
Figure 2.
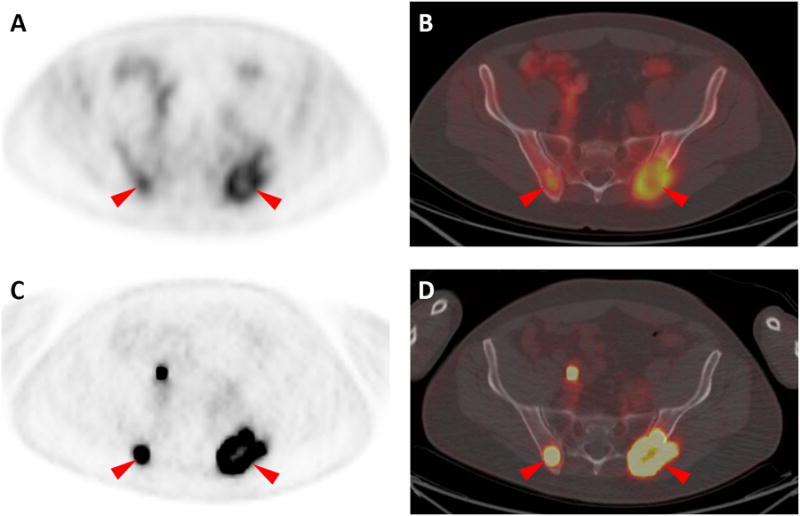
Large lytic lesions were present in the posterior aspects of both iliac bones in this patient, and both sites were found to have intense uptake of both radiotracers (18F-FDG in A and B and 18F-DCFPyL in C and D, red arrowheads). However, 18F-DCFPyL uptake was both visually and quantitatively higher than 18F-FDG. For the right iliac lesion, 18F-FDG uptake yielded SUVmax of 3.3, while for the same lesion 18F-DCFPyL uptake generated SUVmax of 16.6. For the left iliac, 18F-FDG SUVmax was 4.0 while 18F-DCFPyL SUVmax was 13.9. In aggregate, our findings in this patient with metastatic clear cell RCC are suggestive that 18F-DCFPyL may able to identify more lesions and has higher tumor uptake than 18F-FDG. Although a significant body of work has examined the role of 18F-DCFPyL and other small molecule inhibitors targeted against PSMA in the detection of prostate cancer [1-4], the use of such radiotracers for non-prostate applications has been limited to date [5, 6]. This is despite the fact that PSMA is highly expressed on the tumor neovasculature of many solid tumors, including RCC [7, 8]. Indeed, a previous case report has demonstrated the ability of a 68Ga-labeled small molecule inhibitor of PSMA (68Ga-PSMA) to identify sites of disease in a patient with metastatic clear cell RCC [5]. In that report, the authors noted concordance between 18F-FDG and 68Ga-PSMA uptake for all described lesions, though the 68Ga-PSMA PET acquisition was notable for improved lesion conspicuity. In combination with the earlier findings utilizing 68Ga-PSMA, this report confirms that further study with PSMA radiotracers in metastatic RCC is warranted.