

Abstract
Background.
Specific regions of the foot are responsible for the gait tasks of weight acceptance, single-limb support, and forward propulsion. With region foot pain, gait abnormalities may arise and affect the plantar pressure and force pattern utilized. Therefore, this study’s purpose was to evaluate plantar pressure and force pattern differences between adults with and without region-specific foot pain.
Methods.
Plantar pressure and force data were collected on Framingham Foot Study members while walking barefoot at a self-selected pace. Foot pain was evaluated by self-report and grouped by foot region (toe, forefoot, midfoot, or rearfoot) or regions (two or three or more regions) of pain. Unadjusted and adjusted linear regression with generalized estimating equations was used to determine associations between feet with and without foot pain.
Results.
Individuals with distal foot (forefoot or toes) pain had similar maximum vertical forces under the pain region, while those with proximal foot (rearfoot or midfoot) pain had different maximum vertical forces compared to those without regional foot pain (referent). During walking, there were significant differences in plantar loading and propulsion ranging from 2% to 4% between those with and without regional foot pain. Significant differences in normalized maximum vertical force and plantar pressure ranged from 5.3% to 12.4% and 3.4% to 24.1%, respectively, between those with and without regional foot pain.
Conclusions.
Associations of regional foot pain with plantar pressure and force were different by regions of pain. Region-specific foot pain was not uniformly associated with an increase or decrease in loading and pressure patterns regions of pain.
Key Words: Plantar heel pain, Arch pain, Idiopathic pain, Older adults, Gait analysis
Foot pain affects one in four adults (1) and is a leading cause of mobility limitations in older adults (2,3). Conservative treatment strategies of foot pain often include orthotics and shoewear modifications (4,5), with plantar pressure measurement (pedobarographic) systems used to objectively evaluate treatment process (5). Pedobarography allows the foot to be divided into regions, enabling clinicians, and researchers to evaluate pressures or forces within the specific region of interest. These systems provide a visual representation and quantification of high pressure (6) and high force (7) areas linked to foot dysfunction and injury.
With foot pain, however, it is unclear if it is (8,9) or is not (10) associated with plantar pressure differences, as pressures under the pain region have been shown to be increased (8), decreased (9), or unchanged (10) relative to those without pain. Moreover, not all foot pain is the same. Foot pain within specific regions, such as the forefoot or rearfoot, may influence whether or not static foot alignment differences exist with region-specific pain and it effects on the foot biomechanics during dynamic activities, such as walking, are unknown (11).
During walking three tasks occur: weight acceptance, single-limb support, and forward propulsion (12). In healthy gait, each of the four main regions of the foot—rearfoot, midfoot, forefoot, and toes—undertake an element of these tasks (13) (Figure 1). If an individual experiences foot pain in one or more of these regions, it can lead to gait compensatory strategies that alter foot and gait biomechanics, increasing risk of pain or injury elsewhere (6,14). Thus, understanding the effects of regional foot pain to foot biomechanical measures can provide insights into potential causes and effects of regional foot pain. Therefore, the purpose of this study was to evaluate cross-sectional associations of region-specific foot pain to foot biomechanical measures of plantar pressure and force in a population-based study of adults.
Figure 1.

Example of vertical ground reaction force (vGRF) showing gait tasks of weight acceptance, single-limb support, and forward propulsions. From initial contact (0% stance) to last contact (100% stance), the four foot regions contribute to the vGRF. Point ‘a’ is peak loading, and point ‘b’ is peak propulsion or peak unloading.
Methods
Participants
Participants included cohort members from the population-based Framingham Foot Study of older adults (15–17). Hebrew SeniorLife and Boston University Institutional Review Boards approved the Framingham Foot Study; all participants signed an informed consent prior to enrolment.
Analysis inclusion criteria were persons who had at least one foot with data regarding structural foot disorder, plantar pressure and force, and covariate information (age, gender, and body mass index); feet with amputated toes were excluded from the analyses.
Foot Biomechanical Measures
Participants walked barefoot at a self-selected pace across a Matscan system (40 frames per second, Tekscan, Boston, MA) using the two-step method. The two-step method involves participants stepping on the pressure mat on their second step and is as reliable as the midgait approach (18). There were two trials, one per foot.
Using Novel Automask software (Novel GmbH, Munich, Germany), Matscan data were masked into four regions: toes, forefoot, midfoot, and rearfoot (19). These computer-derived regions were evaluated against a single, trained evaluator who manually determined the foot regions, and interclass correlations ranged 0.96 (toes)–0.99 (midfoot). Peak pressure and maximum vertical forces were normalized by body mass.
Contributions of the four foot regions (ie, toes, forefoot, midfoot, and rearfoot) at peak vertical loading and propulsive force during stance phase were evaluated using a custom-made Matlab (The Mathworks, Natick, MA) script. This script extracted peak vertical ground reaction force under the foot during the loading and propulsive phases during gait.
Center of force (CoF) during the gait cycle was also extracted. Locations of CoF at initial contact, peak vertical loading, peak vertical propulsion, and last contact were normalized by the line of progression.
Foot Pain
Site-specific foot pain was assessed with participants selecting site(s) of each foot with pain, aching, or stiffness on most days (15). Site-specific areas included: nails, toes, forefoot, ball of the foot, arch, heel, and hindfoot, and were dichotomized to yes or no pain. These seven sites were collapsed into four regions: (i) toes—included toes and nails, (ii) forefoot—included forefoot and ball, (iii) midfoot—included the arch, and (iv) rearfoot—included heel and hindfoot.
Feet were grouped by foot pain region: (i) toe pain only (TPO); (ii) forefoot pain only (FPO); (iii) midfoot pain only (MPO); (iv) rearfoot pain only (RPO); (v) pain in two regions; (vi) pain in three or more regions; and (vii) no regional foot pain (referent).
Foot Disorders Assessment
Participants received a standardized, validated foot examination to screen for structural foot disorders (20). This examination recorded the presence or absence of structural foot disorders, including hallux valgus, hallux rigidus, hammer toes, claw toes, and overlapping toes.
Data Analysis
Mean and standard deviations were calculated for each region-specific foot pain group. Significant differences between pain groups and referent were determined using linear regression with generalized estimating equations (GEE) to account for correlations between participants’ two feet, or Fisher’s exact test, wherever appropriate.
A per-foot analysis using linear regression with GEE was used to determine associations of regional peak pressure and maximum vertical force during walking to region of foot pain. Adjusted models used covariates of age (21), weight (21), and gender (19) in all analyses. Presence of any structural foot disorder (yes/no) was included in midfoot models. Normalized maximum vertical forces and CoF were also evaluated using linear regression with GEE, with adjusted models using covariates of age (21,22), gender (19), and body mass index, with the presence of any structural foot disorders included only in midfoot models.
Inclusion of structural foot disorders as a dichotomized variable in only the midfoot model was determined through systematic model building. In this systematic model building, the structural foot disorders of hallux valgus, hallux rigidus, hammer toes, claw toes, overlapping toes, and hammer toes were evaluated individually at each foot region (ie, toes, forefoot, midfoot, rearfoot) to determine if estimates of effect changed by ≥15% (23). Each of the six individual structural foot disorders were considered confounders in only the midfoot region. A separate model using a variable of presence of any structural foot disorder (yes/no), as opposed to individual foot disorders, was also evaluated; it yielded similar results to individual variables. Because of model similarities between the individual foot disorders and the dichotomized structural foot disorder variable, the dichotomized presence of structural foot disorders was the adjustment variable.
Statistical analyses were conducted using SAS statistical analysis package, version 9.3 (SAS Institute, Cary, NC); alpha was p ≤ .05.
Results
There were 3,158 participants contributing 6,280 feet (missing data included 2 feet with amputated toes, 27 feet without foot biomechanics data, 4 feet without foot pain data, and 3 feet without foot disorder data). There were 1,520 feet (24.2%) with regional foot pain, with the forefoot the most common region (12.1%; Table 1). Participants with RPO were younger than those without regional foot pain (referent). Women were more likely than men to have TPO, FPO, and pain in two or three or more regions.
Table 1.
Participant Demographics.
| Total Population | No of Regional Foot Pain (Referent) | Toe Pain Only | Forefoot Pain Only | Midfoot Pain Only | Rearfoot Pain Only | Pain in Two Regions | Pain in Three or More Regions | |
|---|---|---|---|---|---|---|---|---|
| Number of Feet | 6,280 | 4,760 | 262 | 223 | 78 | 261 | 473 | 223 |
| Age, y | 66.2±10.5 | 66.3±10.4 | 68.0±11.9 | 65.9±9.7 | 64.1±10.1 | 64.3±9.7* | 66.3±11.2 | 66.0±11.2 |
| Women (%) | 3,525 (56.1) | 2,517 (52.9) | 171 (65.3)* | 167 (74.9)* | 40 (51.3) | 154 (59.0)* | 314 (66.4)* | 162 (72.7)* |
| Body mass index, kg/m2 | 28.4±5.5 | 28.1±5.2 | 28.1±5.8 | 29.8±5.8* | 29.2±5.6 | 29.9±5.9* | 29.8±6.4* | 30.0±6.2* |
| Structural foot disorder | ||||||||
| Hallux valgus (%) | 1,24 (27.5) | 1,225 (25.7) | 100 (38.2)* | 79 (35.4)* | 17 (21.8) | 62 (23.8) | 167 (35.3)* | 74 (33.2)* |
| Claw toes (%) | 106 (1.7) | 62 (1.3) | 12 (4.6) | 6 (2.7) | 0 | 9 (3.5) | 9 (1.9) | 8 (3.6) |
| Hammer toes (%) | 1,097 (17.5) | 772 (16.2) | 59 (22.5)* | 42 (18.8) | 20 (25.6)* | 38 (14.6) | 107 (22.6)* | 59 (26.5)* |
| Overlapping toes (%) | 377 (6.0) | 260 (5.5) | 26 (9.9)* | 12 (5.4) | 5 (6.4) | 20 (7.7)* | 34 (7.2) | 20 (9.0) |
| Hallux rigidus (%) | 232 (3.7) | 150 (3.2) | 12 (4.6) | 11 (4.9) | 0 | 3 (1.2) | 37 (7.8) | 19 (8.5) |
| Pain locations | ||||||||
| Toe region (%) | 669 (10.7) | — | 262 (100) | — | — | — | 255 (53.9) | 152 (68.2) |
| Nails (%) | 52 (0.8) | — | 22 (8.4) | — | — | — | 18 (3.8) | 12 (5.4) |
| Toes (%) | 633 (10.1) | — | 245 (93.5) | — | — | — | 238 (50.3) | 150 (67.3) |
| Forefoot region (%) | 762 (12.1) | — | — | 223 (100) | — | — | 328 (69.3) | 221 (94.6) |
| Forefoot (%) | 441 (7.0) | — | — | 124 (55.6) | — | — | 205 (43.3) | 112 (50.2) |
| Ball of foot (%) | 415 (6.6) | — | — | 110 (49.3) | — | — | 143 (30.2) | 162 (72.7) |
| Midfoot region (%) | 427 (6.8) | — | — | — | 78 (100) | — | 175 (37.0) | 174 (78.0) |
| Rearfoot region (%) | 627 (10.0) | — | — | — | — | 261 (100) | 188 (39.8) | 178 (79.8) |
| Heel (%) | 346 (5.5) | — | — | — | — | 120 (46.0) | 100 (21.1) | 126 (56.5) |
| Hindfoot (%) | 390 (6.2) | — | — | — | — | 177 (67.8) | 116 (24.5) | 97 (43.5) |
Notes: Data presented as mean ± standard deviation or N feet (%).
*Significantly different from referent (no regional pain group).
Associations of Regional Foot Pain and Plantar Peak Pressure
Feet with pain localized to one region (eg, TPO) displayed similar peak pressures in the pain region compared to the referent, except those with RPO (Figure 2), which had significantly lower rearfoot pressure (−6.1%).
Figure 2.

Differences in regional peak pressure and maximum vertical force by regions of pain, compared to referent (no regional foot pain). Lighter color denotes significantly higher pressure or force and darker color denotes significantly lower pressure or force relative to referent. Data were presented in Supplementary Tables 1 and 2.
Feet with TPO displayed similar toe and forefoot pressure as those without regional pain but showed significantly less midfoot (−7.0%) and rearfoot (−5.3%) peak pressure. Feet with FPO had, on average, 10.6% higher midfoot pressure relative to the referent with similar pressures in other regions. Toe pressure was 6.1% higher in those with MPO, while toe (5.8%) and rearfoot (6.1%) peak pressure was lower in those with RPO. Feet with two or three or more regions of pain showed significantly lower forces in the toes, forefoot, and rearfoot.
Associations of Regional Foot Pain and Maximum Vertical Force
Feet with TPO and FPO had similar maximum vertical force in the pain region, whereas those with MPO had higher maximum vertical force at the midfoot region and those with RPO had lower rearfoot maximum vertical force, compared to the referent.
Feet with TPO displayed lower (−6.6%) rearfoot maximum vertical force, but similar maximum vertical force at the other foot regions (Figure 3). Feet with FPO had a lower toe force (−11.8%) but higher midfoot (5.8%) and rearfoot (3.4%) forces. Those with MPO had high maximum vertical forces at the forefoot (3.0%) and midfoot (24.1%), while those with RPO displayed lower rearfoot (−5.1%) maximum vertical force.
Figure 3.
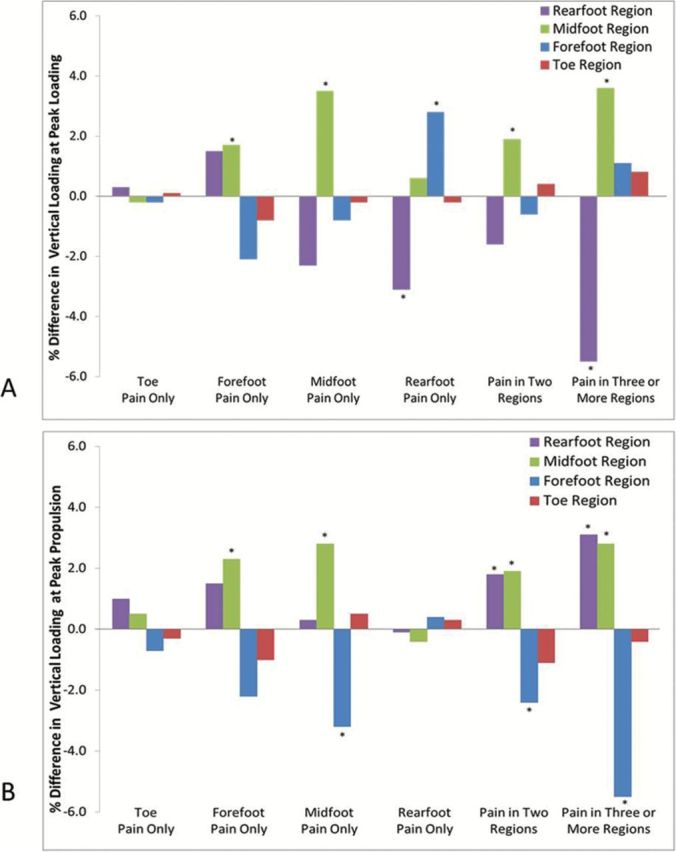
Percent differences in (A) peak vertical loading and (B) peak vertical propulsive force when walking, compared to the referent (no regional foot pain). *p < .05 denotes significant difference between pain group and referent. Data were presented in Supplementary Table 3.
Regional Foot Pain and Peak Vertical Loading Force
For individuals without regional foot pain, peak vertical loading occurred at 33.2±4.8% of the stance phase, which was similar to those with foot pain. CoF was similar between groups relative to the referent, except those with three or more regions of foot pain, where it was more distally located (Table 2).
Table 2.
Center of Force (CoF) Point as a Percent of Foot Length.
| Total Population | No of Regional Foot Pain (Referent) | Toe Pain Only | Forefoot Pain Only | Midfoot Pain Only | Rearfoot Pain Only | Pain in Two Regions | Pain in Three or More Regions | |
|---|---|---|---|---|---|---|---|---|
| Location of CoF at initial contact | 9.9±10.2 | 9.7±9.7 | 10.5±11.5 | 10.3±12.6 | 10.6±14.1 | 10.0±11.6 | 9.6±8.2 | 12.8±15.4* |
| Location of CoF at peak vertical loading | 38.3±8.5 | 38.2±8.4 | 38.1±8.3 | 37.6±8.5 | 39.2±8.9 | 39.1±8.4 | 38.7±8.8 | 40.5±9.8* |
| Location of CoF at peak vertical propulsion | 67.3±9.8 | 67.7±9.5 | 66.4±10.3 | 66.7±10.3 | 66.5±10.9 | 67.8±9.1 | 65.4±10.3* | 64.2±11.5* |
| Location of CoF at last contact | 91.0±8.4 | 91.1±7.9 | 90.9±8.9 | 90.3±11.3 | 89.1±15.2 | 91.1±9.4 | 90.8±6.9 | 89.0±12.7* |
| Distance of CoF from initial to last contact | 82.2±9.1 | 82.3±8.9 | 81.7±11.0 | 82.4±10.2 | 83.3±4.9 | 83.0±7.6 | 81.7±9.4 | 79.6±12.3* |
| Distance of CoF from peak vertical loading to peak vertical propulsion | 29.5±10.5 | 29.9±10.4 | 28.8±11.3 | 29.6±11.0 | 28.7±10.2 | 29.3±9.5 | 27.0±11.5* | 24.7±10.6* |
Note: Data presented as mean ± standard deviation.
*Significantly different from referent after adjustment (age, gender, and body mass index).
Individuals with RPO displayed significantly lower rearfoot force (3.1%) and higher forefoot force (2.8%) at peak vertical loading, relative to referent (Figure 2). People with MPO had a 3.5% higher midfoot force at peak vertical loading. Those with FPO displayed a higher midfoot force (1.8%) with a lower forefoot force (1.6) at the point of peak vertical loading. Individuals with two regions of foot pain or three or more regions of foot pain showed a 3.6% and 5.6% lower rearfoot force and a 1.8% and 2.4% higher midfoot force, respectively, at peak vertical loading.
Regional Foot Pain and Peak Vertical Propulsive Force
For individuals without regional foot pain, peak vertical propulsive force occurred at 68.7% ± 5.9% of the stance phase, which was statistically similar to those with RPO, MPO, FPO, and TPO. Individuals with two regions and three or more sites of foot pain had a significantly earlier peak vertical propulsive force at 67.3% ± 5.7% and 67.0% ± 5.3% of the stance phase, respectively. The CoF in feet with multiple regions of pain was more proximally placed at peak vertical propulsion compared to the referent. At the point of last contact, feet with three or more regions of pain had displayed a more proximal CoF location.
At peak vertical propulsion, individuals with RPO displayed higher forefoot force (3.1%; p = .046), while those with TPO had a lower forefoot force (−2.9%) at peak vertical propulsion. People with MPO had higher midfoot (2.7%) and forefoot (3.7%) forces, respectively, at peak vertical propulsion. Individuals with FPO exhibited 2.7% higher midfoot force with lower toe force (2.1%) at peak vertical propulsion. Individuals with two and three or more regions of foot pain showed a higher rearfoot force (2.8%; 3.6%) with lower forefoot (2.6%; 5.6%) and toe (3.1%; 2.1%) force, respectively, at peak vertical loading.
Discussion
The purpose of this cross-sectional, population-based study was to evaluate associations between foot biomechanical measures of plantar pressure and force to regional foot pain. We found significant differences in plantar pressure by region of foot pain. Feet with TPO, FPO, or MPO showed no differences in peak pressure under the pain region, but those with RPO had significantly lower pressure in this region. We also noted significant differences in maximum vertical force by region of foot pain. In feet with a single region of foot pain at the distal foot (toes or forefoot), maximum vertical force under the pain region was similar to referent. In contrast, in feet with a single foot pain region in the proximal foot (midfoot or rearfoot), maximum vertical forces were significantly different under the pain region. Feet with MPO had greater midfoot maximum vertical force, whereas those with RPO displayed lower pain maximum vertical force under the rearfoot relative to feet without regional pain. These results suggest that interventions for region-specific foot pain should not be uniform and that effects of region specific on gait and injury risk may differ.
The rearfoot’s common task is weight acceptance, and a mechanism for easing rearfoot pain is through reducing vertical ground reaction force and pressure (24). This theory aligns with our results as those with RPO reduced maximal force role in the rearfoot region, but it was only those with a single region of pain who may have adopted this strategy. Reductions as low as 3% in plantar pressure have been shown to decrease foot pain (25), and as individuals with RPO had a 6.1% lower plantar pressure, it may have been a gait strategy to lessen foot pain during gait. Mechanism for reducing the plantar pressures and forces are to (i) offload to another foot region (eg, midfoot, forefoot) or (ii) slow the gait speed to reduce rearfoot impact (21). At peak loading forefoot forces were increased while the rearfoot forces were lower, suggesting forces were offloaded to the forefoot. When combining this result that showed reduced pressure in the rearfoot and toes, it also suggest that gait speed was reduced (24). As gait was not monitored or controlled through this study, future work should evaluate how gait speed is affected by region-specific foot pain in order to evaluate its role as a compensatory mechanism.
Stability (26), single-limb support (26), and postural control (26,27) are the midfoot’s task. With foot pain, stability is reduced (2,3), and a mechanism to improve stability is to increase the contact area and force under the midfoot region (28) as well as to increase forefoot force (29) and toe pressure (30). Although we cannot address stability specifically, we did find that those with MPO displayed greater midfoot and forefoot force as well as greater toe pressure, suggesting that those with MPO utilize a gait strategy that improves stability. One limitation of the gait pattern of those with MPO may be that the atypical forces and pressures at the distal foot increase the risk of foot disorders (31). Given these relations of MPO, gait stability, and foot disorders, longitudinal research is needed to evaluate the role of MPO in fall risk and in the etiology of structural foot disorders.
The role of the forefoot and toes is to produce forward propulsion, with the forefoot contributing greater force than the toes (21) The differences between the contribution of the forefoot and toes to the vertical ground reaction force may explain the difference in foot biomechanical measures of those with FPO and TPO. In those with FPO or TPO, only those with FPO decreased vertical force. Those with FPO also increased pressure within the midfoot and increased forces within the midfoot and rearfoot regions, whereas those with TPO decreased force at the rearfoot and pressures at the rearfoot and midfoot. The forefoot contributes to forward propulsion (32), and dysfunction in this region results in forward propulsion offloaded to other force-producing areas of the foot, in line with our results showing greater force production in the midfoot and rearfoot with FPO (33). The toes, with the lower contribution of forward propulsion, do not offload but instead may reduce gait speed through a reduced propulsion force (21), which would explain reduced biomechanical measures of force and pressure rearfoot and midfoot.
Individuals with only one region of pain showed no difference in the CoF. The CoF can be indicative of ankle joint actions (34), and only feet with multiple regions of pain showed a shift in the CoF. Feet with two or three or more regions of pain shifted the CoF proximally. Proximal placement of the CoF during peak vertical propulsion as well as during last contact would tend to place the ankle in a position of reduced plantarflexion, relative to those without foot pain. Reduced ankle plantarflexion would lower gait speed (34) and reduce plantar pressure and forces (21), which would be in agreement to our results. In light to these findings, studies of foot pain should include evaluations of ankle function, foot function, and biomechanics.
Although we noted differences in plantar force and pressure in feet with regional foot pain compared to those without, the results of this study need to be interpreted in the context of its strengths and limitations. First, our analysis was a cross-sectional evaluation of foot biomechanics and regional foot pain, meaning causal relations cannot be inferred. Moreover, there was no severity of regional foot pain measurement, which if these data were included in the analyses may yield different results regarding plantar force and pressure patterns utilized in those with region-specific pain. Future work should evaluate the effects of pain severity to determine if regional plantar forces and pressures are increased, decreased, or similar with regard to severity. Second, while gait speed is known to affect plantar loading (21), gait speed was not controlled or evaluated in this study. However, when participants walk at a controlled speed, gait pattern disturbances occur (35), suggesting measurement of a typical step at self-selected speed may be more meaningful than that from a particular gait speed. Finally, this work found those with regional foot pain had differences in regional forces, normalized by body mass, during loading and propulsion ranging from 2% to 4%. Significant differences in normalized maximum vertical force and plantar pressure ranged from 3% to 24% between those with and without regional foot pain. Currently, there is no clinically meaningful difference for normalized plantar pressure or force during walking; however, changes in plantar pressure as low as 3% may affect gait and ulcer risk in patients with diabetes (25). These results are within the ranges noted by prior work in patients with diabetes, but further work elucidating clinically meaningful differences in normalized plantar pressure and force during gait are necessary to elucidate the clinical relevance between those with and without regional foot pain.
Strengths of this study include its participants, data collection, and analysis. The Framingham Foot Study is a large, well-described, population-based cohort of adults evaluating foot health, foot function, and pain (2,3,20), which improves generalizability relative to studies with a smaller sample size. Further, this analysis utilized GEE to enable inclusion of both feet, while adjusting for correlations between feet. The study characteristics, participants, and statistical modeling provide a novel means for understanding associations of regional foot pain to plantar pressures and forces during gait.
Conclusion
This is the first study to show regional foot pain is associated with specific plantar pressure and force differences. The results support biomechanical theory and clinical implications of region-specific foot pain, and they suggest that the treatment of foot pain may be dependent on the foot region involved and its role in gait. Moreover, as regional foot pain is associated with differences in plantar pressure and loading difference that may influence the gait pattern utilized, this cross-sectional study highlights the need for continued research into foot pain etiology, effects, and treatment strategies to reduce the disabling effect of foot pain. Prospective studies are needed to elucidate causes of regional foot pain in relation to plantar loading in order to understand their effects on gait and physical function. As aberrant foot forces and pressures, such as those that were noted with regional foot pain, may lead to aberrant joint actions or increased odds of pain throughout the kinetic chain or (eg, knee or hip) (36) understanding the compensatory mechanisms that with regional foot pain may be a key to reducing risk of joint pain elsewhere. Moreover, treatment strategies of regional foot pain that seeks to alleviate plantar pressure abnormalities of increased or decreased pressure to restore a more natural plantar pressure and gait pattern may provide a means for improved physical function and mobility for those with foot pain.
Supplementary Material
Supplementary material can be found at: http://biomedgerontology.oxfordjournals.org/
Funding
Funding for this project was provided by the NIH’s National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01-AR047853) and National Institute of Aging (T32-AG023480).
Conflict of Interest
None.
Supplementary Material
References
- 1. Thomas MJ, Roddy E, Zhang W, Menz HB, Hannan MT, Peat GM. The population prevalence of foot and ankle pain in middle and old age: a systematic review. Pain. 2011;152:2870–2880. 10.1016/j.pain.2011.09.019 [DOI] [PubMed] [Google Scholar]
- 2. Menz HB, Dufour AB, Casey VA, et al. Foot pain and mobility limitations in older adults: the Framingham Foot Study. J. Gerontol A Biol Sci Med Sci. 2013;68:1281–1285. 10.1093/gerona/glt048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Riskowski JL, Hagedorn TJ, Dufour AB, Hannan MT. Functional foot symmetry and its relation to lower extremity physical performance in older adults: the Framingham Foot Study. J Biomech. 2012;45:1796–1802. 10.1016/j.jbiomech.2012.04.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Riskowski J, Dufour AB, Hannan MT. Arthritis, foot pain and shoe wear: current musculoskeletal research on feet. Curr Opin Rheumatol. 2011;23:148–155. 10.1097/BOR.0b013e3283422cf5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Rao S, Riskowski JL, Hannan MT. Musculoskeletal conditions of the foot and ankle: assessments and treatment options. Best Pract Res Clin Rheumatol. 2012;26:345–368. 10.1016/j.berh.2012.05.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Woodburn J, Helliwell PS. Relation between heel position and the distribution of forefoot plantar pressures and skin callosities in rheumatoid arthritis. Ann Rheum Dis. 1996;55:806–810. 10.1136/ard.55.11.806 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Kernozek TW, Elfessi A, Sterriker S. Clinical and biomechanical risk factors of patients diagnosed with hallux valgus. J Am Podiatr Med Assoc. 2003;93:97–103. 10.7547/87507315-93-2-97 [DOI] [PubMed] [Google Scholar]
- 8. Bryant A, Tinley P, Singer K. Plantar pressure distribution in normal, hallux valgus and hallux limitus feet. The Foot. 1999;9:115–119. 10.1054/foot.1999.0538 [Google Scholar]
- 9. Kibler WB, Goldberg C, Chandler TJ. Functional biomechanical deficits in running athletes with plantar fasciitis. Am J Sports Med. 1991;19:66–71. 10.1177/036354659101900111 [DOI] [PubMed] [Google Scholar]
- 10. Liddle D, Rome K, Howe T. Vertical ground reaction forces in patients with unilateral plantar heel pain - a pilot study. Gait Posture. 2000;11:62–66. 10.1016/S0966-6362(99)00053-3 [DOI] [PubMed] [Google Scholar]
- 11. O’Duffy EK, Clunie GP, Gacinovic S, Edwards JC, Bomanji JB, Ell PJ. Foot pain: specific indications for scintigraphy. Rheumatology. 1998;37:442–447. [DOI] [PubMed] [Google Scholar]
- 12. Perry J. Gait Analysis: Normal and Pathological Function. Thorofare, NJ: Charles B. Slack; 1992. [Google Scholar]
- 13. Bruening DA, Cooney KM, Buczek FL, Richards JG. Measured and estimated ground reaction forces for multi-segment foot models. J Biomech. 2010;43:3222–3226. 10.1016/j.jbiomech.2010.08.003 [DOI] [PubMed] [Google Scholar]
- 14. van der Leeden M, Steultjens M, Dekker JH, Prins AP, Dekker J. Forefoot joint damage, pain and disability in rheumatoid arthritis patients with foot complaints: the role of plantar pressure and gait characteristics. Rheumatology (Oxford). 2006;45:465–469. 10.1093/rheumatology/kei186 [DOI] [PubMed] [Google Scholar]
- 15. Dufour AB, Broe KE, Nguyen US, et al. Foot pain: is current or past shoewear a factor? Arthritis Rheum. 2009;61:1352–1358. 10.1002/art.24733 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Dawber TR, Meadors GF, Moore FE., Jr Epidemiological approaches to heart disease: the Framingham Study. Am J Public Health Nations Health. 1951;41:279–281. 10.2105/AJPH.41.3.279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Feinleib M, Kannel WB, Garrison RJ, McNamara PM, Castelli WP. The Framingham Offspring Study. Design and preliminary data. Prev Med. 1975;4:518–525. 10.1016/0091-7435(75)90037-7 [DOI] [PubMed] [Google Scholar]
- 18. McPoil TG, Cornwall MW, Dupuis L, Cornwell M. Variability of plantar pressure data. A comparison of the two-step and midgait methods. J Am Podiatr Med Assoc. 1999;89:495–501. 10.7547/87507315-89-10-495 [DOI] [PubMed] [Google Scholar]
- 19. VanZant RS, McPoil TG, Cornwall MW. Symmetry of plantar pressures and vertical forces in healthy subjects during walking. J Am Podiatr Med Assoc. 2001;91:337–342. 10.7547/87507315-91-7-337 [DOI] [PubMed] [Google Scholar]
- 20. Hagedorn TJ, Dufour AB, Riskowski JL, et al. Foot disorders, foot posture, and foot function: the Framingham foot study. PLoS One. 2013;8:e74364. 10.1371/journal.pone.0074364 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Menz HB, Morris ME. Clinical determinants of plantar forces and pressures during walking in older people. Gait Posture. 2006;24:229–236. 10.1016/j.gaitpost.2005.09.002 [DOI] [PubMed] [Google Scholar]
- 22. Scott G, Menz HB, Newcombe L. Age-related differences in foot structure and function. Gait Posture. 2007;26:68–75. 10.1016/j.gaitpost.2006.07.009 [DOI] [PubMed] [Google Scholar]
- 23. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:17. 10.1186/1751-0473-3-17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Wearing SC, Smeathers JE, Urry SR. The effect of plantar fasciitis on vertical foot-ground reaction force. Clin Orthop Relat Res. 2003;409:175–185. 10.1097/01.blo.0000057989.41099.d8 [DOI] [PubMed] [Google Scholar]
- 25. Bus SA, Ulbrecht JS, Cavanagh PR. Pressure relief and load redistribution by custom-made insoles in diabetic patients with neuropathy and foot deformity. Clin. Biomech. 2004;19:629–638. 10.1016/j.clinbiomech.2004.02.010 [DOI] [PubMed] [Google Scholar]
- 26. Cote KP, Brunet ME, Gansneder BM, Shultz SJ. Effects of pronated and supinated foot postures on static and dynamic postural stability. J Athl Train. 2005;40:41–46. [PMC free article] [PubMed] [Google Scholar]
- 27. Soames RW. Foot pressure patterns during gait. J Biomed Eng. 1985;7:120–126. 10.1016/0141-5425(85)90040-8 [DOI] [PubMed] [Google Scholar]
- 28. Hertel J, Gay MR, Denegar CR. Differences in postural control during single-leg stance among healthy individuals with different foot types. J Athl Train. 2002;37:129–132. [PMC free article] [PubMed] [Google Scholar]
- 29. Tanaka T, Takeda H, Izumi T, Ino S, Ifukube T. Effects on the location of the centre of gravity and the foot pressure contribution to standing balance associated with ageing. Ergonomics. 1999;42:997–1010. 10.1080/001401399185261 [DOI] [PubMed] [Google Scholar]
- 30. Hughes J, Clark P, Klenerman L. The importance of the toes in walking. J Bone Joint Surg Br. 1990;72-B:245–251. [DOI] [PubMed] [Google Scholar]
- 31. Lavery LA, Armstrong DG, Wunderlich RP, Tredwell J, Boulton AJ. Predictive value of foot pressure assessment as part of a population-based diabetes disease management program. Diabetes Care. 2003;26:1069–1073. 10.2337/diacare.26.4.1069 [DOI] [PubMed] [Google Scholar]
- 32. Prince F, Corriveau H, Hébert R, Winter DA. Gait in the elderly. Gait Posture. 1997;5:128–135. 10.1016/S0966-6362(97)01118-1 [Google Scholar]
- 33. Allen MK, Cuddeford TJ, Glasoe WM, et al. Relationship between static mobility of the first ray and first ray, midfoot, and hindfoot motion during gait. Foot Ankle Int. 2004;25:391–396. [DOI] [PubMed] [Google Scholar]
- 34. Kerrigan DC, Todd MK, Della Croce U, Lipsitz LA, Collins JJ. Biomechanical gait alterations independent of speed in the healthy elderly: evidence for specific limiting impairments. Arch Phys Med Rehabil. 1998;79:317–322. 10.1016/S0003-9993(98)90013-2 [DOI] [PubMed] [Google Scholar]
- 35. Cavanagh PR, Ulbrecht JS. Clinical plantar pressure measurement in diabetes: rationale and methodology. The Foot. 1994;4:123–135. 10.1016/0958-2592(94)90017-5 [Google Scholar]
- 36. Riskowski JL, Dufour AB, Hagedorn TJ, Hillstrom HJ, Casey VA, Hannan MT. Associations of foot posture and function to lower extremity pain: results from a population-based foot study. Arthritis Care Res (Hoboken). 2013;65:1804–1812. 10.1002/acr.22049 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.