

Abstract
Contrast sparing devices have been slowly adopted into routine patient care. Randomized trial evidence of automated contrast injectors (ACIs) has not been analyzed to evaluate the true reduction in contrast volume during coronary angiography and intervention. It is thought that by reducing the amount of contrast exposure there will be a simultaneous reduction in the risk of CIN. Therefore, we sought to synthesize published evidence on contrast sparing devices, contrast volume and incidence of contrast-induced nephropathy (CIN). We searched Medline, The Cochrane Library, and ClinicalTrials.gov. Search criteria included ACIs compared to manual injection, contrast media volume and incidence of CIN. Data was extracted by two independent reviewers. Weighted mean difference of contrast volume was calculated using random effects models in RevMan 5.4.1 software to derive a summary estimate. A total of 79,694 patients from 10 studies were included (ACI arm n= 20,099; Manual injection arm n= 59,595). On average, ACIs reduced contrast volume delivery by 45 mL per case (p < 0.001, 95%CI: -54, -35). CIN incidence was significantly reduced by 15% with an odds ratio of 0.85 (p<0.001, 95%CI: 0.78, 0.93) for those utilizing ACIs compared to manual injection. In conclusion, ACIs in angiography significantly reduces the volume of contrast delivered to the patient and the incidence of CIN.
Keywords: automated contrast injectors, contrast volume, contrast induced nephropathy
Introduction
To date, several studies have compared manual injection to ACIs and have reported a reduction in contrast volume administered with use of ACIs.(1-7) Studies have varied in the reported reduction of contrast for diagnostic catheterization.(1-4, 6-9) Others also include the contrast volume utilized during percutaneous coronary intervention (PCI).(1-5, 7, 9) However, there is a significant gap in summarizing the evidence in the published literature. With several studies reporting varying results in the utilization of ACIs compared to manual injection a meta-analysis or systematic review of the current research is required. The sample size of several of the studies is small and the combined power of a meta-analysis may allow for a more powerful conclusion based on the evidence. Therefore, we conducted a meta-analysis examining the currently published evidence on the reduction of contrast volume and the possible reduction of contrast-induced nephropathy (CIN) by the utilization of ACIs compared to manual injection. Several studies report the effects of ACIs on the volume of contrast used during coronary angiography; fewer studies examine the effects of contrast volume on renal function. We hypothesized that 1) contrast sparing devices reduce total contrast volume utilized during diagnostic and interventional cases; and 2) through the reduction of contrast volume, CIN is also reduced.
Methods
We searched MEDLINE (through April 2013), ClinicalTrials.gov, and The Cochrane Library, for clinical trials comparing ACIs versus manual injection and whether contrast media volume and/or rates of CIN were reported. As of April, 2013, 62 potentially relevant articles were identified. We also did a manual search on cross-references which were included in this meta-analysis.
Key word MESH terms included “automated injection”, “manual injection”, “automated contrast injectors” and “ACIST” for the ACIST Injection System (ACIST™; ACIST Medical Systems, Eden Prairie, Minnesota). Studies were included if they compared the amount of contrast volume delivery between ACIs and manual manifold injection systems in patients undergoing diagnostic coronary angiography and/or ad hoc PCI. Exclusion criteria included the absence of a manual injection arm or failing to report delivered contrast volume. Data was abstracted following appropriate methods according to the Quality of Reporting of Meta-analysis statement.(10) Two authors (K.M. and H.K.) independently reviewed the articles and recorded information outcomes on spreadsheets. Study quality was assessed by Jadad criteria (Table 1).(11)
Table 1. Study Characteristics.
| Article | Reference Number | Intervention | N | Protocol | Enrollment criteria | Study Type | RCT | Jadad Score |
|---|---|---|---|---|---|---|---|---|
| Anne et al. 2004 | 6 | Automated Injection | 253 | Contrast injection with ACIST device | Catheterization and/or PCI | Prospective | + | 2 |
| Manual Injection | 200 | Manual contrast injection using stopcock-manifold system | ||||||
| Brosh et al. 2005 | 4 | Automated Injection | 117 | Contrast injection with ACIST device | Catheterization and angiography or PCI | + | 1 | |
| Manual Injection | 95 | Manual injection with hand syringe | ||||||
| Call et al. 2006 | 5 | Automated Injection | 377 | Automated contrast injection | Catheterization and PCI | Retrospective observational | 0 | 1 |
| Manual Injection | 1,798 | Manual injection with hand syringe | ||||||
| Chahoud et al. 2001 | 7 | Automated Injection | 47 | Contrast injection using 4Fr ACIST device | Catheterization and coronary arteriography | Prospective | + | 1 |
| Manual Injection | 49 | Manual injection with 4Fr catheter | ||||||
| Godley et al. 2012 | 16 | Automated Injection | 7,970 | Contrast injection using ACIST device | Catheterization and ad hoc PCI | Retrospective observational | 0 | 1 |
| Manual Injection | 5,137 | Manual injection | ||||||
| Gonzalez et al. 2010 | 11 | Automated Injection | 80 | Contrast injection using 4Fr catheter | Catheterization | Prospective | + | 1 |
| Manual Injection | 84 | Manual injection with 6Fr catheter | ||||||
| Gurm et al. 2013 | 8 | Automated Injection | 9,995 | Automated injection with ACIS; catheter size per operator preference | PCI | Propensity matching retrospective observational | 0 | 1 |
| Manual Injection | 50,889 | Manual injection; catheter size per operator preference | ||||||
| Hwang et al. 2013 | 12 | Automated Injection | 306 | Contrast injection using Avanta Fluid Management Injection System | Catheterization and ad hoc PCI | Prospective | + | 1 |
| Manual Injection | 1,052 | Manual injection with | ||||||
| Hou et al. 2010 | 9 | Automated Injection | 856 | Contrast injection using 4Fr ACIST device | Coronary angiography | Prospective | 0 | 0 |
| Manual Injection | 960 | Manual injection with 6Fr catheter | ||||||
| Khoukaz et al. 2001 | 10 | Automated Injection | 47 | Contrast injection using 4Fr ACIST device | Catheterization and coronary arteriography | Prospective | + | 1 |
| Manual Injection | 46 | Manual injection with 6Fr catheter |
Summary statistics were calculated using Cochrane Collaborative software, RevMan5.4.1 (Baltimore, M.D.). We tested for heterogeneity by using the I2 test.(12) Heterogeneity was observed in the diagnostic and diagnostic and ad hoc comparisons. Therefore a random effects model was used to account for the existing heterogeneity across the studies. Weighted mean difference (MD) and 95% confidence intervals (CI) were calculated for contrast volume delivered and fluoroscopy time. Methods for the calculation have been previously described.
Results
We retrieved 62 articles that report on cardiac catheterization, ACIs, prevention of CIN, the use of contrast in other diagnostic cardiac modalities including magnetic resonance imaging and angiography. Forty-two articles were excluded as they did not meet inclusion criteria or report on coronary angiography. Twenty studies were reviewed for more detailed information, and 10 withdrawn as they did not include a comparison arm or report on contrast volume (Figure 1). Jadad scores ranged between 0 and 2 (Table 2).
Figure 1. Selection of Studies.
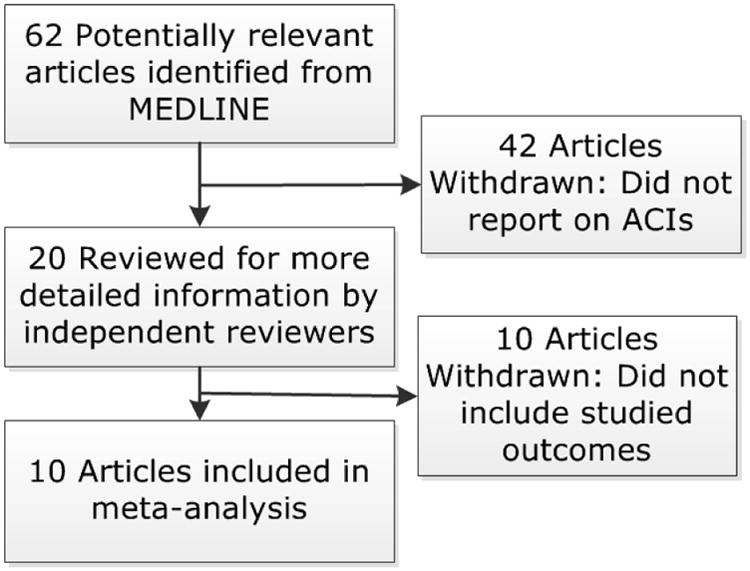
The figure flow diagram documents the flow of relevant study identification and the selection process for review and final inclusion in the meta-analysis.
Ten studies met our inclusion criteria and are included in this analysis (Table 2).(1-9, 13) A total of 79,694 patients were included: 20,099 patients in the ACI arm and 59,595 patients in the manual contrast injection arm. Demographics were similar among all studies and there were no gender related differences. Six studies were randomized controlled trials, 3 studies were retrospective cohorts, and one study divided patients based on the preference of the intervening cardiologist. Three different procedures were performed on patients including diagnostic coronary angiography, diagnostic angiography with ad hoc PCI, and PCI only (Figure 2).
Figure 2. Meta-analysis of Contrast Volume Use.
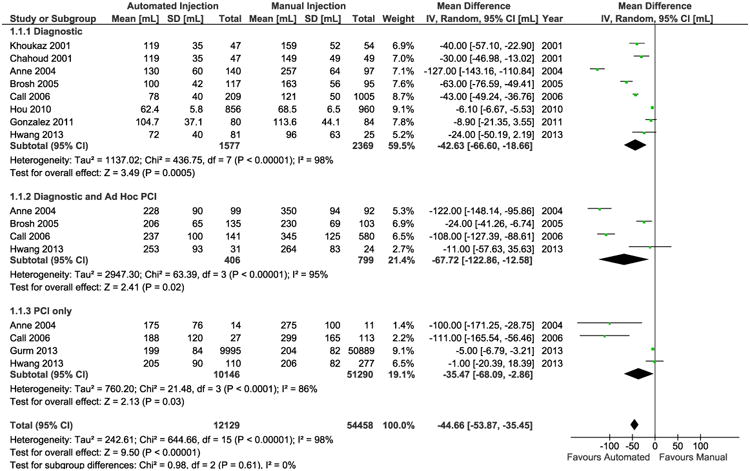
The forest plot graphs the weighted mean difference in contrast volume use between manual injection and ACIs devices stratified by type of procedure each with a sub-group summary estimate (black diamond) and a final summary estimate at the bottom for all types of procedure. The small boxes and horizontal lines depict the weighted mean difference for contrast volume for each listed study.
Overall, contrast volume was reduced by 45 ml (Figure 2) when using ACIs compared to manual injection. The incidence of CIN was reduced in the ACI group by 15% (Figure 3). ACIs resulted in a non-significant reduction in CIN in diagnostic coronary angiography and ad hoc PCI, and a non-significant reduction of in PCI alone.
Figure 3. Meta-analysis of Contrast-induced Nephropathy.
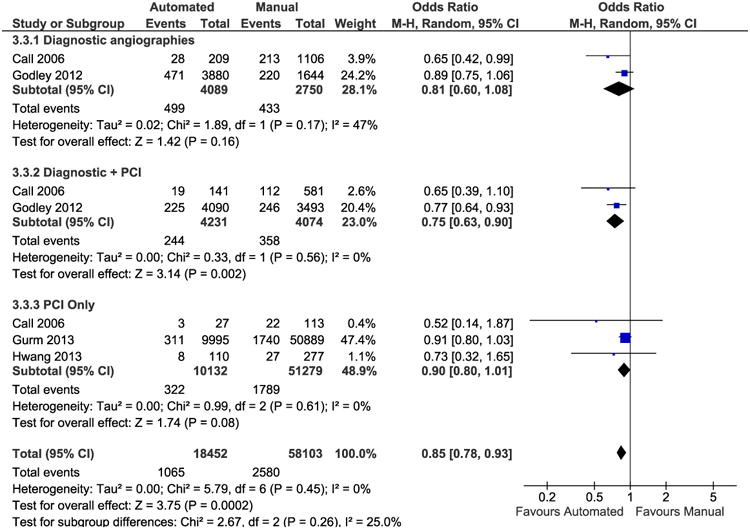
The forest plot graphs the odds ratios for CIN between manual injection and ACIs devices stratified by type of procedure each with a sub-group summary estimate (black diamond) and a final summary estimate at the bottom for all types of procedure. The small boxes and horizontal lines depict the odds ratio and 95% confidence intervals for CIN nephropathy for each listed study.
Discussion
We conducted a meta-analysis to evaluate contrast volume administered via ACI systems compared to manual injection. Overall, ACIs reduced contrast volume delivery by 45 ml and in reduced CIN by 15%.
ACIs have been reported to deliver less contrast volume during cardiac catheterization while maintaining image quality. It is likely that the reduction in contrast volume delivered using ACIs may reduce the patient's risk for CIN.(14-16) As shown by Call and colleagues there were 108 ml [-127, -89] less contrast used by ACIs with a 31.1% relative reduction in the incidence of CIN when ACIs were used for diagnostic catheterization and ad hoc PCI.(3) Incidence of CIN was reduced in the ACI group with an overall odds ratio of 0.85 (p<0.001, 95% CI: 0.78, 0.93, Figure 3). ACIs resulted in a non-significant reduction in CIN with an odds ratio of 0.81 (p =0.16, 95% CI, 0.60, 1.08) in diagnostic coronary angiography, a significant reduction of 0.75 (p<0.001, 95% CI, 0.63, 0.90) in diagnostic procedures and PCI, and a non-significant reduction of 0.90 ml (p = 0.08, 95% CI, 0.80, 1.01) in PCI only, when compared to a manual manifold. The precise pathophysiology has not been established, though contrast media-induced renal vasoconstriction, direct tubular toxicity, lipid peroxidation, and erythrocyte aggregation may be underlying mechanisms.(14)
Four studies compared outcomes based on catheter size; only one compared 4F catheters used in both arms, and 3 reported differences between 6F catheters used in manual manifold systems compared with 4F catheters used with ACIs.(4, 6-8) One study concluded no difference in the amount of contrast volume delivery, while 3 reported significantly less contrast volume use when using the 4F automated injection compared with manual technique.(4, 6, 7) Overall, 5.53 ml (p = 0.01, 95% CI, -9.91, -1.16) less contrast was delivered in the ACIST group compared to the manual group employing automated injectors for left ventriculography only. However, our meta-analysis does not have the ability to explore the causal role of catheter size on contrast volume or CIN endpoints.
There are some limitations to consider. First, the majority of the constituent patient population was derived from 2 studies; 1 study utilized retrospective data from patients that had received manual injection before ACIs had been employed at their hospital, thus the majority of the cohort was in the manual injection group.(5, 13) The other study does not report whether patients were randomized.(13) Larger populations give greater weight when employing a fixed effects model. Additionally, lack of randomization allows for methodological biases and confounding variables including the use of catheter size and biplane to reduce contrast use. Two studies are a continuation of each other, the only difference being 5 additional patients included in the manual injection group.(4, 7) However, after excluding the second study with 5 additional patients, we determined that there were still statistically significant lower volumes of contrast administered for diagnostic catheterizations. Second, the nature of the studies do not allow for equipoise or blinding; 2 studies report randomization techniques, 1 of which employed a faulty strategy, and none report withdrawal or dropout rates, creating an overall low Jadad score (Table 2). Despite lack of blinding we do not believe that study methodology affects the validity of this analysis.
Acknowledgments
The study was funded in part by grant number HS018443 from the Agency for Healthcare Research and Quality (Dr. Brown).
Footnotes
Disclosures: None
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Anne G, Gruberg L, Huber A, Nikolsky E, Grenadier E, Boulus M, Amikam S, Markiewicz W, Beyar R. Traditional versus automated injection contrast system in diagnostic and percutaneous coronary interventional procedures: comparison of the contrast volume delivered. J Invasive Cardiol. 2004;16:360–362. [PubMed] [Google Scholar]
- 2.Brosh D, Assali A, Vaknin-Assa H, Fuchs S, Teplitsky I, Shor N, Kornowski R. The ACIST power injection system reduces the amount of contrast media delivered to the patient, as well as fluoroscopy time, during diagnostic and interventional cardiac procedures. Int J Cardiovasc Intervent. 2005;7:183–187. doi: 10.1080/14628840500390812. [DOI] [PubMed] [Google Scholar]
- 3.Call J, Sacrinty M, Applegate R, Little W, Santos R, Baki T, Gandhi S, Kahl F, Kutcher M. Automated contrast injection in contemporary practice during cardiac catheterization and PCI: effects on contrast-induced nephropathy. J Invasive Cardiol. 2006;18:469–474. [PubMed] [Google Scholar]
- 4.Chahoud G, Khoukaz S, El-Shafei A, Azrak E, Bitar S, Kern MJ. Randomized comparison of coronary angiography using 4F catheters: 4F manual versus “Acisted” power injection technique. Catheter Cardiovasc Interv. 2001;53:221–224. doi: 10.1002/ccd.1152. [DOI] [PubMed] [Google Scholar]
- 5.Gurm HS, Smith D, Share D, Wohns D, Collins J, Madala M, Koneru S, Menees D, Chetcuti S. Impact of automated contrast injector systems on contrast use and contrast-associated complications in patients undergoing percutaneous coronary interventions. JACC Cardiovasc Interv. 2013;6:399–405. doi: 10.1016/j.jcin.2012.11.008. [DOI] [PubMed] [Google Scholar]
- 6.Hou L, Wei YD, Song J, Che WL, Peng WH, Wang Y, Li WM, Xu YW, Hu DY. Comparative study of 4Fr catheters using the ACIST variable rate injector system versus 6Fr catheters using hand manifold in diagnostic coronary angiography via transradial approach. Chin Med J (Engl) 2010;123:1373–1376. [PubMed] [Google Scholar]
- 7.Khoukaz S, Kern MJ, Bitar SR, Azrak E, Eisenhauer M, Wolford T, El-Shafei A. Coronary angiography using 4 Fr catheters with acisted power injection: A randomized comparison to 6 Fr manual technique and early ambulation. Catheter Cardiovasc Interv. 2001;52:393–398. doi: 10.1002/ccd.1088. [DOI] [PubMed] [Google Scholar]
- 8.Gonzalez MA, Ben-Dor I, Gaglia MA, Jr, Torguson R, Shimellis H, Bui A, Suddath WO, Pichard AD, Satler LF, Waksman R. Qualitative comparison of coronary angiograms between 4 French catheters with an advanced cardiovascular injection system and 6 French catheters with manual injection. Catheter Cardiovasc Interv. 2012;79:843–848. doi: 10.1002/ccd.23085. [DOI] [PubMed] [Google Scholar]
- 9.Hwang JR, D'Alfonso S, Kostuk WJ, Diamantouros P, Teefy P, Jablonsky G, Lavi S. Contrast volume use in manual vs automated contrast injection systems for diagnostic coronary angiography and percutaneous coronary interventions. Can J Cardiol. 2013;29:372–376. doi: 10.1016/j.cjca.2012.11.023. [DOI] [PubMed] [Google Scholar]
- 10.Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet. 1999;354:1896–1900. doi: 10.1016/s0140-6736(99)04149-5. [DOI] [PubMed] [Google Scholar]
- 11.Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17:1–12. doi: 10.1016/0197-2456(95)00134-4. [DOI] [PubMed] [Google Scholar]
- 12.Henry DA, Moxey AJ, Carless PA, O'Connell D, McClelland B, Henderson KM, Sly K, Laupacis A, Fergusson D. Anti-fibrinolytic use for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev. 2001:CD001886. doi: 10.1002/14651858.CD001886. [DOI] [PubMed] [Google Scholar]
- 13.Godley RW, 2nd, Joshi K, Breall JA. A comparison of the use of traditional hand injection versus automated contrast injectors during cardiac catheterization. J Invasive Cardiol. 2012;24:628–630. [PubMed] [Google Scholar]
- 14.Bartorelli AL, Marenzi G. Contrast-induced nephropathy. J Interv Cardiol. 2008;21:74–85. doi: 10.1111/j.1540-8183.2007.00318.x. [DOI] [PubMed] [Google Scholar]
- 15.Brown JR, Robb JF, Block CA, Schoolwerth AC, Kaplan AV, O'Connor GT, Solomon RJ, Malenka DJ. Does safe dosing of iodinated contrast prevent contrast-induced acute kidney injury? Circ Cardiovasc Interv. 2010;3:346–350. doi: 10.1161/CIRCINTERVENTIONS.109.910638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mehran R, Aymong ED, Nikolsky E, Lasic Z, Iakovou I, Fahy M, Mintz GS, Lansky AJ, Moses JW, Stone GW, Leon MB, Dangas G. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44:1393–1399. doi: 10.1016/j.jacc.2004.06.068. [DOI] [PubMed] [Google Scholar]