicaltrials.gov identifier: 00209209).9 Both protocols were approved by the institutional review boards of all participating institutions and were conducted according to the Declaration of Helsinki. Peripheral blood (PB) and/or bone marrow (BM) samples were collected at diagnosis, mid-term staging, end-of-induction and post induction at 2–3-monthly intervals until clinical relapse in both trials.2,9,11 Full details of treatment are given in the Online Supplementary Appendix. Response duration (RD) was defined only for patients who achieved at least a partial response (PR) after induction treatment and was calculated as the period from the completion of induction to documented progression or death from any cause, which were both considered as an event. Statistical analyses are detailed in the Online Supplementary Appendix.
Minimal residual disease analysis in France was centralized in 2 reference centers, one of which (Necker Hospital) performed the comparison presented here. The comparison of MFC and RQ-PCR was performed for patients with diagnostic data and at least one follow up. The number of samples analyzed by these techniques is indicated in Online Supplementary Table S1.
Multiparameter flow cytometry
Eight-color MFC was performed prospectively at diagnosis on fresh cells after Ficoll-separation, but on thawed cryopreserved cell for MRD samples. The cells were stained with a conjugated monoclonal antibody combination using CD3/CD14/CD56-(FITC), LAIR-1/CD305-(PE), CD19-(PeCy7), CD5-(PerCPCy5.5), CD11A-(APC), Lambda (Alexa700), Kappa (Pacific Blue) and CD45 (V500). All antibodies were from Becton-Dickinson (San Jose, CA, USA) except Kappa and Lambda (Exbio, Prague, the Czech Republic). MFC was performed on a FACS canto-II flow cytometer with DIVA software (Becton-Dickinson, USA) and standardized Euroflow instrument settings.22
For MRD assessment, 106 viable cells were stained with the diagnostic antibody panel and at least 200,000 non-gated events were acquired. In accordance with studies on MRD in acute leukemia,23–25 positive MFC MRD was defined by a homogenous cluster (>20 events) with the LAIP and scatter properties defined at diagnosis. MRD was quantified by dividing the number of MCL cells by the total number of events acquired (Online Supplementary Figure S1).
PCR-based MRD analysis
DNA from PB or BM was extracted by standard techniques and identification of clonal IgH rearrangement assessed using qualitative IgH-VDJ FR1 and FR2 consensus PCR on DNA extracted from the mononuclear fraction used for MFC. Gene scanning and sequence analyses (ABI prism automated sequencer Applied Biosystems, San Francisco, CA, USA) and ASO clone specific PCR were performed as described13 adapted for lymphoma,11 with identification of minimal sensitivity and QR for each patient. The minimum sensitivity considered acceptable was 10−4 (0.01%). Positive RQ-PCR MRD results were quantified if within the QR, and considered as BQR if below this range. All analyses were performed using a 1Ct RQ-PCR cut-off from background (see Online Supplementary Table S3 for details), which maximizes the number of BQR samples. BQR samples were separated on the number of positive triplicate wells.
Results
Sensitivity and specificity of MCL cell detection by MFC
We initially evaluated an antibody panel allowing assessment of tumor infiltration and identification of leukemia-associated immunophenotype (LAIP) on 51 cryopreserved diagnostic EU-MCL samples (experimental cohort). We combined the LAIR-1 and CD11a antibodies described in Euroflow standardization protocols22 with a standard backbone in a 10-antibody 8-color single tube. LAIR-1 and CD11a are expressed on normal blood B lymphocytes and other chronic B lymphoproliferations but not MCL.21,26,27 The backbone included well-defined antibodies previously used in 4-color MCL MRD strategies: CD45, CD19, CD5, Kappa and Lambda light chains, CD3, CD14 and CD56. Peripheral blood cells from 10 healthy donors were used as normal controls to evaluate the specificity and sensitivity of the antigenic combination.
Lymphocytes were identified by FSC/SSC properties and high CD45 expression. After exclusion of doublets, CD14+ monocytes, CD56+ NK cells and CD3+ T lymphocytes, MCL B cells were selected on a CD19/CD5 plot. The expression of CD11a and LAIR-1 and Kappa/Lambda isotypic restriction were then evaluated (Figure 2). Polyclonal B CD19+/CD5+ lymphocytes from 10 healthy donors expressed higher levels of both CD11a [MFI: median (range): 1729 (1426–2154)] and LAIR-1 [1859 (1150–2788)] compared to MCL samples, allowing the definition of a “physiological B-cell area”. In the 51 MCL patients, the intensity of expression [MFI: median (range)] of CD11a and LAIR-1 on pathological B cells was lower [681 (118–4986) and 416 (15–4013)], respectively. In 41 of 51 (80%) cases, MCL cells expressed low levels of CD11a and LAIR-1 and fell in an area defined as the “mantle box” (Figure 3, lower left quadrant). In the remaining cases, 5 of 51 (10%) were CD11alow/LAIR-1high or CD11ahigh/LAIR-1low. No CD11ahigh/LAIR-1high cases were detected (Figure 3). As such, the association of CD11a and LAIR-1 rescued cases with high expression of one of these antigens, increasing LAIP discrimination power in comparison to a CD19/CD5/Kappa/Lambda combination. Among the 51 MCL cases, 49 (96%) were detected outside the “physiological B-cell area”. Only 2 (4%) expressed CD11a and LAIR-1 levels close to those of normal B cells but light chain isotypic restriction allowed accurate MRD evaluation for these cases. Thus, the single tube antibody panel allowed the identification of at least one specific LAIP in almost all MCL cases tested [49 of 51 (96%)].
Figure 2.
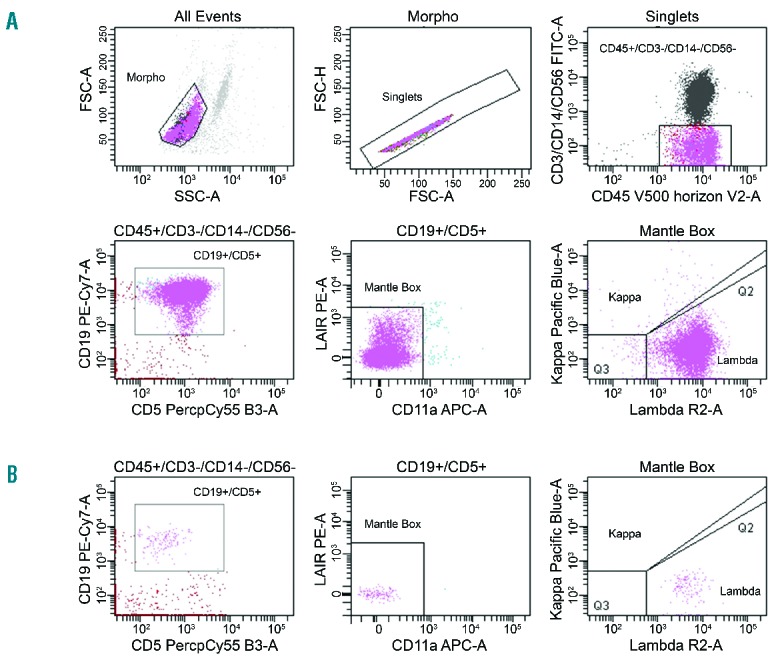
Gating strategy to assess mantle cell lymphoma involvement and evaluate LAIP in a diagnostic peripheral blood (PB) sample (A) and to quantify MFC MRD in a follow-up PB sample (B) from a patient included in the EU-MCL trial.
Figure 3.
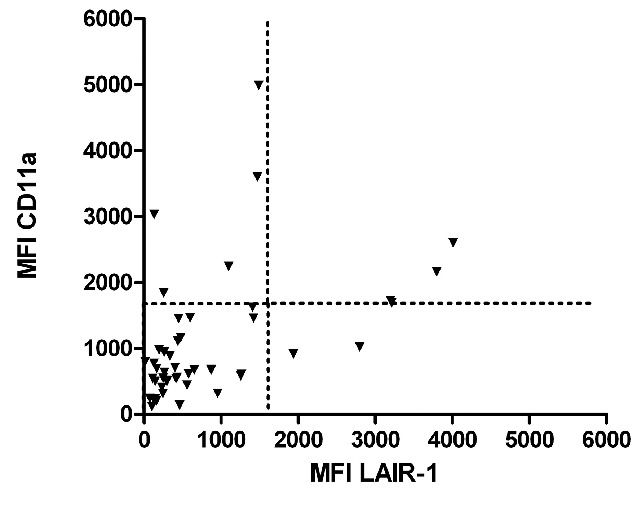
CD11a and LAIR mean fluorescent intensity (MFI) on diagnostic mantle cell lymphoma samples in the experimental cohort (n=51 patients).
We then evaluated the specificity and sensitivity of this single tube on 10 normal blood samples. Analysis of 1.106 cells gave less than 7.10−5 non-specific events in the “mantle box” [range 32 (3.10−5) to 63 (6.10−5) events], giving a theoretical sensitivity of at least 0.01%/10−4 (Online Supplementary Table S2 and Figure S1). Serial dilutions of diagnostic samples in normal PB showed that the sensitivity of discrimination of mantle cells from polyclonal background was 10−4 (data not shown). These data demonstrate that the use of a single, 8-color MFC tube allows specific flow cytometric MRD assessment in all patients tested, with a robust sensitivity of 10−4.
Assessment of MCL by MFC
A total of 195 diagnostic samples (115 PB and 80 BM) from 116 EU-MCL patients (including the 51 aforementioned samples) were analyzed with the MFC panel. No lymphoma cells were detected, with a 10−2 sensitivity, in 20 diagnostic samples (10 PB, 10 BM) from 11 MCL patients. MFC MRD was not performed for these patients. Infiltration at diagnosis was at least 1% in 164 of 175 (94%) samples (97 of 105 PB, 67 of 70 BM), with a median of 16%. Lower level infiltration between 0.01% and 0.9% was seen in 11 samples (Online Supplementary Figure S2). At least one LAIP, based on low CD11a and/or LAIR expression and Kappa/Lambda restriction, was identified in 175 samples, allowing MRD evaluation with a robust sensitivity of 0.01%/10−4 in 105 of 116 (91%) patients.
A total of 294 MRD samples (211 PB and 83 BM) were quantified by MFC at specified time points (see Online Supplementary Table S1). Overall, MRD was undetectable, below 0.01%, in 236 (80%) samples (172 PB, 64 BM). MFC positivity was detected in 58 (20%) samples (39 PB, 19 BM), with 34 samples between 0.01%–0.09%, 11 between 0.1%–0.9% and 13 up to 1%.
MCL assessment by RQ-PCR
At least one diagnostic PB, BM or lymph node sample was submitted for prospective RQ-PCR from 131 MCL patients. Of these patients, at least one MRD sample was available for 113. Nine (8%) patients had no available tissue DNA, less than 1% infiltration by MCL cells by MFC and no clearly detectable clonal population by IgH-VDJ and BCL1-IgH PCR. It was not possible to sequence or to obtain an ASO IgH or BCL1-IgH RQ-PCR system with acceptable sensitivity in 7 patients, despite at least 1% infiltration by MFC. In the remaining 97 of 113 (86%) patients, the RQ-PCR strategy was sufficiently sensitive (minimum 0.01%) and specific for MRD quantification (Figure 1). These 97 patients underwent RQ-PCR MRD quantification (Figure 1) of IgH-VDJ targets in 92, BCL1-IgH in 5 and both in 11. Although the RQ-PCR sensitivity was below 0.01% in all patients, the QR was above 0.01% in 26 patients (27%); it was between 0.02% and 0.05% in 19 and between 0.06% and 0.2% in 7.
Figure 1.
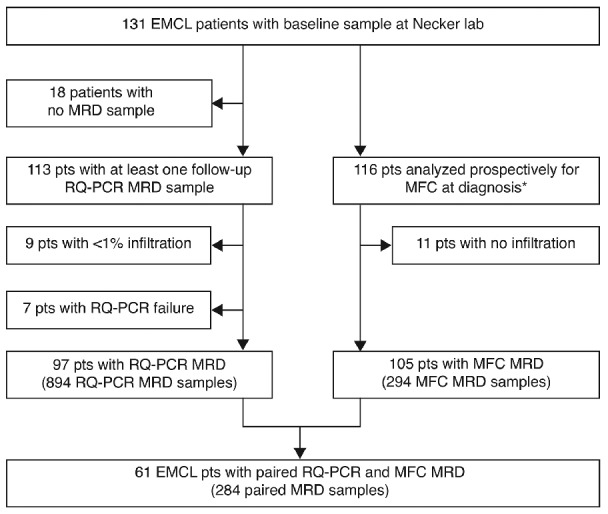
Flow chart for EU-MCL patients. *Including 51 samples from the experimental cohort.
Qualitative PCR allowed identification of a distinct clonal peak which could be sequenced in 95% (99 of 104) of diagnostic samples with a MFC population of at least 1%, but also in 9 samples for whom MFC was lower than 1% and 14 patients for whom MFC was not possible, including 7 lymph node DNA samples. In these patients, the diagnostic sample infiltration used for the patient-specific standard curves construction was deduced from its RQ-PCR CT value, using a MFC/PCR regression curve obtained from 100 diagnostic PB/BM MCL samples with at least 1% infiltration by MFC (Online Supplementary Figure S3). This increased the number of patients accessible to RQ-PCR MRD from 74 (65%) to 97 (86%) of the 113 EU-MCL patients with at least one MRD sample. Suboptimal QR were no more frequent in these patients (5 of 23, 22%) than those with MFC values above 1% (21 of 74, 28%).
A total of 894 MRD samples (639 PB and 255 BM) from 97 EU-MCL patients were quantified by RQ-PCR (see Figure 4 and Online Supplementary Table 1S for time points), of which 173 (19%) were positive quantifiable, 180 (20%) positive below the quantifiable range (BQR), and 541 (61%) negative. As such, half the positive MRD samples were within the low-level non-quantifiable range. We, therefore, compared IgH-VDJ RQ-PCR with MFC assessment and with RQ-PCR quantification of BCL1-IgH, distinguishing BQR samples on the number of positive wells within the triplicates analyzed.
Figure 4.
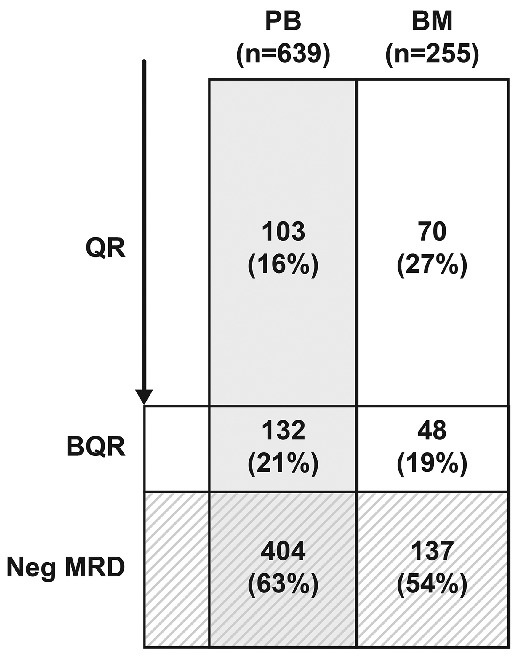
RQ-PCR results from 97 (49 elderly and 48 younger) EU-MCL patients.
Comparison of RQ-PCR and MFC MRD values
MFC was compared with RQ-PCR in 284 samples (207 PB and 77 BM) from 61 patients (32 younger and 29 elderly). These included 153 of 541 (28%) RQ-PCR negative and 131 of 355 (37%) RQ-PCR positive samples (Figure 1).
Using cut-off levels of at least 0.01% positivity for RQ-PCR, 80% (39 of 49) of samples were also positive by MFC (Cohen kappa of 0.6666, P<0.0001), giving a true-positive rate of MFC MRD evaluation of 80% and a true-negative rate of 92% (Table 1). Below this level, agreement dropped due to the significant number of samples which were positive by RQ-PCR but negative by MFC. MFC-/RQ-PCR+ samples included 19 positive quantifiable and 54 positive BQR results by RQ-PCR. Conversely, MFC+/RQ-PCR-less-than-0.01% samples included 4 positive quantifiable samples, 14 BQR, and only one negative sample by RQ-PCR. A significantly higher proportion of BQR samples with at least 2 positive triplicates were MFC positive (17 of 62, 27%; Cohen kappa 0.5391, P<0.0001) compared to virtually none of those with only 1 or no triplicate above sensitivity (2 of 173, 1%) (Cohen kappa 0.4515, P<0.0001) (Online Supplementary Figure S4).
Table 1.
Multiparameter flow cytometry positivity as a function of the level of RQ-PCR MRD positivity in 284 samples from 61 patients.

If all levels of RQ-PCR positivity are considered, amongst 154 RQ-PCR negative samples, only one was positive by MFC, at 0.07% (RQ-PCR sensitivity and QR of 0.01%). Of the 62 RQ-PCR positive-quantifiable MRD samples, 43 (69%) were also positive by MFC, whereas 19 (31%) samples from 11 patients were considered negative by MFC. Overall, 14 of 68 (21%) BQR samples were also positive by MFC (Table 1 and Figure 5). The incidence of MFC positivity in samples with two or three positive triplicate PCR analyses was not significantly lower than quantifiable samples, below 0.01% by RQ-PCR (13 of 49 vs. 4 of 13 respectively; P=0.6667), whereas this incidence fell in samples with only 1 of 3 positive triplicates, when it was not significantly different from samples considered negative by PCR (1 of 19 vs. 1 of 154; P=0.2207). Restriction of criteria for MRD low-level positivity to samples with at least 2 of 3 positive triplicates reduced the overall incidence of positivity from 46% to 39% of the 284 samples analyzed (Table 1). The RQ-PCR BQR samples that were positive by MFC were all below 0.1%. Similarly, all but one of the RQ-PCR quantifiably positive samples, which were negative by MFC, were below 0.1% (18 of 19) (Table 1 and Figure 5).
Figure 5.
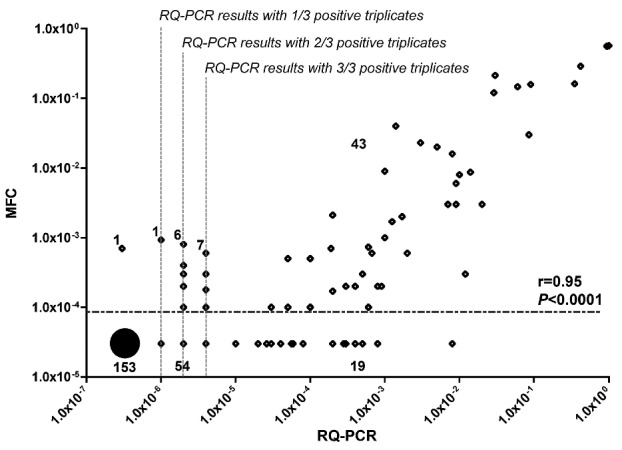
Visual representation of paired minimal residual disease (MRD) evaluated by multiparameter flow cytometry (MFC) and RQ-PCR. Underlined numbers refer to the total number of samples in the corresponding quadrant. Pearson correlation coefficient of the 62 MRD in which RQ-PCR provided quantifiable MRD results and MFC provided either positive or negative results was calculated with Pearson correlation test.
In 62 of 284 samples with quantifiable RQ-PCR MRD and positive or negative MFC MRD, values correlated well (Pearson correlation coefficient r=0.95, P<0.0001) (Figure 5). A Bland-Altman analysis28 showed higher MFC-based MRD values with a mean difference of 0.0862 log and a relatively wide range between the 95% limits of agreement (95%CI: −1.1525; 1.3249) (Online Supplementary Figure S5).
The Euro-MRD network defined two criteria for definition of BQR positivity, with a 3Ct or 1Ct difference from first background positivity.13 Re-analysis of data using these more restrictive criteria for positivity (Online Supplementary Table S3) led to a diminution of BQR samples from 68 of 284 (24%) to 53 of 284 (19%).
We also compared IgH-VDJ and BCL1-IgH ASO RQ-PCR results for 48 MRD samples from 11 patients. Twelve of 13 samples positive above 0.01% by IgH-VDJ or BCL1-IgH gave identical results (Online Supplementary Figure S6). All 11 IgH-VDJ BQR results with 2 or 3 positive triplicates were also BCL1-IgH positive, in contrast to only 3 of 9 IgH BQR with one positive triplicate. These data are in keeping with the MFC-IgH RQ-PCR comparison.
Taken together, this comparison shows comparable results for MFC and quantifiable positive RQ-PCR results (Pearson correlation coefficient r=0.95, P<0.0001) but a greater sensitivity for RQ-PCR, when the identification of at least 2 of 3 positive triplicate results detects veritable low level positivity.
Prognostic relevance of MFC MRD values
A total of 33 patients with MRD data and a documented clinical remission after induction were evaluable for assessment of the prognostic impact of MFC MRD status at the end of induction. Patients achieving a negative MFC MRD after induction (n=26) demonstrated a non-significant trend for prolonged remission duration (RD) compared with patients with residual disease (n=7; P=0.1496) (Figure 6A), Comparable results were obtained for RD based on end-of-induction RQ-PCR MRD status with a 0.01% positivity cut off (28 of 33 MRD negative patients). In contrast, when using an RQ-PCR positive cut off, including BQR positivity, the 13 MRD negative patients required re-treatment significantly later than the 20 MRD positive patients (P=0.0014) (Figure 6B). There was no difference in RD when patients with MRD results showing a single positive triplicate were considered negative (Figure 6B) in this small cohort (16 of 33 MRD negative patients). These data confirm that MFC and RQ-PCR are comparable above 0.01% sensitivity levels, but that the greater sensitivity of the latter improves predictive value for remission duration.
Figure 6.
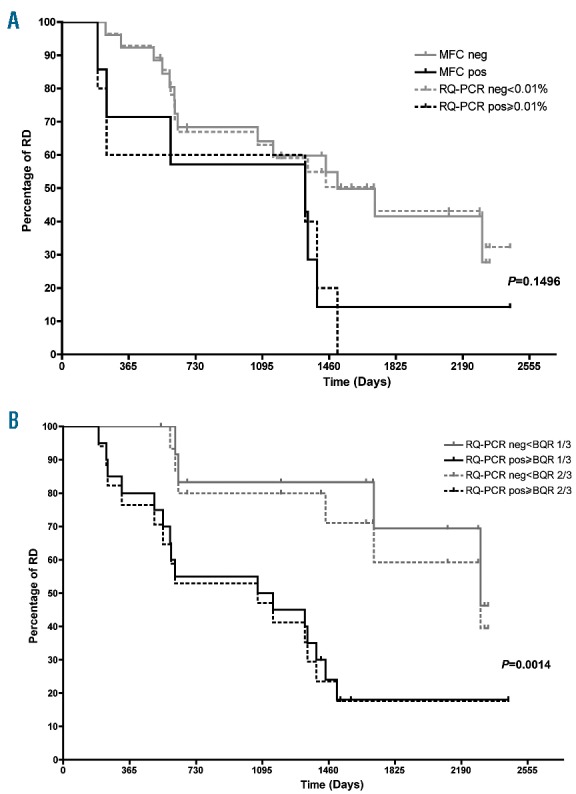
Response duration (RD) according to minimal residual disease (MRD) status in peripheral blood (PB) and/or bone marrow (BM) after the end of induction in 33 mantle cell lymphoma (MCL) younger and elderly patients. RD according to multiparamter flow cytometry (MFC) (7 of 33 MRD positive patients) and RQ-PCR (5 of 33 MRD positive patients) with a 0.01% cut off (6A) and RQ-PCR with a negative/positive cut off, solid lines (20 of 33 MRD positive patients with at least one positive triplicate; 6B) or a 1 vs. 2 of 3 triplicate cut off, dashed line (17 of 33 MRD positive patients with at least 2 positive triplicates). Gray lines indicate negative MRD and black lines positive MRD.
MRD relapse precedes clinical relapse and allows pre-emptive treatment
Amongst 61 patients with at least one paired MRD analysis, 29 relapsed and 19 died. Analysis of relapse kinetics was restricted to PB MRD values, since regular monitoring makes this a more appropriate source of material. Ten relapsing patients had sufficient MRD points to assess the capacity of RQ-PCR or MFC to predict future clinical relapse. For relapse kinetics, samples with only one positive triplicate were considered negative but are represented graphically at 10−7, (Figure 7) whereas two or three positive triplicates were considered to be MRD positive (represented graphically at 10−6).
Figure 7.

Kinetics of minmal residual disease (MRD) evolution. RQ-PCR (gray) and multiparameter flow cytometry (MFC) (black) quantification of peripheral blood samples at indicated dates. Negative RQ-PCR values are shown as 1E-08, single triplicate BQR results at 1E-07 and 2 or 3 positive triplicates at 1E-06. The horizontal dotted lines represent individual QR and MFC sensitivity, as labeled. Negative MFC results are shown just below 10E-4 (0.01%). RQ-PCR and MFC MRD relapses, respectively, 26 and five months before clinical relapse (A). Pre-emptive treatment based on rising RQ-PCR and/or MFC MRD results (B).
Clinical relapse was preceded by MRD relapse in all patients by RQ-PCR, compared to 6 of 8 by MFC (Figure 6 and Online Supplementary Table S4). If only positive results above 0.01% were taken into account, MRD relapse preceded clinical relapse in 7 of 10 patients. The median latency for prediction by RQ-PCR when any increase to at least 2 positive triplicates was considered as MRD relapse was 22.5 months (range 1–48 months) and 5 months (range 2–11 months) when only results above 0.01% were considered positive. Latency by MFC was similar to the latter, at 4.5 months (range 2–18 months). No relapse tissue was available for the patients whose relapses had not been predicted (Online Supplementary Table S4).
Although the number of patients is limited, these data suggest that regular MFC and RQ-PCR monitoring may facilitate pre-emptive treatment, with sufficient latency to allow appropriate therapeutic modification. As proof of principle, 2 patients treated locally off protocol underwent an MRD relapse (one relapsed twice) with no evidence of clinical or hematologic relapse, and were treated with rituximab with rapid molecular and phenotypic response (Figure 7B), followed by 3-monthly maintenance. This led to a 4-year remission in one patient, with the second currently in CR under maintenance.
Discussion
Monitoring MRD in MCL clearly has a place in prognostic evaluation, therapeutic stratification,11 and assessment of pre-emptive treatment,8 underlining the need for optimal MRD surveillance during remission, with therapeutic modification at MRD conversion or relapse. Gold standard IgH RQ-PCR MRD quantification is sensitive but relatively complex and time consuming, and has a high proportion of low-level positive results below the quantifiable range. As such, it may be less easily adapted for immediate, individual patient management than MFC. MFC MRD should be faster and cheaper than molecular analysis but FC was, until recently, insufficiently sensitive.21 We and others have shown that MFC can give comparable results to Ig/TCR MRD for levels above 0.01% in acute lymphoblastic leukemia,14 chronic lymphocytic leukemia,29 and hairy cell leukemia,20 with complementary informativity. We now demonstrate that this is also the case for MCL.
At diagnosis, it was possible to identify at least one MCL LAIP in all patients followed by RQ-PCR. The latter was possible for 86% of patients overall, including 16 with no or insufficient MFC infiltration for identification of a diagnostic LAIP. Conversely, 7 patients had an identifiable MCL population by MFC but no satisfactory clone-specific RQ-PCR probes. Only 9 of 113 (8%) of patients could not access either approach, demonstrating that MFC and RQ-PCR are complementary. Phenotypic evolution during the course of the disease is a potential risk of MFC, but the 8-color strategy described here reduced the risk of false negative results by increasing the number of LAIP per patient. MFC MRD quantification is based on the detection of MCL cells within a large number of normal B lymphocytes. We demonstrate a robust sensitivity of at least 0.01%, on analysis of at least 200,000 cells. This could obviously be increased by increasing the number of cells analyzed, as long as the number of normal B lymphocytes in the “MCL-box” remains low/absent. Using a cut-off level of 0.01%, RQ-PCR and MFC MRD values correlated significantly, although MFC was negative in 10 of 49 samples (20%). It should be emphasized that this is a retrospective study of thawed cryopreserved Ficoll MRD samples, which may underestimate MFC sensitivity, relative to prospective whole blood samples. MFC MRD was specific, as demonstrated by the virtual absence of RQ-PCR negative/MFC positive cases.
Multiparameter flow cytometry, with a sensitivity limit of 0.01%, would be expected to be negative in the vast majority of RQ-PCR BQR samples. This was indeed the case for samples with only one positive triplicate (1 of 19, 5%) but not in samples with 2 or 3 positive triplicates (13 of 49, 27%), when the incidence of positivity was similar to quantifiable samples below 0.01% (4 of 13, 31%). This probably reflects the significant variability in QR values between patients, since 8 of 15 MFC+/BQR samples had QR above 0.01%, compared to 27% of patients overall. Inter-patient variability and acceptable QR limits should be optimized, ideally with a QR of at least 0.01% in all patients. The use of more stringent criteria for low-level MRD positivity will reduce the proportion of BQR samples by 5%–10% overall, or 10%–25% of positive samples. Whether this will improve the positive and negative predictive value of MRD needs to be evaluated in prospective studies. It is possible that even very low levels of MRD positivity should be used for therapeutic stratification, as demonstrated for remission duration in this study, in which case RQ-PCR is preferable to MFC, unless at least one log more cells can be quantified with the latter. It is probable that combined, integrated use of MFC and RQ-PCR will provide optimal MCL follow up. The recent demonstration that next generation sequencing strategies will improve informativity and sensitivity30 also underline the need for a combined approach, as will the use of droplet digital PCR.31
In practice, therapeutic modification is rarely based on a single MRD result. The clinical relevance of MFC and RQ-PCR MRD assessment could be analyzed for 10 patients undergoing first relapse. The transition from negative to positive, including BQR RQ-PCR (median 22.5 months) nearly always preceded negative to positive transition by MFC (4.5 months), but RQ-PCR positivity above 0.01% did not differ (5 months). These delays are compatible with pre-emptive treatment in the majority of relapsing patients. If therapeutic intervention is to be considered, the interval for PB surveillance should probably be 3-monthly. It should, however, be noted that MRD gave less than a 3-month warning in 3 of 10 patients. Failure to detect relapse may reflect clonal evolution or relapse as purely nodal disease, or even the appearance of a novel B-lymphoproliferative disorder. Distinguishing between these possibilities will require histological and molecular analysis of relapse tissue. As proof of concept, pre-emptive treatment of 2 patients at MRD conversion prior to clinical relapse allowed re-establishment of molecular and phenotypic complete remission and a durable second remission. It remains unknown what the MRD threshold for starting pre-emptive treatment should be, and analysis of individual MRD kinetics for a larger number of patients is clearly required. Similarly, MRD kinetics following novel agents such as idelalisib need to be studied. MFC (or limiting RQ-PCR positivity to samples with at least 2 of 3 positive triplicates) might also be useful in the interpretation of low-level positive results, potentially avoiding excessively early therapeutic stratification.8
Molecular remission is an independent prognostic factor of clinical outcome.11 With its greater sensitivity, RQ-PCR MRD is better suited to prognostic analysis but MFC MRD may be more clinically relevant and feasible in individual therapeutic management. We need to clarify the optimal integration of these complementary techniques, their timing and the definition of MRD relapse, in order to optimize comparison between studies. MFC clearly has a place in MCL management, which needs further evaluation in a prospective setting.
Acknowledgments
We thank Franck Morschhauser, Loic Ysebaert, François Boue, Celia Salanoubat, Michel Fabbro, Eric Jourdan, Sylvie Castaigne, Maud Janvier, Pierre Fenaux, Lina Al Jassem, Hugo Gonzalez and Marie Beaumont for contributing diagnostic and MRD samples for EU-MCL patients and Carine Deschodt and Fabienne Morand for help with sample management.
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/101/3/336
Funding
This work was supported by the Institut National du Cancer (INCa) PAIR Lymphoma program on Mantle Cell Lymphoma and by the Lymphoma Study Association (LYSA).
References
- 1.Dreyling M, Lenz G, Hoster E, et al. Early consolidation by myeloablative radiochemotherapy followed by autologous stem cell transplantation in first remission significantly prolongs progression-free survival in mantle-cell lymphoma: results of a prospective randomized trial of the European MCL Network. Blood. 2005;105(7):2677–2684. [DOI] [PubMed] [Google Scholar]
- 2.Hermine O, Hoster E, Walewski J, et al. Alternating courses of 3xCHOP and 3xDHAP plus rituximab followed by a high dose ARA-C containing myeloablative regimen and autologous stem cell transplantation increases overall survival when compared to 6 courses of CHOP plus rituximab followed by myeloablative radiochemotherapy and ASCT in mantle cell lymphoma: final analysis of the MCL Younger Trial of the European mantle cell lymphoma Network. Hematol Oncol. 2012: abstract 151 Presented at: ASH Annual Meeting, Atlanta, GA, USA, 8–11 December 2012. [Google Scholar]
- 3.Geisler CH, Kolstad A, Laurell A, et al. Long-term progression-free survival of mantle cell lymphoma after intensive front-line immunochemotherapy with in vivo-purged stem cell rescue: a nonrandomized phase 2 multicenter study by the Nordic Lymphoma Group. Blood. 2008;112(7): 2687–2693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Romaguera JE, Fayad L, Rodriguez MA, et al. High rate of durable remissions after treatment of newly diagnosed aggressive mantle-cell lymphoma with rituximab plus hyper-CVAD alternating with rituximab plus high-dose methotrexate and cytarabine. J Clin Oncol. 2005;23(28):7013–7023. [DOI] [PubMed] [Google Scholar]
- 5.Lenz G, Dreyling M, Hoster E, et al. Immunochemotherapy with rituximab and cyclophosphamide, doxorubicin, vincristine, and prednisone significantly improves response and time to treatment failure, but not long-term outcome in patients with previously untreated mantle cell lymphoma: results of a prospective randomized trial of the German Low Grade Lymphoma Study Group (GLSG). J Clin Oncol. 2005;23(9):1984–1992. [DOI] [PubMed] [Google Scholar]
- 6.Delarue R, Haioun C, Ribrag V, et al. CHOP and DHAP plus rituximab followed by autologous stem cell transplantation in mantle cell lymphoma: a phase 2 study from the Groupe d’Etude des Lymphomes de l’Adulte. Blood. 2013;121(1):48–53. [DOI] [PubMed] [Google Scholar]
- 7.Lefrère F, Delmer A, Levy V, et al. Sequential chemotherapy regimens followed by high-dose therapy with stem cell transplantation in mantle cell lymphoma: an update of a prospective study. Haematologica. 2004;89(10):1275–1276. [PubMed] [Google Scholar]
- 8.Andersen NS, Pedersen LB, Laurell A, et al. Pre-emptive treatment with rituximab of molecular relapse after autologous stem cell transplantation in mantle cell lymphoma. J Clin Oncol. 2009; 27(26):4365–4370. [DOI] [PubMed] [Google Scholar]
- 9.Kluin-Nelemans HC, Hoster E, Hermine O, et al. Treatment of older patients with mantle-cell lymphoma. N Engl J Med. 2012;367(6):520–531. [DOI] [PubMed] [Google Scholar]
- 10.Le Gouill S, Thieblemont C, Oberic L, et al. Rituximab maintenance versus wait and watch after four courses of R-DHAP followed by autologous stem cell transplantation in previously untreated young patients with mantle cell lymphoma: first interim analysis of the phase III prospective LyMa trial, a Lysa study. Hematol Oncol. 2014: abstract 146 Presented at: ASH Annual Meeting, Atlanta, GA, USA, 6–9 December 2014. [Google Scholar]
- 11.Pott C, Hoster E, Delfau-Larue M-H, et al. Molecular remission is an independent predictor of clinical outcome in patients with mantle cell lymphoma after combined immunochemotherapy: a European MCL intergroup study. Blood. 2010;115(16): 3215–3223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pott C, Schrader C, Gesk S, et al. Quantitative assessment of molecular remission after high-dose therapy with autologous stem cell transplantation predicts long-term remission in mantle cell lymphoma. Blood. 2006;107(6):2271–2278. [DOI] [PubMed] [Google Scholar]
- 13.Van der Velden VHJ, Cazzaniga G, Schrauder A, et al. Analysis of minimal residual disease by Ig/TCR gene rearrangements: guidelines for interpretation of real-time quantitative PCR data. Leukemia. 2007;21(4):604–611. [DOI] [PubMed] [Google Scholar]
- 14.Garand R, Beldjord K, Cavé H, et al. Flow cytometry and IG/TCR quantitative PCR for minimal residual disease quantitation in acute lymphoblastic leukemia: a French multicenter prospective study on behalf of the FRALLE, EORTC and GRAALL. Leukemia. 2013;27(2):370–376. [DOI] [PubMed] [Google Scholar]
- 15.Schrappe M. Minimal residual disease: optimal methods, timing, and clinical relevance for an individual patient. Hematology Am Soc Hematol Educ Program. 2012;2012:137–142. [DOI] [PubMed] [Google Scholar]
- 16.Flanders A, Stetler-Stevenson M, Landgren O. Minimal residual disease testing in multiple myeloma by flow cytometry: major heterogeneity. Blood. 2013; 122(6):1088–1089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Paiva B, van Dongen JJM, Orfao A. New criteria for response assessment: role of minimal residual disease in multiple myeloma. Blood. 2015;125(20):3059–3068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rawstron AC, Gregory WM, de Tute RM, et al. Minimal residual disease in myeloma by flow cytometry: independent prediction of survival benefit per log reduction. Blood. 2015;125(12):1932–1935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rawstron AC, Böttcher S, Letestu R, et al. Improving efficiency and sensitivity: European Research Initiative in CLL (ERIC) update on the international harmonised approach for flow cytometric residual disease monitoring in CLL. Leukemia. 2013;27(1):142–149. [DOI] [PubMed] [Google Scholar]
- 20.Garnache Ottou F, Chandesris M-O, Lhermitte L, et al. Peripheral blood 8 colour flow cytometry monitoring of hairy cell leukaemia allows detection of high-risk patients. Br J Haematol. 2014;166(1):50–59. [DOI] [PubMed] [Google Scholar]
- 21.Böttcher S, Ritgen M, Buske S, et al. Minimal residual disease detection in mantle cell lymphoma: methods and significance of four-color flow cytometry compared to consensus IGH-polymerase chain reaction at initial staging and for follow-up examinations. Haematologica. 2008; 93(4):551–559. [DOI] [PubMed] [Google Scholar]
- 22.Van Dongen JJM, Lhermitte L, Böttcher S, et al. EuroFlow antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive and malignant leukocytes. Leukemia. 2012; 26(9):1908–1975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Neale GA, Coustan-Smith E, Pan Q, et al. Tandem application of flow cytometry and polymerase chain reaction for comprehensive detection of minimal residual disease in childhood acute lymphoblastic leukemia. Leukemia. 1999; 13(8):1221–1226. [DOI] [PubMed] [Google Scholar]
- 24.Borowitz MJ, Pullen DJ, Shuster JJ, et al. Minimal residual disease detection in childhood precursor-B-cell acute lymphoblastic leukemia: relation to other risk factors. A Children’s Oncology Group study. Leukemia. 2003;17(8):1566–1572. [DOI] [PubMed] [Google Scholar]
- 25.Campana D, Coustan-Smith E. Detection of minimal residual disease in acute leukemia by flow cytometry. Cytometry. 1999;38(4):139–152. [DOI] [PubMed] [Google Scholar]
- 26.Van der Vuurst de Vries AR, Clevers H, Logtenberg T, Meyaard L. Leukocyte-associated immunoglobulin-like receptor-1 (LAIR-1) is differentially expressed during human B cell differentiation and inhibits B cell receptor-mediated signaling. Eur J Immunol. 1999;29(10):3160–3167. [DOI] [PubMed] [Google Scholar]
- 27.Sánchez ML, Almeida J, Vidriales B, et al. Incidence of phenotypic aberrations in a series of 467 patients with B chronic lymphoproliferative disorders: basis for the design of specific four-color stainings to be used for minimal residual disease investigation. Leukemia. 2002;16(8):1460–1469. [DOI] [PubMed] [Google Scholar]
- 28.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–310. [PubMed] [Google Scholar]
- 29.Letestu R, Cartron G, Lepretre S, et al. Minimal residual disease (MRD) by 8-color flow cytometry (Flow-MRD) and IGH clonospecific quantitative PCR (ASO RQPCR) reached similar performances for evaluation of CLL treatment in a phase II clinical trial: cross validation of the methods. Hematol Oncol. 2014: abstract 3307 Presented at: ASH Annual Meeting, San Francisco, GA, USA, 6–9 December 2014. [Google Scholar]
- 30.Ladetto M, Brüggemann M, Monitillo L, et al. Next-generation sequencing and real-time quantitative PCR for minimal residual disease detection in B-cell disorders. Leukemia. 2014;28(6):1299–1307. [DOI] [PubMed] [Google Scholar]
- 31.Drandi D, Kubiczkova-Besse L, Ferrero S, et al. Minimal residual disease detection by Droplet digital PCR in multiple myeloma, mantle cell lymphoma, and follicular lymphoma: a comparison with real-time PCR. J Mol Diagn. 2015;17(6):652–660. [DOI] [PubMed] [Google Scholar]