

Summary:
We describe a case in which hyperbaric oxygen therapy was used to salvage ischemic skin flaps after nipple-sparing mastectomy.
A 71-year-old woman with hypothyroidism, BRCA-2 gene mutation, and previous bilateral breast cancer presented for prophylactic bilateral nipple-sparing mastectomies and reconstruction with implantation of bilateral silicone elastomer tissue expanders and use of SERI surgical scaffold (Allergan, Medford, Mass.). There was previous left partial mastectomy, radiation, and endocrine therapy with tamoxifen and an aromatase inhibitor for invasive ductal and lobular carcinoma and ductal carcinoma in situ, and later right partial mastectomy for estrogen and progesterone receptor positive ductal carcinoma in situ. The final pathology was negative for malignancy. During reconstruction, the right breast developed early signs of ischemia, prompting instillation of only 50 mL normal saline, approximately 20% of their capacity. By the first postoperative day, ischemic necrosis developed bilaterally (Fig. 1). Hyperbaric oxygen therapy was initiated at 2.0 atmospheres for 120 minutes on day 1, followed by 90-minute sessions twice daily for 2 days and 120 minutes daily for the remaining treatments. There was substantial improvement in the appearance of the flaps after 15 sessions (Fig. 2), when treatment stopped because of wheezing and oropharyngeal mucosal dryness. Beginning 10 weeks postoperatively [6 weeks after completing hyperbaric oxygen (HbO) therapy], the tissue expanders were filled in 40 mL increments to a total volume of 250 mL. She underwent implant exchange 10 months postoperatively (Fig. 3).
Fig. 1.

Postoperative day 1. Right breast flap showing significant ischemia.
Fig. 2.
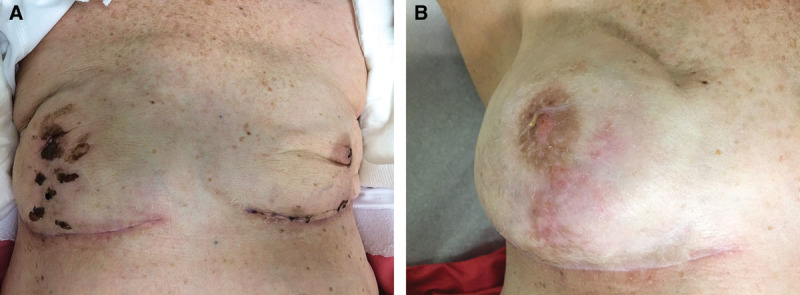
Interval improvement in ischemia at (A) 7 weeks postoperatively and 4 weeks after completion of HbO therapy and (B) 6 months postoperatively and 5.5 months after HbO therapy.
Fig. 3.

One year after initial surgery and 10 months after HbO therapy.
DISCUSSION
Up to 30% of patients undergoing immediate breast reconstruction after mastectomy develop partial loss of skin flap viability,1,2 and this delays adjuvant therapy for malignancy, requires additional surgical procedures, and compromises aesthetic outcomes. Tissue hypoxia also impairs leukocyte bactericidal activity and delays healing. Compromised tissue may respond favorably to hyperbaric oxygen therapy3,4 through various mechanisms, including angiogenesis, increased tissue levels of reactive oxygen and nitrogen species, inhibition of β2 integrins, limiting production of inflammatory cytokines, enhancing endogenous antimicrobial activity, and promoting collagen production by fibroblasts.1,5 Treatment protocols vary but typically involve 60- to 120-minute sessions of high concentration oxygen delivery by face mask, tent, or endotracheal tube at pressures of 2 to 2.5 atmospheres, raising systemic arterial oxygen tension to nearly 1500 torr.6,7
A search of the English literature identified only 2 earlier case reports of hyperbaric oxygen therapy to prevent necrosis of ischemic skin flaps after mastectomy. One involved a woman with BRCA-2 gene mutation who developed erythematous wound dehiscence 1 day after bilateral mastectomy and implant reconstruction. After 20 sessions of HbO therapy initiated on postoperative day 4, the patient developed hyperoxic seizure, which is treated with midazolam. The authors reported improvement in skin flap viability, and after debridement of necrotic tissue, the outcome was satisfactory.1 The other case involved a woman with antecedent breast irradiation who developed ischemia after a skin-sparing mastectomy.2 The skin flap appeared compromised during the reconstructive phase, HbO therapy was initiated 6 hours postoperatively, and signs of ischemia abated after 5 sessions over 3 days.
There is little evidence regarding the optimum timing of HbO therapy for this indication. The few case reports available suggest that acute wounds respond best when treatment is initiated early, but there have been no controlled studies. Among the unanswered questions is whether preoperative HbO therapy reduces the risk of postoperative tissue necrosis in patients with radiation-related tissue injury. Complications of HbO therapy include pneumothorax and potentially fatal seizures,6 but the risks and long-term outcomes of HbO therapy have not been adequately evaluated.
Our patient, like one previously described, had breast cancer associated with a BRCA-2 gene mutation and had previously undergone breast irradiation. In all 3 cases, ischemia developed when immediate breast reconstruction was attempted after mastectomy, and the flaps survived after HbO therapy, although no information is available from comparative studies involving alternative strategies. Soft tissue injury can develop years after exposure to therapeutic radiation, leading to fibrosis or microvascular compromise.1 Although reported infrequently, we speculate that HbO therapy might prevent skin flap necrosis and reduce the need for debridement or flap revision.
CONCLUSIONS
We describe a patient in whom bilateral skin flap ischemia developed after nipple-sparing mastectomies. Tissue expander reconstruction was successfully salvaged with HbO therapy. Clinicians should consider the potential benefits and risks of early postoperative HbO therapy in similar situations, but further research is needed to confirm the efficacy of and indications for HbO therapy after mastectomy. Such studies should also address the optimum method and timing of intervention and explore the potential prophylactic value of preoperative HbO therapy in patients at greatest risk, such as those previously exposed to adjuvant radiation therapy.
Footnotes
Disclosure: Dr. Mesbahi is a consultant and on the speakers bureau for Allergan, Novadaq, and Davol. The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Mermans JF, Tuinder S, von Meyenfeldt MF, et al. Hyperbaric oxygen treatment for skin flap necrosis after a mastectomy: a case study. Undersea Hyperb Med. 2012;39:719–723. [PubMed] [Google Scholar]
- 2.Fredman R, Wise I, Friedman T, et al. Skin-sparing mastectomy flap ischemia salvage using urgent hyperbaric chamber oxygen therapy: a case report. Undersea Hyperb Med. 2014;41:145–147. [PubMed] [Google Scholar]
- 3.Gessell L. Hyperbaric Oxygen Therapy Indications. 12th ed. Durham, NC: Undersea and Hyperbaric Medical Society; 2008. [Google Scholar]
- 4.Baynosa RC, Zamboni WA. The effect of hyperbaric oxygen on compromised grafts and flaps. Undersea Hyperb Med. 2012;39:857–865. [PubMed] [Google Scholar]
- 5.Zamboni WA, Browder LK, Martinez J. Hyperbaric oxygen and wound healing. Clin Plast Surg. 2003;30:67–75. doi: 10.1016/s0094-1298(02)00068-8. [DOI] [PubMed] [Google Scholar]
- 6.Hoggan BL, Cameron AL. Systematic review of hyperbaric oxygen therapy for the treatment of non-neurological soft tissue radiation-related injuries. Support Care Cancer. 2014;22:1715–1726. doi: 10.1007/s00520-014-2198-z. [DOI] [PubMed] [Google Scholar]
- 7.Wang C, Schwaitzberg S, Berliner E, et al. Hyperbaric oxygen for treating wounds: a systematic review of the literature. Arch Surg. 2003;138:272–279; discussion 280. doi: 10.1001/archsurg.138.3.272. [DOI] [PubMed] [Google Scholar]