

Abstract
Context:
Striae distensae are linear atrophic dermal scars covered with flat atrophic epidermis. They may cause disfigurement, especially in females. Many factors may cause striae distensae such as steroids, obesity, and pregnancy. Although there is no standard treatment for striae; many topical applications, peeling, and light and laser systems have been tried.
Aims:
To evaluate and compare the efficacy of fractional CO2 laser with intense pulse light in treating striae distensae.
Subjects and Methods:
Forty patients with striae distensae were recruited. Twenty of them were treated by fractional CO2 laser and 20 were treated with intense pulse light. Length and width of the largest striae were measured pre- and post-treatment. Patient satisfaction was also evaluated and graded. Patients were photographed after each treatment session and photos were examined by a blinded physician who had no knowledge about the cases.
Results:
Both groups showed significant improvement after treatments (P < 0.05). Patients treated with fractional CO2 laser showed significant improvement after the fifth session compared with those treated with ten sessions of intense pulsed light (P < 0.05) in all parameters except in the length of striae (P > 0.05).
Conclusions:
The current study has provided supportive evidence to the effectiveness of both fractional CO2 laser and intense pulse light as treatments for striae distensae. Fractional CO2 laser was found to be more effective in the treatment of striae distensae compared with intense pulse light.
Keywords: CO2 laser, intense pulse light, photothermolysis, striae distensae
What was known?
Striae distensae have no standard line of treatment in spite of many different treatment modalities.
Introduction
Striae distensae, also termed stretch marks, are linear atrophic dermal scars covered with flat atrophic epidermis.[1,2] They were clinically described hundreds of years ago and the first histological description appeared in the medical literature in 1889.[3]
Striae distensae are caused by many physiological conditions such as adolescent growth spurts and pregnancy. They may also be caused by various pathological conditions such as obesity, Cushing's or Marfan's syndromes, and long-term systemic or topical steroid use.[1,4,5] Genetic predisposition assumption has been supported by many evidences such as the occurrence of striae in twins and the association between striae and hereditary diseases of connective tissue as Marfan syndrome.[6,7] Moreover, there is a decreased expression of collagen and fibronectin in striae distensae tissue.[8]
Although striae distensae do not cause any significant medical problems, they can be of great concern regarding their psychological implications, especially for females because of the disfigurement they cause. The exact pathogenesis of striae is still controversial. However, it may be due to changes in the components of extracellular matrix including fibrillin, elastin, and collagen.[9] In the early stages of striae, there are sequential changes in elastolysis and mast cell degeneration. Elastic fibers are the primary target affected in striae, then the pathology extends to the other dermal components.[10] It has been proposed that a striatoxin damages the tissues in a toxic way which leads to striations.[11] Furthermore, striae distensae are diagnosed clinically by their appearance as atrophied lines which are erythematous in early lesions and skin colored or hypopigmented in old lesions. Investigations are not needed except if there is an internal cause such as Cushing's syndrome.[3]
Up till now, there is no standard treatment modality for striae distensae. Several treatment modalities have been tried. Topical tretinoin (0.1%) has been used with an improvement that may persist for almost a year after discontinuation of therapy.[12] Ash et al. have found that combinations of 20% glycolic acid and 0.05% tretinoin or 20% glycolic acid and 10% L-ascorbic acid can improve the appearance of striae distensae. These applications have been supposed to improve the epidermal and dermal thickness to approach that of the adjacent normal skin.[13] Various other topical treatments (Centella asiatica, hyaluronic acid, trichloroacetic acid peels, and oils)[14] and disk micro-needle therapy system[15] have been used for treatment.
In the last two decades, various types of light and laser systems have been used for the treatment of striae distensae with inconsistent findings. Intense pulsed light (IPL) was used to treat striae distensae with good results.[16] A previous study has demonstrated that IPL replaces dermal elastosis with neo-collagen.[17]
Of the various modalities used to treat striae distensae, lasers have recently become the most widely used alternative.[16] The 585-nm flashlamp-pumped pulsed-dye laser was used to treat early immature striae distensae with good results. It acts through dilatation of the blood vessels and increase in collagen deposition in early stages of striae.[18,19,20] Although the 308-nm XeCl laser failed to improve skin atrophy in striae distensae, its action resulted solely from the improvement of pigmentation.[21] The 1064-nm long-pulse neodymium-doped yttrium aluminum garnet laser was used to treat immature striae distensae with satisfactory results through remodeling of elastic and collagen fibers.[22]
Recently, fractional photothermolysis has been introduced as a newer, nonablative resurfacing laser technique. Ultimately, the necrotic debris is expelled and neo-collagenesis occurs.[23] Fractional photothermolysis has been approved for the treatment of many skin conditions such as wrinkles, postacne scars, postburn scars, and other conditions needing skin resurfacing.[23] It has been found that fractional CO2 laser improved texture and appearance of the mature, white striae distensae in skin Types I–IV in a Brazilian study on 15 females with old striae distensae.[24] Other recent studies showed satisfactory improvement in striae distensae after fractional CO2 thermolysis.[25] Kim et al. treated six females with striae alba using 1550-nm fractional photothermolysis laser. They evaluated the results by serial photographs, erythema index and melanin index tracking, skin elasticity, histologic examination, and the patients’ subjective satisfaction scores. They concluded that fractional photothermolysis can reduce SD by stimulating new collagen and elastic fiber synthesis.[26]
In the current study, we have evaluated and compared the efficacy of fractional CO2 laser and IPL in the treatment of striae distensae of variable causes in female patients.
Subjects and Methods
Forty female patients with striae distensae visiting the dermatology out-patient clinic at the Dermatology, Venereology and Andrology Department at Qina Faculty of Medicine, South Valley University, Egypt, were enrolled in this study. Patients were randomly divided into two groups. Each group included 20 patients. The study took place in the period from April 2011 to April 2013. Exclusion criteria included current pregnancy, steroid, retinoids or immunosuppressive drugs intake, history of keloid tendency, and history of striae treatment in the last 6 months. The protocol and informed consent were approved by our local Institutional Review Board. The study was designed as a prospective, case comparison study.
Treatment
A topical anesthetic cream was applied under occlusion for 60 min on the striae and washed off, then dried before treatment. The first 20 patients were treated with fractional 10.6 μm CO2 laser using (fractional CO2 ATL 250, advanced technology laser, China) at 40 mJ energy, pulse width 4 ms, and scanning area 10 mm × 10 mm. All the patients received monthly treatment for five sessions. The total treatment duration was 5 months for each patient. The other 20 patients were treated with IPL (GP Flash 1, CACI International, USA). Every patient was treated twice monthly for 5 months. Each patient received 10 treatments by the end of the treatment duration. We used the hand piece of skin rejuvenation treatment with band width 590 nm. The starting dose was 20 J/cm2 increased by 1 J/cm2/session to reach the maximum dose of 30 J/cm2.
Patients’ evaluation
Width and length of the largest striae were measured and photographs were taken (using high resolution digital identical camera settings “Sony, Tokyo, Japan”) in each patient before the beginning of treatment and 4 weeks after the last session of treatment. Patient satisfaction was rated into either none or less satisfied = 0 or satisfied = 1. Clinical improvement was evaluated by a study-blinded physician by measuring the length and width of the largest striae and comparing photographs before and 1 month after the last treatment. The criteria for photographs evaluation were as follow: (1= ≤50% improvement and 2= >50% improvement).
Statistical analysis
Data were analyzed using SPSS version 17 software (USA). Descriptive statistics: Mean, standard deviation, and percentages were calculated. Test of significances: Chi-square test was used to compare the difference in the distribution of frequencies among different groups. Mann–Whitney U-test was calculated to test the mean differences in continuous variables between groups for the un-paired data, while Wilcoxon signed rank test was used for the paired data (before vs. after treatment). A significant P value was considered when it is <0.05.
Results
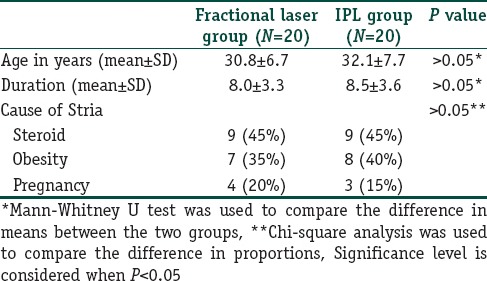
Forty patients were enrolled in the study. All the patients completed the treatment sessions. Patient ages ranged from 23 to 48 with a mean of 31.5 ± 7.2 years [Figure 1]. All the patients were females. The duration of striae ranged from 3 to 12 years with a mean of 8.22 ± 3.4 years. The causes of striae distensae were variable as shown in Figure 2. Side effects were mild in the study groups and included erythema, feeling of heat, pruritus, and one patient only showed marked hyperpigmentation [Table 1].
Figure 1.
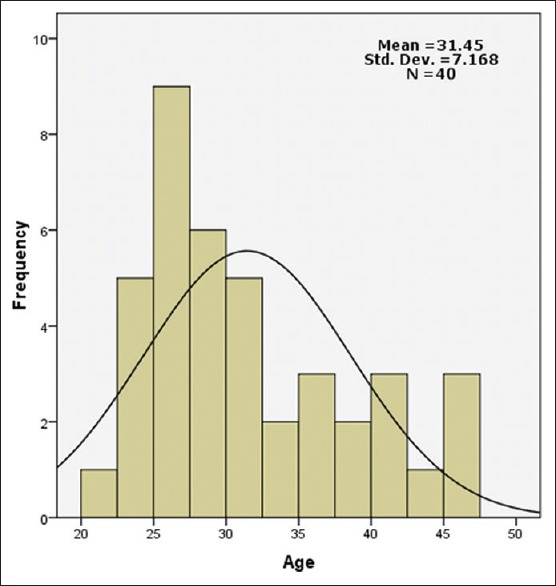
Age frequency of the studied sample
Figure 2.
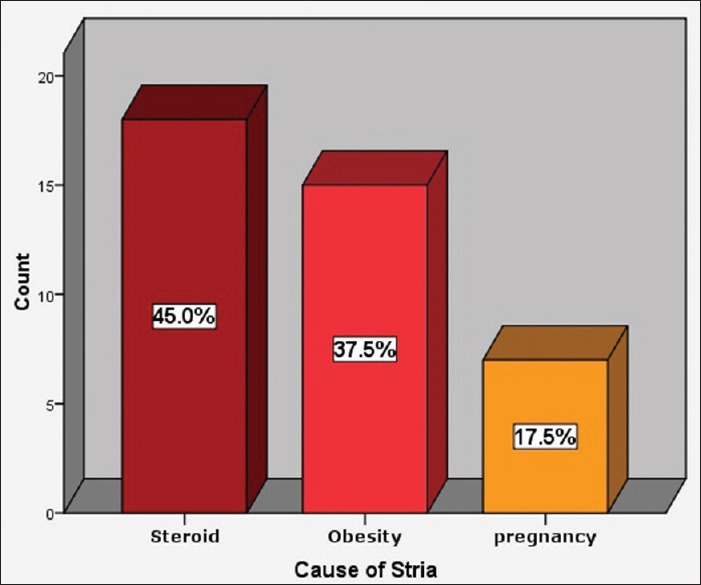
Distribution of the sample according to the stria etiology
Table 1.
Comparative analysis of the studied groups (cases vs. controls)
Width and length of striae
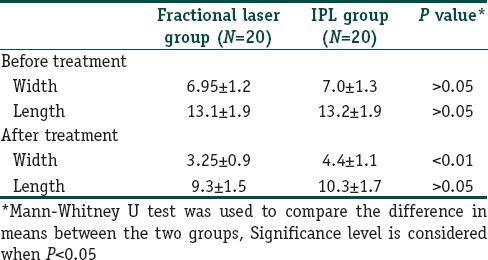
In the first group, the width of the largest striae varied between 5 and 9 mm at the start of study. The mean value of width was reduced from 6.95 to 3.25 1 month after the last treatment with high statistical significance (P < 0.001). The base line length of the largest striae varied from 11 to 16 cm. The mean length was reduced from 13.1 before the treatment to 9.3 as measured 1 month after the treatment with significant improvement (P < 0.001) [Table 2, Figures 3–6].
Table 2.
Change of Length and Width of Stria before and after treatment in each treatment group
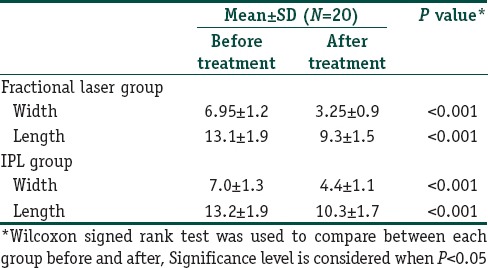
Figure 3.
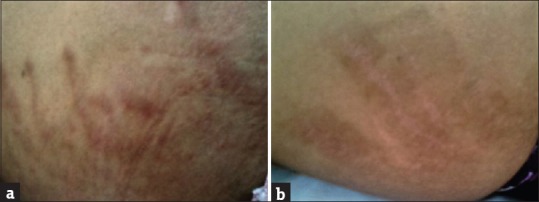
(a) A 31-year-old patient with extensive steroid-induced striae before CO2 fractional laser treatment. (b) A 31-year-old patient with extensive steroid-induced striae with good improvement after CO2 fractional laser treatment. The patient developed marked hyperpigmentation
Figure 6.
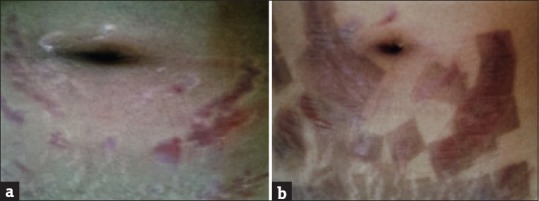
(a) A 22-year-old patient with obesity-induced striae in the abdomen before CO2 fractional laser treatment. (b) A 22-year-old patient with obesity-induced striae in the abdomen after CO2 fractional laser treatment
Figure 4.
(a) A female patient aged 26 years with extensive striae in the thigh before CO2 fractional laser treatment. (b) A female patient aged 26 years with extensive striae in the thigh showed marked improvement after CO2 fractional laser treatment
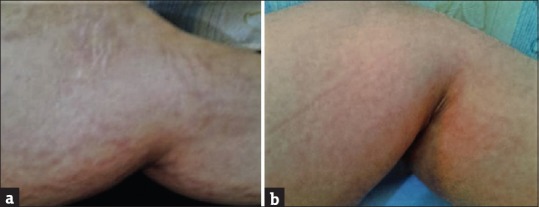
Figure 5.
(a) A 28-year-old patient with marked striae in the legs before CO2 fractional laser treatment. (b) A 28-year-old patient with marked striae in the legs showed marked improvement after CO2 fractional laser treatment
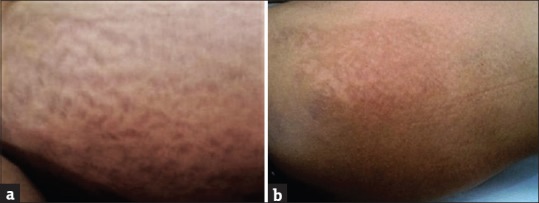
The IPL-treated patients’ baseline width of the largest striae varied from 4 to 9 mm [Figures 7 and 8]. The mean value of width was reduced from 7.0 to 4.4 mm 1 month after the last treatment which is statistically significant (P < 0.001). The baseline length of the largest striae varied from 10 to 16 cm. The mean length was reduced from 13.2 before the treatment to 10.3 as measured 1 month after the treatment with significant improvement (P < 0.005) [Table 2].
Figure 7.
(a) A 29-year-old patient with obesity-induced striae before intense pulsed light treatment. (b) A 29-year-old patient with obesity-induced striae showed moderate improvement after intense pulsed light treatment
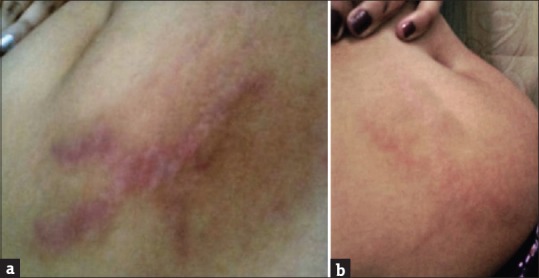
Figure 8.

(a) A 25-year-old patient with steroid-induced striae before intense pulsed light treatment. (b) A 25 years old patients with steroid-induced striae showed mild improvement after intense pulsed light treatment
By comparing both the treatment modalities, there was a significant difference in the improvement in striae width in those treated with laser than those treated with IPL (P < 0.005). There is no significant difference in the improvement of striae length in both study groups (P > 0.05) [Table 3].
Table 3.
Comparison between the two treatment strategy regarding change of Length and Width of Stria before and after treatment
Patient satisfaction
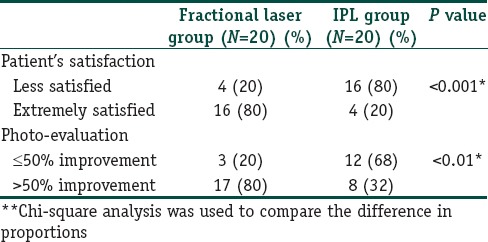
In the first group; 4 patients (20%) were none or less satisfied with the improvement, while 16 patients (80%) were satisfied with the results. In the second group, 16 patients (80%) were non or less satisfied by the results, while only 4 (20%) patients were satisfied. There is a significant difference between the two study groups regarding patient satisfaction (P < 0.005) [Table 4].
Table 4.
Comparative analysis of the studied groups regarding satisfaction and photo-evaluation
Photographic evaluation
By comparing the photographs before and 1 month after the treatments; 3 patients (20%) in the first group have been evaluated to have ≤50% improvement, while 17 patients (80%) have been evaluated to have improvement more than 50%. In the second group, 12 patients (68%) have been evaluated to have ≤50% improvement, while only 8 patients (32%) have been evaluated to have more than 50% improvement. There was a significant difference in the evaluation of photographs between the two study groups (P < 0.005) [Table 4].
Discussion
Striae distensae is a distressing cosmetic problem that has many causes such as obesity, steroids, and many other causes.[4,5,6,7,8] There are various treatment modalities for striae distensae such as topical tretinoin,[12] topical ascorbic acid,[13] topical glycolic acid,[13] and other topical treatments.[14] Other treatment options include: needling systems,[15] ultrasound, and radiofrequency.[27] The most recent treatment modalities are laser and light therapies.[16,17,28]
In this study, we evaluated and compared the efficacy of both CO2 fractional laser and IPL in the treatment of striae distensae of various causes in 40 female patients. Half of the patients were treated with fractional laser and the other half were treated with IPL.
In the fractional laser treated group, significant improvements in both length and width of striae, photographic evaluation, and patients’ satisfaction after the treatment have been assessed. The findings of the current study were consistent with previous research carried out to evaluate the efficacy of fractional CO2 laser on striae distensae. Naein and Soghrati compared the efficacy of fractional CO2 laser with a combination of 10% glycolic acid and 0.05% tretinoin cream in the treatment of striae alba in females. They treated 92 striae and they divided them into two groups. The first group was treated with five sessions of laser resurfacing every 2–4 weeks. The second group was treated with 10% glycolic acid +0.05% tretinoin cream nightly during the study. They found that fractional laser treatment was significantly more effective than medical treatment.[29]
Lee et al. treated 27 patients with striae distensae using an ablative 10,600-nm CO2 fractional laser. They treated 27 women with striae distensae in a single session with a CO2 fractional laser and used deep FX mode with a pulse energy of 10 mJ and a density of 2 (percent coverage of 10%). They found that it could be an effective method in treating striae distensae.[30] Shin et al. evaluated the effect of succinylated atelocollagen and ablative CO2 fractional laser in the treatment of striae distensae. They concluded that both ablative CO2 fractional laser and succinylated atelocollagen were effective treatments for striae distensae. They suggested that further studies are needed to prove this efficacy.[31] Cho et al. treated patients with striae alba by using the 10,600-nm CO2 fractional laser. They found a significant improvement of striae alba after the treatment.[32]
Our results also concur with previous studies that proved the efficacy of fractional photothermolysis by other photothermolysis devices. Katz et al. proved the efficacy of nonablative fractional photothermolysis in the treatment of striae rubra.[33] In addition, Bak et al. used fractional photothermolysis in the treatment of striae distensae in females. They concluded that fractional photothermolysis may be effective in treating striae distensae, without significant side effects. Treatment outcomes were better in patients with white rather than red striae.[34]
de Angelis et al., described the safety and efficacy results of treatment with a fractional nonablative 1540-nm erbium:glass laser in patients with Fitzpatrick skin Types II–IV for both striae rubra and striae alba. They detected positive safety and efficacy results with the fractional nonablative 1540-nm erbium:glass laser for the treatment of stria rubra and striae alba ranging in maturation age from 1 to 40 years in Fitzpatrick skin Types II–IV.[35] Guimarães et al., treated 10 female patients with striae distensae developed after breast augmentation by the use of nonablative fractionated 1550-nm erbium glass laser. They demonstrated excellent patient and plastic surgeon satisfaction after treatment. They supposed that the use of fractional photothermolysis is a good treatment modality for striae rubra.[36]
In the IPL-treated group, we found also a significant improvement in both length and width of striae distensae. Regarding the patient satisfaction and photographic evaluation, there was no significant improvement. These results agree with the previous reports which detected positive effects of IPL on striae distensae. Al-Dhalimi and Abo Nasyria compared two different wavelengths of IPL in the treatment of striae distensae. They treated 20 patients with striae by both wavelengths. Every site was treated with different wavelength every 2 weeks for five sessions. They found that both wavelengths were effective.[37]
Bedewi and Khalafawy used synchrotron infrared microspectroscopy to demonstrate the effect of IPL on dermal fibroblasts in patients with striae distensae. They found that IPL can treat striae through fibroblast stimulation which led to protein expression, especially collagen stimulation. They supposed that IPL is a promising therapeutic modality for striae with minimal side effects.[16]
In our knowledge, no previous work has compared the efficacy of fractional CO2 laser and IPL in the treatment of striae distensae. By comparing the two treatment modalities, we found a significant difference in all the study parameters except in the length of striae. Striae width showed a significant improvement in the group treated with CO2 fractional laser than the group treated with IPL in the same duration of treatment as evaluated by measurement, while no significant difference was noticed regarding the length of striae. Photographic evaluation showed a significant improvement in CO2 fractional laser treated patients than those treated with IPL. Patients treated with CO2 fractional laser were highly satisfied with their results as compared to those treated with IPL. Moreover, the CO2 fractional laser treated group was treated only with five treatment sessions, while the IPL-treated group was treated with 10 treatment sessions. Both groups showed minimal side effects.
Conclusion
We concluded that both fractional CO2 laser and IPL are effective treatment for striae distensae. Fractional CO2 laser is more effective than IPL in the same duration of treatment and with lesser treatment sessions. Both treatment modalities have little side effects. Larger sized studies are needed to corroborate this efficacy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
What is new?
Fractional CO2 Laser is an effective and safe treatment modality for striae distensae.
References
- 1.Cho S, Park ES, Lee DH, Li K, Chung JH. Clinical features and risk factors for striae distensae in Korean adolescents. J Eur Acad Dermatol Venereol. 2006;20:1108–13. doi: 10.1111/j.1468-3083.2006.01747.x. [DOI] [PubMed] [Google Scholar]
- 2.Atwal GS, Manku LK, Griffiths CE, Polson DW. Striae gravidarum in primiparae. Br J Dermatol. 2006;155:965–9. doi: 10.1111/j.1365-2133.2006.07427.x. [DOI] [PubMed] [Google Scholar]
- 3.Burrows NP, Lovell CR. Disorders of connective tissue. In: Burns T, Breathnach S, Cox N, Griffith C, editors. Rook's Textbook of Dermatology. 7th ed. Oxford: Blackwell Science; 2004. pp. 46–7. [Google Scholar]
- 4.Seguro LP, Rosario C, Shoenfeld Y. Long-term complications of past glucocorticoid use. Autoimmun Rev. 2013;12:629–32. doi: 10.1016/j.autrev.2012.12.002. [DOI] [PubMed] [Google Scholar]
- 5.Basile FV, Basile AV, Basile AR. Striae distensae after breast augmentation. Aesthetic Plast Surg. 2012;36:894–900. doi: 10.1007/s00266-012-9902-5. [DOI] [PubMed] [Google Scholar]
- 6.Di Lernia V, Bonci A, Cattania M, Bisighini G. Striae distensae (rubrae) in monozygotic twins. Pediatr Dermatol. 2001;18:261–2. doi: 10.1046/j.1525-1470.2001.018003261.x. [DOI] [PubMed] [Google Scholar]
- 7.Viennet C, Bride J, Cohen-Letessier A, Humbert P. Mechanical behavior of fibroblasts included in collagen lattices. J Soc Biol. 2001;195:427–30. [PubMed] [Google Scholar]
- 8.Lee KS, Rho YJ, Jang SI, Suh MH, Song JY. Decreased expression of collagen and fibronectin genes in striae distensae tissue. Clin Exp Dermatol. 1994;19:285–8. doi: 10.1111/j.1365-2230.1994.tb01196.x. [DOI] [PubMed] [Google Scholar]
- 9.Watson RE, Parry EJ, Humphries JD, Jones CJ, Polson DW, Kielty CM, et al. Fibrillin microfibrils are reduced in skin exhibiting striae distensae. Br J Dermatol. 1998;138:931–7. doi: 10.1046/j.1365-2133.1998.02257.x. [DOI] [PubMed] [Google Scholar]
- 10.Sheu HM, Yu HS, Chang CH. Mast cell degranulation and elastolysis in the early stage of striae distensae. J Cutan Pathol. 1991;18:410–6. doi: 10.1111/j.1600-0560.1991.tb01376.x. [DOI] [PubMed] [Google Scholar]
- 11.Kogoj F. Aetiology and pathogenesis of striae destinsae (article in German) Arch Dermatol Syphiliol. 1925;149:667. [Google Scholar]
- 12.Elson ML. Treatment of striae distensae with topical tretinoin. J Dermatol Surg Oncol. 1990;16:267–70. doi: 10.1111/j.1524-4725.1990.tb03962.x. [DOI] [PubMed] [Google Scholar]
- 13.Ash K, Lord J, Zukowski M, McDaniel DH. Comparison of topical therapy for striae alba (20% glycolic acid/0.05% tretinoin versus 20% glycolic acid/10% L-ascorbic acid) Dermatol Surg. 1998;24:849–56. doi: 10.1111/j.1524-4725.1998.tb04262.x. [DOI] [PubMed] [Google Scholar]
- 14.Elsaie ML, Baumann LS, Elsaaiee LT. Striae distensae (stretch marks) and different modalities of therapy: An update. Dermatol Surg. 2009;35:563–73. doi: 10.1111/j.1524-4725.2009.01094.x. [DOI] [PubMed] [Google Scholar]
- 15.Park KY, Kim HK, Kim SE, Kim BJ, Kim MN. Treatment of striae distensae using needling therapy: A pilot study. Dermatol Surg. 2012;38:1823–8. doi: 10.1111/j.1524-4725.2012.02552.x. [DOI] [PubMed] [Google Scholar]
- 16.Bedewi AE, Khalafawy GE. The use of synchrotron infrared microspectroscopy to demonstrate the effect of intense pulsed light on dermal fibroblasts. J Cosmet Laser Ther. 2013;15:305–9. doi: 10.3109/14764172.2013.769271. [DOI] [PubMed] [Google Scholar]
- 17.Hernández-Pérez E, Ibiett EV. Gross and microscopic findings in patients submitted to nonablative full-face resurfacing using intense pulsed light: A preliminary study. Dermatol Surg. 2002;28:651–5. doi: 10.1046/j.1524-4725.2002.02010.x. [DOI] [PubMed] [Google Scholar]
- 18.Karsai S, Roos S, Hammes S, Raulin C. Pulsed dye laser: What's new in non-vascular lesions? J Eur Acad Dermatol Venereol. 2007;21:877–90. doi: 10.1111/j.1468-3083.2007.02297.x. [DOI] [PubMed] [Google Scholar]
- 19.McDaniel DH, Ash K, Zukowski M. Treatment of stretch marks with the 585-nm flashlamp-pumped pulsed dye laser. Dermatol Surg. 1996;22:332–7. doi: 10.1111/j.1524-4725.1996.tb00326.x. [DOI] [PubMed] [Google Scholar]
- 20.Jiménez GP, Flores F, Berman B, Gunja-Smith Z. Treatment of striae rubra and striae alba with the 585-nm pulsed-dye laser. Dermatol Surg. 2003;29:362–5. doi: 10.1046/j.1524-4725.2003.29086.x. [DOI] [PubMed] [Google Scholar]
- 21.Goldberg DJ, Marmur ES, Hussain M. 308 nm excimer laser treatment of mature hypopigmentedstriae. Dermatol Surg. 2003;29:596–9. doi: 10.1046/j.1524-4725.2003.29144.x. [DOI] [PubMed] [Google Scholar]
- 22.Goldman A, Rossato F, Prati C. Stretch marks: Treatment using the 1,064-nm Nd: YAG laser. Dermatol Surg. 2008;34:686–91. doi: 10.1111/j.1524-4725.2008.34129.x. [DOI] [PubMed] [Google Scholar]
- 23.Wanner M, Tanzi EL, Alster TS. Fractional photothermolysis: Treatment of facial and nonfacial cutaneous photodamage with a 1,550-nm erbium-doped fiber laser. Dermatol Surg. 2007;33:23–8. doi: 10.1111/j.1524-4725.2007.33003.x. [DOI] [PubMed] [Google Scholar]
- 24.Macedo OR, Macedo O, Bussade M, Salgado A, Ribeiro M. Fractional photothermolysis for the treatment of striae distensae. JAAD. 2007;56((2) Supl 2):204. [Google Scholar]
- 25.Petro I. Fractional photothermolysis tackles striae distensae. Dermatol Times. 2007;28:94–6. [Google Scholar]
- 26.Kim BJ, Lee DH, Kim MN, Song KY, Cho WI, Lee CK, et al. Fractional photothermolysis for the treatment of striae distensae in Asian skin. Am J Clin Dermatol. 2008;9:33–7. doi: 10.2165/00128071-200809010-00003. [DOI] [PubMed] [Google Scholar]
- 27.Manuskiatti W, Boonthaweeyuwat E, Varothai S. Treatment of striae distensae with a TriPollar radiofrequency device: A pilot study. J Dermatolog Treat. 2009;20:359–64. doi: 10.3109/09546630903085278. [DOI] [PubMed] [Google Scholar]
- 28.Savas JA, Ledon JA, Franca K, Nouri K. Lasers and lights for the treatment of striae distensae. Lasers Med Sci. 2014;29:1735–43. doi: 10.1007/s10103-013-1342-1. [DOI] [PubMed] [Google Scholar]
- 29.Naein FF, Soghrati M. Fractional CO2 laser as an effective modality in treatment of striae alba in skin types III and IV. J Res Med Sci. 2012;17:928–33. [PMC free article] [PubMed] [Google Scholar]
- 30.Lee SE, Kim JH, Lee SJ, Lee JE, Kang JM, Kim YK, et al. Treatment of striae distensae using an ablative 10,600-nm carbon dioxide fractional laser: A retrospective review of 27 participants. Dermatol Surg. 2010;36:1683–90. doi: 10.1111/j.1524-4725.2010.01719.x. [DOI] [PubMed] [Google Scholar]
- 31.Shin JU, Roh MR, Rah DK, Ae NK, Suh H, Chung KY. The effect of succinylated atelocollagen and ablative fractional resurfacing laser on striae distensae. J Dermatolog Treat. 2011;22:113–21. doi: 10.3109/09546630903476902. [DOI] [PubMed] [Google Scholar]
- 32.Cho SB, Lee SJ, Lee JE, Kang JM, Kim YK, Oh SH. Treatment of striae alba using the 10,600-nm carbon dioxide fractional laser. J Cosmet Laser Ther. 2010;12:118–9. doi: 10.3109/14764171003706117. [DOI] [PubMed] [Google Scholar]
- 33.Katz TM, Goldberg LH, Friedman PM. Nonablative fractional photothermolysis for the treatment of striae rubra. Dermatol Surg. 2009;35:1430–3. doi: 10.1111/j.1524-4725.2009.01252.x. [DOI] [PubMed] [Google Scholar]
- 34.Bak H, Kim BJ, Lee WJ, Bang JS, Lee SY, Choi JH, et al. Treatment of striae distensae with fractional photothermolysis. Dermatol Surg. 2009;35:1215–20. doi: 10.1111/j.1524-4725.2009.01221.x. [DOI] [PubMed] [Google Scholar]
- 35.de Angelis F, Kolesnikova L, Renato F, Liguori G. Fractional nonablative 1540-nm laser treatment of striae distensae in Fitzpatrick skin types II to IV: Clinical and histological results. Aesthet Surg J. 2011;31:411–9. doi: 10.1177/1090820X11402493. [DOI] [PubMed] [Google Scholar]
- 36.Guimarães PA, Haddad A, Sabino Neto M, Lage FC, Ferreira LM. Striae distensae after breast augmentation: Treatment using the nonablative fractionated 1550-nm erbium glass laser. Plast Reconstr Surg. 2013;131:636–42. doi: 10.1097/PRS.0b013e31827c7010. [DOI] [PubMed] [Google Scholar]
- 37.Al-Dhalimi MA, Abo Nasyria AA. A comparative study of the effectiveness of intense pulsed light wavelengths (650 nm vs 590 nm) in the treatment of striae distensae. J Cosmet Laser Ther. 2013;15:120–5. doi: 10.3109/14764172.2012.748200. [DOI] [PubMed] [Google Scholar]