

Abbreviations
- CT
computed tomography
- MRI
magnetic resonance imaging
- TCS
tethered cord syndrome
A1‐year‐old female neutered English Cocker Spaniel was presented with a 9 months history of progressive right pelvic limb lameness. Survey radiographs, computed tomography (CT), magnetic resonance imaging (MRI), and joint taps of the pelvis, stifles, hock joints and tarsi, performed before referral, were within normal limits. Medical management with meloxicam did not result in clinical improvement. Treatment with gabapentin, initiated 7 days before presentation, resulted in improvement. General physical examination did not reveal any abnormalities. Neurological examination revealed paraparesis, right pelvic limb lameness, a low tail carriage, proprioceptive deficits expressed by delayed hopping, but intact paw placement in both pelvic limbs, a reduced withdrawal reflex in the right pelvic limb and decreased tail tone. Pain was elicited on lumbosacral palpation, dorsal extension of the tail and extension of both hips. The remainder of the neurological examination was within normal limits. Her neurological lesion was localized to the L4‐S3 spinal cord segments. A complete blood count and biochemistry panel were within normal limits. After premedication with methadone (0.2 mg/kg IM) and acepromazine (0.0 1mg/kg IM), anesthesia was induced with propofol (4–6 mg/kg, IV), and maintained with sevoflurane in oxygen. MRI1 of the lumbar and lumbosacral vertebral column was performed with the dog in dorsal recumbency with flexed limbs (ie, frog‐leg position). The imaging protocol included sagittal and transverse plane T2‐weighted (repetition time (ms) (TR), echo time (ms) (TE), 3000/120), sagittal and dorsal plane T2‐weighted short‐tau inversion recovery (TR/TE, 3612/80), and transverse plane T2‐weighted BAL TGRAD (TR/TE, 7.9/3.9) sequences. Sagittal and transverse plane T1‐weighted (T1W TSE) (TR/TE, 400/8) images were acquired before and after IV injection with gadolinium contrast.2 MRI demonstrated possible caudodorsal displacement of the conus medullaris. Mild lumbosacral intervertebral disk protrusion was also seen (Fig 1). After MRI, a CT examination of the lumbosacral vertebral column was performed using a 16‐slice scanner.3 After completion of the transverse CT study, sagittal and dorsal reconstructions were made. CT imaging (Fig 2) confirmed the MRI findings and did not reveal any other vertebral or spinal abnormalities. Differential diagnoses included tethered cord syndrome and dynamic lumbosacral vertebral canal stenosis. Given her initial positive response, medical management was continued with gabapentin (10mg/kg, q8h, PO), carprofen (2mg/kg, q12h, PO) and restricted exercise for 4 weeks. A re‐examination 4 weeks later demonstrated progression of her clinical signs characterized by more pronounced paraparesis and right pelvic limb lameness. General anesthesia was induced and maintained with the aforementioned protocol. A standard dorsal lumbosacral laminectomy, from L7 to S2 was performed. After opening the vertebral canal, a ligamentous structure was identified between the conus medullaris and the dorsal lamina of S2, which caused caudodorsal displacement and traction of the conus medullaris (Fig 3A,B). After sectioning and sampling the distal aspect of this ligamentous structure, the conus medullaris regained a more cranial position. The wound was closed routinely. Intraoperative analgesia was provided with ketamine (loading dose of 0.5 mg/kg IV followed by a CRI at 10 μg/kg/min IV) and methadone (0.1 mg/kg q4h, IV). Postoperative analgesia consisted of a combination of methadone (0.2 mg/kg, q4h, IV), carprofen (2 mg/kg, q12h, PO) and gabapentin (10 mg/kg, q8h, PO). The dog was discharged from hospitalization 4 days after surgery. The owner was advised to provide strict rest for 4 weeks in combination with gabapentin and carprofen for 2 more weeks. Histopathological evaluation revealed a combination of elastin and collagen fibers in parallel arrangement, confirming the ligamentous nature of the sampled tissue (Fig 3C). The surgical‐ and histopathological findings were considered diagnostic for tethered cord syndrome associated with a thickened and shortened filum terminale. A neurological examination 4 weeks after surgery revealed marked clinical improvement. At this time, the dog demonstrated mild lameness and proprioceptive deficits in the right pelvic limb. A neurological examination 10 weeks after surgery did not reveal any abnormalities. A telephone interview with the owner and referring veterinary surgeon 8 months after surgery revealed that the dog was free of clinical signs.
Figure 1.
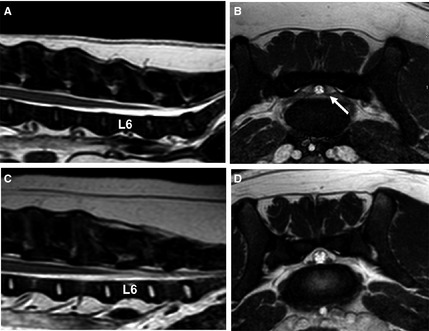
T2‐weighted sagittal image of the lumbosacral region (A) and transverse BAL TGRAD image at the level of L7‐S1 (B) demonstrating possible caudodorsal displacement of the conus medullaris. (A) The conus medullaris extends until the cranial aspect of L7. (B) The dural sac is located dorsally against the lamina of S1. T2‐weighted sagittal image of the lumbosacral region (C) and transverse BAL TGRAD image at the level of L7‐S1 (D) in a 1.5‐year‐old male English Cocker Spaniel without a spinal problem. (C) The conus medullaris terminates at the cranial aspect of L6. (D) The dural sac lies on the floor of the vertebral canal.
Figure 2.
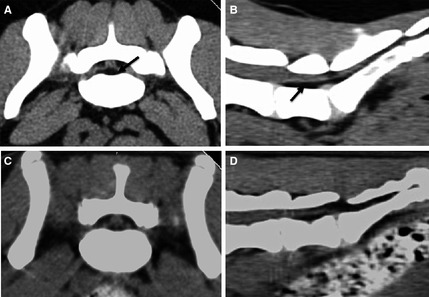
Transverse CT image at the level of the lumbosacral joint (A) and a sagittal reconstructed CT image (B) demonstrating possible caudodorsal displacement of the conus medullaris. Hypodense signal suggestive of epidural fat can be seen ventral from the conus medullaris (arrow). Transverse CT image (C) at the level of the lumbosacral joint and a sagittal reconstructed CT image (D) of a neurologically normal 1‐year‐old male English Cocker Spaniel for comparison.
Figure 3.
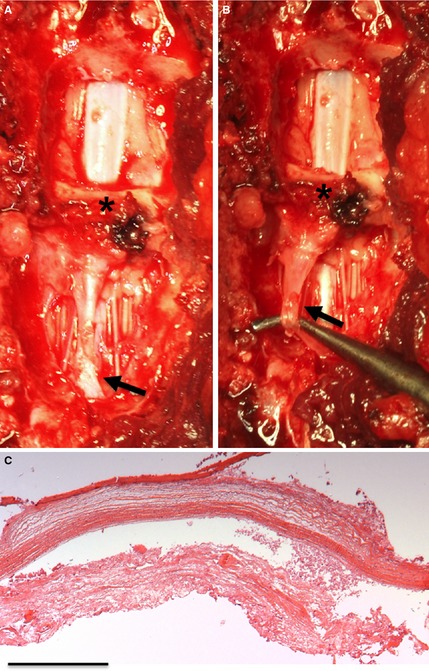
(A, B) Intraoperative pictures demonstrating caudal traction of the conus medullaris associated with a thickened filum terminale (arrow). Other intraoperative abnormalities included moderate hypertrophy of the ligamentum flavum (asterisk). (C) Histopathological evaluation (HE staining) demonstrated a combination of elastin and collagen fibers in parallel arrangement. × 40 Bar: 0.5 mm.
Tethered cord syndrome (TCS) represents a spectrum of congenital anomalies characterized by an abnormal caudal position and traction of the conus medullaris.1, 2 It can be associated with a variety of spinal malformations, including fatty infiltration of the filum terminale and open and closed forms of spinal dysraphism.3 TCS can, however, also be associated with an abnormally thickened, inelastic, and shortened filum terminale without other spinal or vertebral malformations.3 In people, this is also referred to as true or primary TCS.1, 4 In the case presented here, no other spinal or vertebral malformations were present and caudal traction of the conus medullaris was most likely caused by an abnormally thickened, inelastic, and shortened filum terminale. Although reported in conjunction with an intradural lipoma, myelomeningocele, spina bifida, myeloschisis, and a split cord malformation5, 6, 7, 8, 9, this case report, to the best of the authors' knowledge, represents the first veterinary report of TCS associated with a thickened filum terminale. The conus medullaris is the tapered ending of the spinal cord and is continued by a filament, the filum terminale. The filum terminale extends caudally and attaches to a sacral or caudal vertebra.10 Thickening of the filum terminale and subsequent TCS results from abnormal embryological development of the filum terminale during the process of retrogressive differentiation.2 The process of neurulation is not responsible for formation of the entire spinal cord. Distal to the caudal neuropore, undifferentiated cells form the caudal cell mass. This structure will proliferate, canalize, fuse with the neural tube and will eventually develop into the conus medullaris, cauda equina, and filum terminale. The filum terminale forms through regression of the most caudal portion of the caudal cell mass during a process called retrogressive differentiation. A thickened filum terminale may result from incomplete involution of the caudal cell mass.2, 3, 11 The thickened and shortened filum terminale causes progressive and repeated traction on the conus medullaris and caudal spinal cord segments. This results in decreased blood flow and decreased oxidative metabolism of the spinal cord segments just cranial of the inelastic abnormality.1, 12 TCS therefore typically results in progressive dysfunction of the lumbosacral spinal cord segments.1, 2 The degree and reversibility of this dysfunction depends on both the magnitude and duration of the excessive traction.13 In the case reported here, reaching a diagnosis of TCS proved to be very challenging. Interpretation of advanced imaging was subjective and unfortunately inconclusive. A diagnosis of TCS was only confirmed during surgery. In people with TCS, MRI is considered the imaging modality of choice and abnormalities typically include a thickening of the filum terminale and an elongated conus medullaris in an abnormally caudodorsal position.1, 2, 3 This radiological definition is difficult to use in dogs, because there is considerable variability in termination of the conus medullaris14 and filum terminale.10 Furthermore, no specific data are available on normal MRI or CT characteristics of the canine filum terminale. A proportion of people with primary TCS present with the conus medullaris in a normal position. This is referred to as occult TCS.15, 16 Considering these arguments, it cannot be excluded the dog described here presented with occult TCS instead of TCS with an abnormal caudodorsal position of the conus medullaris. Performing MRI in different body positions has been evaluated to facilitate diagnosing occult TCS in people. Decreased spinal cord motion between the prone and supine position has been considered suggestive for TCS.15, 17 The dog presented here, recovered completely after surgical transection of the filum terminale. Because untreated TCS will lead to progressive deterioration of neurological function, surgical untethering is considered the treatment of choice in people.1, 16 The goal of surgery is to remove abnormal tension on the spinal cord without causing further trauma.1 In contrast to TCS associated with more complex vertebral malformations, such as spina bifida, transection of a thickened filum terminale is considered a technically straightforward procedure associated with a low postoperative morbidity and good prognosis for recovery. Rethetering with recurrence of clinical signs, caused by arachnoid adhesions, has been reported in a small proportion of surgically treated cases.16, 17, 18, 19, 20
In summary, this report described TCS associated with a thickened filum terminale in a dog. Reaching a diagnosis was challenging and surgery resulted in complete clinical recovery. TCS associated with a thickened filum terminale could be considered a rare differential diagnosis for lumbosacral neurological dysfunction in a young dog.
Acknowledgments
Funding: No funding was received for this study.
Conflict of Interest Declaration: Authors disclose no conflict of interest.
Off‐label Antimicrobial Declaration: Authors declare no off‐label use of antimicrobials.
Department of Veterinary Clinical Science and Services, The Royal Veterinary College, University of London, Hawkshead Lane, North Mymms, Hertfordshire AL97TA, England.
This case report was presented in abstract form (poster) at the 27th Symposium of the European College of Veterinary Neurology (ECVN), 18–20 September 2014, Madrid, Spain.
Footnotes
1.5 tesla Intera, Philips Medical System, Eindhoven, the Netherlands
0.1 mL/kg gadoterate meglumine, Dotarem, Guerbet, Milton Keynes, England
PQ 500, Universal Systems, Solon, OH
References
- 1. Lew SM, Kothbauer KF. Tethered cord syndrome: An updated review. Pediatr Neurosurg 2007;43:236–248. [DOI] [PubMed] [Google Scholar]
- 2. Hertzler DA, Depowell JJ, Stevenson CB, et al. Tethered cord syndrome: A review of the literature from embryology to adult presentation. Neurosurg Focus 2010;29:E1. doi:103171/20103Focus1079. [DOI] [PubMed] [Google Scholar]
- 3. Michelson DJ, Ashwal S. Tethered cord syndrome in childhood: Diagnostic features and relationship to congenital anomalies. Neurol Res 2004;26:745–753. [DOI] [PubMed] [Google Scholar]
- 4. Yamada S, Won DJ. What is the true tethered cord syndrome? Childs Nerv Syst 2007;23:371–375. [DOI] [PubMed] [Google Scholar]
- 5. Fingeroth JM, Johnson GC, Burt JK, et al. Neuroradiographic diagnosis and surgical repair of tethered cord syndrome in an English bulldog with spina bifida and myeloschisis. J Am Vet Med Assoc 1989;194:1300–1302. [PubMed] [Google Scholar]
- 6. Plummer SB, Bunch SE, Khoo LH, et al. Tethered spinal cord and intradural lipoma associated with a meningocele in a Manx‐type cat. J Am Vet Med Assoc 1993;203:1159–1161. [PubMed] [Google Scholar]
- 7. Shamir M, Rochkind S, Johnston D. Surgical treatment of tethered spinal cord syndrome in a dog with myelomeningocele. Vet Rec 2001;148:755–756. [DOI] [PubMed] [Google Scholar]
- 8. Zani DD, De Zani D, Morandi N, et al. Imaging diagnosis—Split cord malformation. Vet Radiol Ultrasound 2010;51:57–60. [DOI] [PubMed] [Google Scholar]
- 9. Ricci E, Cherubini GB, Jakovljevic S, et al. MRI findings, surgical treatment and follow‐up of a myelomeningocele with tethered spinal cord syndrome in a cat. J Feline Med Surg 2011;13:467–472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Fletcher TF. Spinal cord and meninges In: Evans HE. and de Lahunta A, ed. Miller's Anatomy of the Dog, 4th ed. St Louis, Missouri: Elsevier Saunders; 2013: 589–610. [Google Scholar]
- 11. Yamada S, Zinke DE, Sanders D. Pathophysiology of “tethered cord syndrome”. J Neurosurg 1981;54:494–503. [DOI] [PubMed] [Google Scholar]
- 12. Filipiddis AS, Kalani Y, Theodore N, et al. Spinal cord traction, vascular compromise, hypoxia, and metabolic derangements in the pathophysiology of tethered cord syndrome. Neurosurg Focus 2010;29:E1. doi:103171/20103Focus1085. [DOI] [PubMed] [Google Scholar]
- 13. Yamada S, Iacono RP, Andrade T, et al. Pathophysiology of tethered cord syndrome. Neurosurg Clin N Am 1995;6:311–323. [PubMed] [Google Scholar]
- 14. De Lahunta A, Glass E. Lower motor neuron: Spinal nerve, general somatic efferent system In: de Lahunta A. and Glass E, ed. Veterinary Neuroanatomy and Clinical Neurology, 3rd ed. St Louis, Missouri: Elsevier Saunders; 2009:77–133. [Google Scholar]
- 15. Nakanishi K, Tanaka N, Kamei N, et al. Use of prone position magnetic resonance imaging for detecting the terminal filum in patients with occult tethered cord syndrome. J Neurosurg Spine 2013;18:76–84. [DOI] [PubMed] [Google Scholar]
- 16. Steinbok P, MacNeily AE. Section of the terminal filum for occult tethered cord syndrome: Toward a scientific answer. Neurosurg Focus 2007;23:E5. doi: 10.3171/FOC‐07/08/E5. [DOI] [PubMed] [Google Scholar]
- 17. Vernet O, O'Gorman AM, Farmer J‐P, et al. Use of the prone position in the MRI evaluation of spinal cord rethetering. Pediatr Neurosurg 1996;25:286–294. [DOI] [PubMed] [Google Scholar]
- 18. Ogiwara H, Lyszczarz A, Alden TD, et al. Rethetering of transected fatty filum terminalis. J Neurosurg Pediatr 2011;7:42–46. [DOI] [PubMed] [Google Scholar]
- 19. Yong RL, Habrock‐Bach TH, Vaughan M, et al. Symptomatic retethering of the spinal cord following section of a thight filum terminale. Neurosurg 2011;68:1594–1602. [DOI] [PubMed] [Google Scholar]
- 20. Ostling LR, Bierbrauer KS, Kuntz C IV. Outcome, reoperation, and complications in 99 consecutive children operated for thight or fatty filum. World Neurosurg 2012;77:187–191. [DOI] [PubMed] [Google Scholar]