
Figure 5. Circulating factors and intra-myocyte pathways leading to diaphragm abnormalities in heart failure.
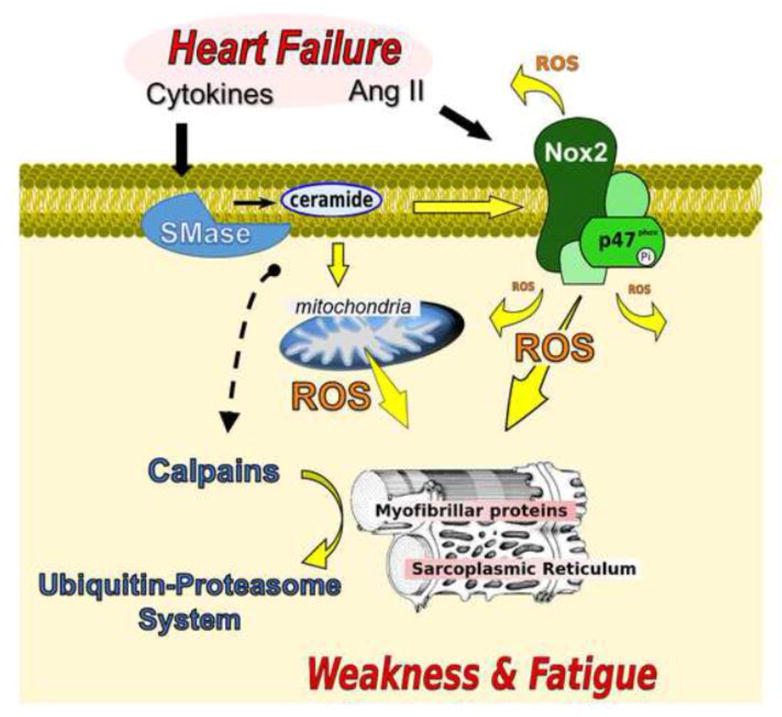
Angiotensin II (Ang II), sphingomyelinase (SMase), NAD(P)H oxidase 2 (Nox2), reactive oxygen species (ROS). Heart failure increases diaphragm neutral SMase activity and ceramide content [82]. SMase and ceramide cause diaphragm contractile dysfunction through ROS from mitochondria and Nox2 [142,144,143], and activation of calpain [140]. ROS play a causative role in diaphragm contractile dysfunction in heart failure [150,83,112]. Heart failure increases diaphragm calpain and proteasome activity [97,100], and proteasome inhibition blunts contractile dysfunction. Notably, ROS stimulates the ubiquitin-proteasome system [178,212].