

Abstract
A concern during the early AIDS epidemic was the lack of a test to identify individuals who carried the virus. The first HIV antibody test, developed in 1985, was designed to screen blood products, not to diagnose AIDS. The first-generation assays detected IgG antibody and became positive 6 to 12 weeks postinfection. False-positive results occurred; thus, a two-test algorithm was developed using a Western blot or immunofluorescence test as a confirmatory procedure. The second-generation HIV test added recombinant antigens, and the third-generation HIV tests included IgM detection, reducing the test-negative window to approximately 3 weeks postinfection. Fourth- and fifth-generation HIV assays added p24 antigen detection to the screening assay, reducing the test-negative window to 11 to 14 days. A new algorithm addressed the fourth-generation assay's ability to detect both antibody and antigen and yet not differentiate between them. The fifth-generation HIV assay provides separate antigen and antibody results and will require yet another algorithm. HIV infection may now be detected approximately 2 weeks postexposure, with a reduced number of false-positive results.
INTRODUCTION
“I want to order the AIDS test on one of my patients.” So began a phone call I received in late 1985 from an oncologist. I explained that the human T cell lymphotropic virus type III (HTLV III) (the term HIV had not been adopted at that time) antibody assay that had just been developed was not a test for AIDS but was actually a test designed to prevent virus transmission via blood or blood products. The assay had not been FDA approved as a diagnostic test for AIDS (1). The oncologist went over my head to my department chairman in a futile attempt to have the “AIDS test” performed on his patient. Fast forward to 2016, and while we still do not have a specific AIDS test, diagnostic testing for HIV infection has evolved during the past 30 years. HIV infection now may be readily detected by laboratory assays, but AIDS is the late stage of HIV infection and requires both clinical and laboratory parameters for diagnosis (2). In this article, I provide a historical background of HIV testing, concluding with a description of the current generation of HIV diagnostic assays and the current testing algorithm.
First-generation HIV antibody tests.
Following the 1983 isolation and description of the virus associated with AIDS (3, 4), diagnostic tests were developed using separate HTLV III (Abbot and Electronucleonics) and lymphadenopathy virus (LAV) (Genetic Systems) isolates. These enzyme-linked immunosorbent assay (ELISA) and chemiluminescence methods used proteins isolated from virus-infected tissue cultures as antigenic targets. The assays detected IgG antibody to HIV-1 only. The tests were empirically sensitive but had an antibody-negative window of up to 12 weeks or more postinfection (5). The high sensitivity, while useful for protecting the blood supply, led to false-positive results, especially when low-risk individuals were tested. False-positive results were associated with infections, autoimmune disease, pregnancy, and unspecified conditions. Similarly to syphilis testing, a second level of testing was added to improve specificity. Two procedures were FDA cleared as confirmatory tests for HIV-1 antibody only: the Western blot assay (6) and an HTLV III immunofluorescence assay (IFA) (7, 8). Like the screening assays, each of these detected only IgG anti-HIV and had antibody-negative windows of 6 weeks or greater. A testing algorithm where reactive specimens were repeated in duplicate was developed. If one or both of the duplicates were reactive, the confirming procedure was performed. Only specimens that were repeatedly reactive in the screening test and reactive by the confirmatory test had a final interpretation as positive. Positive predictive value of a reactive HIV screening test could be less than 50% in low-risk populations (9). Clearly, there was a need for better tests that could be used for the diagnosis of HIV infection.
Second- and third-generation HIV tests.
Second-generation HIV tests, developed in the late 1980s, improved the specificity and thus the positive predictive value of the screening procedures by adding recombinant antigens, specifically HIV-1 p24, to the antigen milieu. Often manufacturers added an HIV-2 protein and an HIV-1 group O protein to the antigen preparation in order to detect antibodies to those viruses. HIV-2 and HIV-1 group O viruses are found primarily in West Africa but have been reported worldwide (10). These second-generation assays reduced the antibody-negative window to 4 to 6 weeks postinfection. Since these assays could detect HIV-2 antibody in addition to HIV-1 antibody, HIV-2 confirmatory testing was added to the algorithm (Fig. 1). The addition of IgM detection to the assay procedure resulted in the third-generation HIV test. While specific IgM detection had not been clinically useful, the IgG/IgM combination reduced the antibody-negative window to approximately 3 weeks postinfection (5). A p24 antigen detection ELISA, which detected the virus as early as 2 weeks postinfection, also could be performed. The overall testing algorithm remained the same, however, and repeatedly reactive screening results still were confirmed by a Western blot assay or an IFA. Inclusion of an HIV-2 protein in the antigen mixture added another level of testing to specimens repeatedly reactive in the screening test yet negative by the confirming procedure. Those specimens may have been positive for antibodies to HIV-2, which were not detected by the HIV-1 Western blot assay, or they may have been false positives. Thus, those specimens were then tested using an HIV-2-specific assay (Fig. 1). Quantitative and qualitative molecular assays could reduce the time from infection to detection even further; however, they were not cost-effective to be used for generalized screening. HIV PCR assays are recommended for neonatal diagnosis, however, as antibody assays may be positive in the neonate due to maternal IgG crossing the placenta (http://www.who.int/hiv/paediatric/EarlydiagnostictestingforHIVVer_Final_May07.pdf). In fact, the testing and HIV staging requirements for individuals <18 months of age differ from those recommended for adults (2).
FIG 1.

Centers for Disease Control/Food and Drug Administration algorithm for second-generation HIV tests (20). †, an immunofluorescence assay (IFA) for HIV-1 antibodies has recently been licensed by the Food and Drug Administration and can be used instead of the Western blot assay. Positive and negative IFA results should be interpreted in the same manner as similar results from Western blot tests. An indeterminate IFA result should first be tested by HIV-1 Western blot assay and then as indicated by the Western blot test results. §, perform HIV-2 EIA only if there is an identified risk factor for HIV-2 infection.
Fourth-generation HIV tests.
In the late 1990s, manufacturers developed HIV assays that combined antibody and antigen detection. As before, these were ELISA and chemiluminescence-based procedures. These tests reduced the test-negative window to approximately 2 weeks. While both antibody and antigen were detected in these procedures, the test gave only a single result and did not differentiate whether a positive result was due to the presence of the HIV-1 p24 antigen or due to the presence of antibody to HIV-1 or -2. While these tests had been used outside the United States for many years, the first fourth-generation procedure cleared by the FDA was the Abbot Architect method, which was approved in August 2010. Chavez et al. found that the Architect had a sensitivity of 99.94% and a repeat testing specificity of 99.5% in a cohort of 3,386 HIV-infected individuals, 7,551 uninfected subjects, and 58 patients with acute HIV infection (11). Bio-Rad's fourth-generation GS ELISA was FDA cleared in 2011. The GS ELISA was evaluated on 9,150 specimens and showed 100% sensitivity and 99.9 to 100% specificity (10). Siemen's ADVIA fourth-generation assay, to be used on the Centaur instrument, was approved in 2015. Siemen's package insert shows an antibody sensitivity of 100%, an antigen sensitivity of 97.87%, and a specificity of 99.69% (http://www.fda.gov/downloads/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/PremarketApprovalsPMAs/UCM450406.pdf).
When the fourth-generation HIV tests were adopted in the United States, a new testing algorithm was needed. Follow-up testing required both antigen and antibody detection. The Western blot assay, which has a 4- to 6-week antibody-negative window, may yield false negatives in patients with early infection who could be identified with a fourth-generation assay. Thus, the Western blot assay would be replaced by an HIV antibody differentiation assay. Initially, the CDC had proposed two separate fourth-generation testing algorithms: one for areas of low risk for HIV infection and one for areas of high risk. In 2014, however, a single algorithm was finalized (Fig. 2). The new algorithm followed the fourth-generation test with an HIV-1/2 differentiation procedure to determine whether the patient had antibodies to HIV-1 or HIV-2. Specimens that were repeatedly reactive by the fourth-generation assay and yet negative by the HIV-1/2 differentiation procedure were to be tested using an HIV-1 RNA qualitative PCR assay to determine if HIV-1 was present, causing a positive antigen result on the fourth-generation screening test. The molecular assay approved for this confirmation procedure is the Gen-Probe Aptima HIV-1 RNA assay. The current HIV viral load assays, while having improved sensitivity, have not been FDA approved for diagnostic use and are thus not recommended for use in this algorithm (S. Michele Owen, personal communication). Specimens that are negative by the molecular assay are considered to be false-positive screening results. The fourth-generation tests and algorithm have improved both sensitivity and specificity in detecting early HIV infection compared to those of the previous algorithm using the Western blot assay as the confirmatory procedure (12, 13) (Fig. 3).
FIG 2.
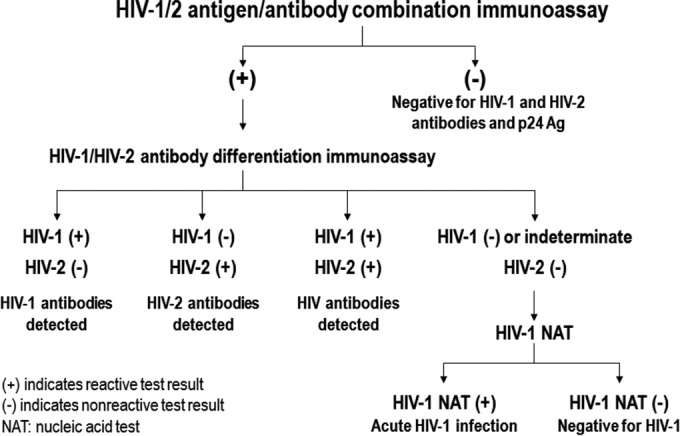
CDC algorithm for use with a fourth-generation HIV antibody/antigen screening test (21).
FIG 3.

Schematic representation of the 30-year evolution of HIV diagnostic assays.
Summa Health System's fourth-generation HIV testing experience.
Summa Akron City/St. Thomas Hospitals, located in Akron, OH, implemented the fourth-generation Abbott Architect HIV assay in December 2010. Prior to implementing the fourth-generation assay, Summa had been performing approximately 3,500 HIV screening tests per year. Approximately 20 specimens per year were repeatedly reactive, and 8 to 10 of those were confirmed as truly HIV positive, resulting in a positive predictive value of 40 to 50% in a typical year during the time we performed the third-generation HIV ELISA. Through 25 January 2016, our volume for the fourth-generation assay has remained approximately 3,500 specimens per year. We had 79 repeatedly reactive specimens over the 5 years we have been performing that procedure. Fifty-six specimens were confirmed by confirmatory testing as being positive for either antibody to HIV-1 (51 specimens) or viral nucleic acid (5 specimens). These values yield a positive predictive value of 70.8%. Thus, while our annual total positivity rate has dropped since we instituted the fourth-generation assay, our positive predictive value has increased, suggesting a reduced number of specimens being reported as false positive. We also detected five acute infections that may have been missed using the third-generation test and algorithm. Similar results for the Architect procedure were recently reported by Muthukumar et al. (14). Positive predictive values may be increased further by determining a different cutoff value appropriate for the population to be tested (15).
Fifth-generation HIV tests.
In 2015, the FDA approved the Bio-Rad BioPlex 2200 HIV Ag/Ab fifth-generation HIV screening test multiplex analysis method as a diagnostic assay. This test, like the fourth-generation procedures, detects both HIV antibody and the HIV-1 p24 antigen but provides separate results for each analyte. This assay will need a new algorithm, as there is no need for a supplemental HIV-1/2 differentiation assay for antibody-positive specimens because the test also provides separate results for HIV-1 and HIV-2 antibody. Specimens reactive only for the p24 antigen do not need an antibody confirming procedure, and specimens reactive only for antibody do not require an antigen confirmatory procedure. Salmona et al. evaluated the BioPlex fifth-generation assay and found 100% sensitivity and 99.5% specificity in a study of 1,505 patients (16). As of January 2016, the CDC has not published a fifth-generation testing algorithm.
Rapid HIV assays.
The advent of HIV prophylactic treatments following an occupational blood or body fluid exposure, as well as a need to be able to provide HIV results to patients in a clinic or emergency room or during labor and delivery, set the stage for manufacturers to develop rapid HIV assays. These card-based assays have gone through the same first through third generations as the main screening tests. Tests have been developed for whole blood, serum, and oral fluid. The OraQuick method is a third-generation HIV antibody assay which is FDA waived and has also been approved for home testing (http://www.fda.gov/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/PremarketApprovalsPMAs/ucm311895.htm). Overall, the rapid tests perform well.
The first HIV-1/2 antibody differentiation assay, the Bio-Rad Multispot procedure that is used in the fourth-generation algorithm (Fig. 2), was initially developed as a third-generation rapid test. Bio-Rad will cease to market the Multispot assay during 2016 and is replacing it with another rapid procedure, the Geenius HIV-1/2 semiautomated HIV-1/2 differentiation assay. Although the Geenius is a “rapid” assay, it is approved to be used only as a supplemental assay in the fourth-generation algorithm, not as a screening procedure. The Geenius has been reported to have a sensitivity of 100% and a specificity of 96% (17).
Currently there is a 4.5-generation rapid test, the Alere Determine HIV Ag-Ab Combo, which provides separate results for HIV antibody and antigen but does not differentiate HIV-1 antibody from HIV-2 antibody. Like the fifth-generation assay, this test would benefit from a different algorithm than has been developed for the fourth-generation tests. Faraoni et al. found this assay to have 100% specificity and positive predictive value with an overall sensitivity of 88.2% (18).
Social aspects of HIV testing.
A complete discussion of the societal aspects of HIV testing is beyond the scope of this article; however, no discussion of the evolution of HIV testing can be complete without noting the social stigma originally associated with HIV infection and testing, the issue of mandatory versus voluntary testing, the legal restrictions concerning release of HIV testing-related information, and the eventual acceptance of HIV testing as part of routine medical practice. Most cases of AIDS were initially described in male homosexuals and intravenous drug users. Although heterosexual and blood product transmission was also documented, just having an HIV test was often interpreted as an indication that the patient was a member of a high-risk group. Many states, including Ohio, where I practice, passed laws requiring specific informed consent for HIV testing, counseling before and after the test was performed, and limiting the disclosure of HIV test results. HIV test results were often not put into laboratory or hospital computer systems. Summa Health System, where I practice, did not put HIV results in the laboratory and hospital computer system until 2005. The CDC recommended, in 2006, that HIV testing become a routine procedure and that all adults be screened for the presence of HIV or antibody to HIV (19). This required amendments to many state laws. As of January 2016, 41 states have at least some law concerning HIV testing and/or counseling (http://www.cdc.gov/hiv/policies/law/states/index.html).
Conclusions.
HIV testing has evolved from being used as a method to safeguard the blood supply to being offered as a routine diagnostic test. The major deficiencies of early HIV tests have largely been overcome with the advent of the fourth- and fifth-generation assays. The test-negative window from infection to detection has been reduced, positive predictive values have improved, and tests are available in a variety of formats. Testing algorithms need to be updated continually to be used appropriately with newer assays. HIV testing has progressed to where infection can be detected approximately 2 weeks postexposure, with a reduced number of false-positive results compared to those seen with the early HIV assays (Fig. 3). Despite the improvements in HIV testing, the oncologist I mentioned above would not be satisfied. There remains no specific diagnostic test for AIDS.
ACKNOWLEDGMENTS
I thank Marcela Pasetti and Morgan Douglas for helpful discussions and assistance with figure preparation.
I have received speaker honoraria and travel assistance from Bio-Rad, Inc.
REFERENCES
- 1.Pear R. 1985. AIDS blood test to be available in 2 to 6 weeks. http://www.nytimes.com/1985/03/03/us/aids-blood-test-to-be-available-in-2-to-6-weeks.html Accessed 26 January 2016.
- 2.Selik RM, Mokotoff ED, Branson B, Owen SM, Whitmore S, Hall HI. 2014. Revised surveillance case definition for HIV infection—United States, 2014. MMWR Morb Recommend Rep 63(RR-03):1–10. [PubMed] [Google Scholar]
- 3.Gallo RC, Sarin PS, Gelmann EP, Robert-Guroff M, Richardson E, Kalyanaraman VS, Mann D, Sidhu GD, Stahl RE, Zolla-Pazner S, Leibowitch J, Popovic M. 1983. Isolation of human T-cell leukemia virus in acquired immune deficiency syndrome (AIDS). Science 220:865–867. doi: 10.1126/science.6601823. [DOI] [PubMed] [Google Scholar]
- 4.Barre-Sinoussi F, Chermann JC, Rey F, Nugeyre MT, Chamaret S, Gruest J, Dauguet C, Axler-Blin C, Vezinet-Brun F, Rouzioux C, Rozenbaum W, Montagnie L. 1983. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science 220:868–871. doi: 10.1126/science.6189183. [DOI] [PubMed] [Google Scholar]
- 5.Chappel RJ, Wilson KM, Dax EM. 2009. Immunoassays for the diagnosis of HIV: meeting future needs by enhancing the quality of testing. Future Microbiol 4:963–982. doi: 10.2217/fmb.09.77. [DOI] [PubMed] [Google Scholar]
- 6.Centers for Disease Control. 1989. Interpretation and use of the Western blot assay for serodiagnosis of human immunodeficiency virus type 1 infections. MMWR Morb Mortal Wkly Rep 38(Suppl 7):1–7. [PubMed] [Google Scholar]
- 7.Hedenskog M, Dewhurst S, Ludvigsen C, Sinangil F, Rodriguez L, Wu YT, Volsky DJ. 1986. Testing for antibodies to AIDS associated retrovirus (HTLV-III/LAV) by indirect fixed cell immunofluorescence: specificity, sensitivity and applications. J Med Virol 19:325–334. doi: 10.1002/jmv.1890190405. [DOI] [PubMed] [Google Scholar]
- 8.Imrie AA, Kehrer S, Smith GW, Penny R, Cooper DA. 1986. Seroimmunology of AIDS retrovirus infection. I. Use of immunofluorescence assay to confirm sera with ELISA reactivity. Pathology 18:438–443. [DOI] [PubMed] [Google Scholar]
- 9.Alexander TS, Lee J, Yen-Lieberman B. 1999. Incidence of human immunodeficiency virus antibody in a prenatal population at a community hospital. Clin Diagn Lab Immunol 6:140–141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bentsen C, McLaughlin L, Mitchell E, Ferrara C, Liska S, Myers R, Peel S, Swenson P, Gadelle S, Shriver MK. 2011. Performance evaluation of the Bio-Rad Laboratories GS HIV combo Ag/Ab EIA, a 4th generation HIV assay for the simultaneous detection of HIV p24 antigen and antibodies to HIV-1 (groups M and O) and HIV-2 in human serum or plasma. J Clin Virol 52S:S57–S61. doi: 10.1016/j.jcv.2011.09.023. [DOI] [PubMed] [Google Scholar]
- 11.Chavez P, Wesolowski L, Patel P, Delaney K, Owen SM. 2011. Evaluation of the performance of the Abbott Architect HIV Ag/Ab combo assay. J Clin Virol 52S:S51–S55. doi: 10.1016/j.jcv.2011.09.010. [DOI] [PubMed] [Google Scholar]
- 12.Geren K, Moore E, Tomlinson C, Hobohm D, Gardner A, Reardon-Maynard D, Gay C, Hightow-Weidman LB, Pandori MB, Moss N, Westheimer E, Tsoi B, Branson BM, Peters PJ. 2013. Detection of acute HIV infection in two evaluations of a new HIV diagnostic testing algorithm—United States, 2011-2013. MMWR Morb Mortal Wkly Rep 62:489–494. [PMC free article] [PubMed] [Google Scholar]
- 13.Cardenas AM, Baughan E, Hodinka R. 2013. Evaluation of the Bio-Rad Multispot HIV-1/HIV-2 rapid test as an alternative to Western blot for confirmation of HIV infection. J Clin Virol 58S:e97–e103. doi: 10.1016/j.jcv.2013.08.021. [DOI] [PubMed] [Google Scholar]
- 14.Muthukumar A, Alatoom A, Burns S, Ashmore J, Kim A, Emerson B, Bannister E, Ansari MQ. 2015. Comparison of 4th generation HIV antigen/antibody combination assay with 3rd generation HIV antibody assays for the occurrence of false-positive and false-negative results. Lab Med 46:84–89. doi: 10.1309/LMM3X37NSWUCMVRS. [DOI] [PubMed] [Google Scholar]
- 15.Kim S, Lee JH, Choi JY, Kim JM, Kim HS. 2010. False-positive rate of a “fourth-generation” HIV antigen/antibody combination assay in an area of low HIV prevalence. Clin Vaccine Immunol 17:1642–1644. doi: 10.1128/CVI.00258-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Salmona M, Delarue S, Delaugerre C, Simon F, Maylin S. 2014. Clinical evaluation of BioPlex 2200 HIV Ag-Ab, an automated screening method providing discrete detection of HIV-1 p24 antigen, HIV-1 antibody, and HIV-2 antibody. J Clin Microbiol 52:103–107. doi: 10.1128/JCM.02460-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Malloch L, Kadivar K, Putz J, Levett PN, Tang J, Hatchette TF, Kadkhoda K, Ng D, Ho J, Kim J. 2013. Comparative evaluation of the Bio-Rad Geenius HIV-1/2 confirmatory assay and the Bio-Rad Multispot HIV-1/2 rapid test as an alternative differentiation assay for CLSI M53 algorithm-I. J Clin Virol 58(Suppl 1):e85–e91. doi: 10.1016/j.jcv.2013.08.008. [DOI] [PubMed] [Google Scholar]
- 18.Faraoni S, Rochetti A, Gotta F, Ruggiero T, Orofino G, Bonoar S, Chisetti V. 2013. Evaluation of a rapid antigen and antibody combination test in acute HIV infection. J Clin Virol 57:84–87. doi: 10.1016/j.jcv.2013.01.007. [DOI] [PubMed] [Google Scholar]
- 19.Branson BM, Handsfield HH, Lampe MA, Janssen RA, Taylor AW, Lyss SB, Clark JE. 2006. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recommend Rep 55(RR-17):1–17. [PubMed] [Google Scholar]
- 20.O'Brien TR, George JR, Epstein JS, Homberg SD, Schochetman G. 1992. Testing for antibodies to human immunodeficiency virus type 2 in the United States. MMWR Recommend Rep 41(RR-12):1–9. [PubMed] [Google Scholar]
- 21.Centers for Disease Control and Prevention and Association of Public Health Laboratories. 27 June 2014. Laboratory testing for the diagnosis of HIV infection: updated recommendations. http://stacks.cdc.gov/view/cdc/23447 Accessed 26 January 2016.