

Abstract
Sinonasal teratocarcinosarcoma is an extremely rare malignant tumor arising in the sinonasal tract, having combined histological features of teratoma and carcinosarcoma. Here, we are presenting a case of sinonasal teratocarcinosarcoma in a 28-year-old male patient. A 28-year-old male patient presented with left-sided nasal obstruction and recurrent epistaxis for last 2 months. On examination, a polypoid mass was noted in the left nasal cavity. The mass was surgically resected. Paraffin-embedded sections were made and stained with hematoxylin and eosin. Microscopic examination revealed intimate admixture of carcinomatous (adenocarcinoma), sarcomatous (chondrosarcoma), primitive neuroendocrine and teratoid elements (immature squamous elements). These findings clearly suggest the diagnosis of sinonasal teratocarcinosarcoma. Sinonasal teratocarcinosarcoma is highly malignant and locally aggressive. About 60% of the patients do not survive beyond 3 years. Total excision and extensive sampling are necessary to reach the diagnosis. Early diagnosis and management can give a better prognosis.
Keywords: Malignant teratoma, sinonasal mass, teratocarcinoma, teratocarcinosarcoma
INTRODUCTION
Sinonasal teratocarcinosarcoma is a rare tumor of nasal cavity and of uncertain histogenesis.[1,2] Almost all cases are found in adults with a significant male predominance.[3] Histogenetically, this tumor is unlikely to be of germ cell origin but probably arises from a primitive cell in the olfactory membrane that not only reproduces the neuroectodermal features of olfactory neuroblastoma but also has the capacity to differentiate into divergent types of somatic cells.[4] Phenotypically, there are multiple tissue types derived from two or three germ layers, exhibiting variable degrees of maturity. In addition, there are intermingled carcinomatous and sarcomatous components.[5] Because of the infrequency and the complex phenotypic composition, these lesions are often misdiagnosed, leading to management difficulties.[4,5,6,7] This tumor almost always arises in the ethmoid sinus and maxillary antrum and patients present with nasal obstruction and occasional epistaxis.[3,7,8,9] Histopathological findings of this tumor comprise a complex malignant neoplasm having combined features of teratoma and carcinosarcoma. Benign and malignant epithelial, mesenchymal and neural elements are typically present in this tumor, including immature tissue with blastomatous features, while embryonal carcinoma, choriocarcinoma or seminoma is typically absent.[1,2,3,8,9] Teratocarcinosarcoma is highly malignant and locally aggressive, with high recurrence rate. The average survival is <2 years.[1,2,3,6,7,8,9]
Here, we are presenting a case of sinonasal teratocarcinosarcoma in a 28-year-old male patient.
CASE REPORT
A 28-year-old male patient presented with right-sided nasal obstruction for last 2 months and recurrent episodes of epistaxis for last 1 month. On examination, a polypoid mass was seen in the right nasal cavity and a clinical diagnosis of infected antrochoanal polyp was made. Then, a computed tomography (CT) scan of paranasal sinuses was advised. CT scan revealed soft tissue attenuation in the right maxillary antrum, extending to the right nasal cavity. Bone destruction was seen in both the lateral wall of maxillary sinus and inferior wall of the orbit, with infiltration into the anterior ethmoidal sinus [Figure 1]. The polypoid mass was surgically resected and transported in 10% formalin. Tissue was sent in multiple pieces altogether measuring 8 cm × 7 cm × 2.5 cm [Figure 2]. Paraffin-embedded sections were made and sections were stained with hematoxylin and eosin. Microscopic examination of the sections from different areas showed variegated appearance having intimate admixture of carcinomatous, sarcomatous, primitive neuroectodermal and teratoid elements [Figure 3]. Sarcomatous component was predominantly having chondroid differentiation with foci of endochondral calcification [Figure 4]. Areas of moderately differentiated adenocarcinoma were noted [Figure 5] along with undifferentiated primitive neuroectodermal elements in solid sheets [Figure 6]. Immature squamous elements with formation of keratin pearls were seen at places, which were the teratoid element of the tumor [Figure 7]. These microscopical findings clearly suggest the diagnosis of sinonasal teratocarcinosarcoma.
Figure 1.

Computed tomography scan: Mass in right maxillary antrum, extending to right nasal cavity
Figure 2.
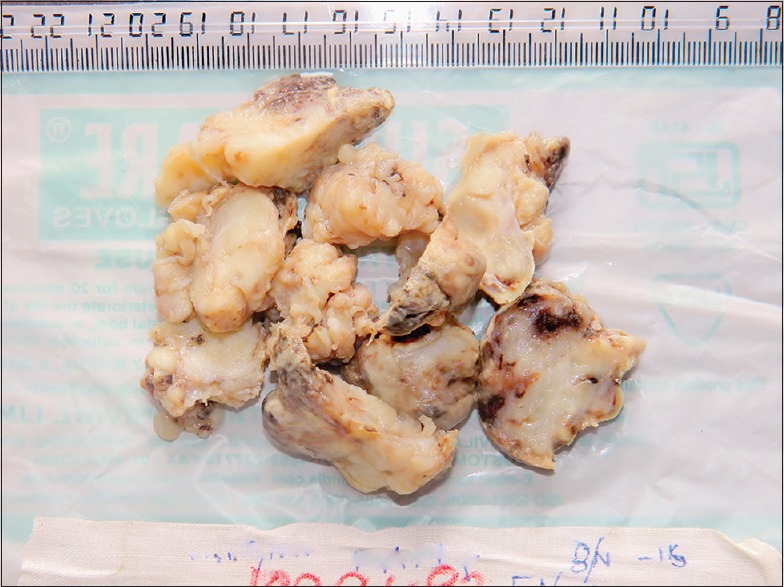
Gross morphology of the specimen: Multiple pieces of grayish yellow-colored firm tissue
Figure 3.
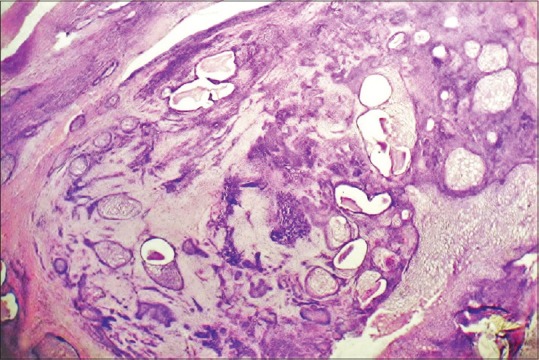
Scanner view of tumor showing the overall variegated appearance (H&E stain, ×40)
Figure 4.
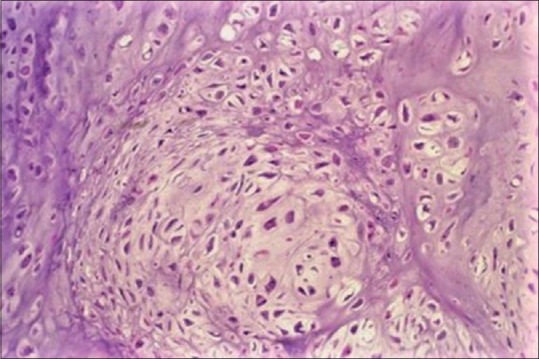
Photomicrograph of sarcomatous component with chondroid differentiation (H&E stain, ×200)
Figure 5.
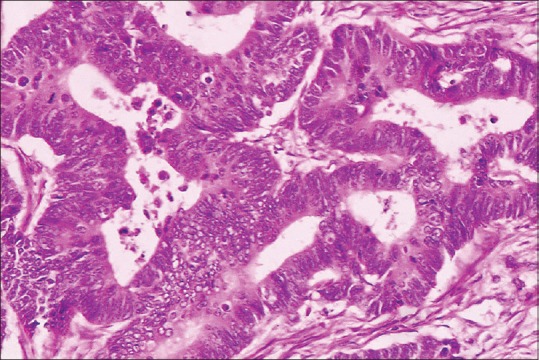
Photomicrograph of carcinomatous component (adenocarcinoma) (H&E stain, ×200)
Figure 6.
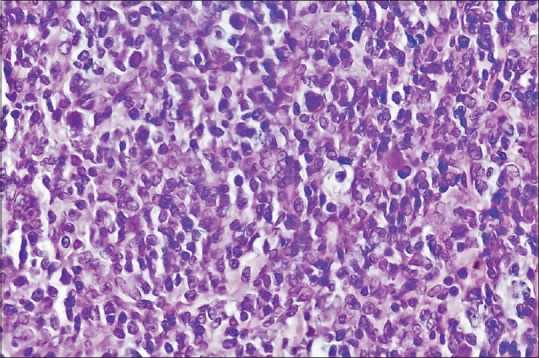
Photomicrograph of primitive neuroectodermal component (H&E stain, ×400)
Figure 7.
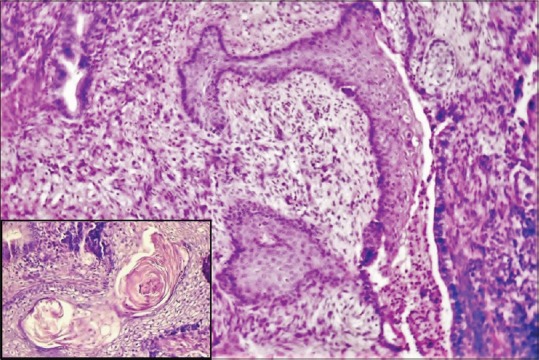
Photomicrograph of squamous component (H&E stain, ×100). Inset: High power view of keratin pearl (H&E stain, ×400)
In spite of complete surgical clearance, a course of radiotherapy and one cycle of combination chemotherapy (cisplatin + 5-fluorouracil) were given. Thereafter, the patient was lost to follow-up.
DISCUSSION
These tumors were previously termed as malignant teratoma, blastoma, teratocarcinoma, carcinosarcoma, teratoid carcinosarcoma, mixed mesodermal tumor and malignant mixed tumor. Heffner and Hyams first coined the term “teratocarcinosarcoma” based on a clinicopathological study on twenty cases of sinonasal tract neoplasm.[5] This tumor is still very rare. Till date, there are <100 cases reported in English literature. It is almost exclusively seen in adults with only three pediatric cases being reported.[10]
This tumor is found much more commonly in male with a male:female ratio of approximately 4:1. It almost exclusively arises in the ethmoid sinus and maxillary antrum.[1,2,3] One tumor has been reported to arise in the roof of the nasopharynx and another from the dorsum of the tongue.[11,12]
Morphologically, these tumors are bulky, friable to firm, red-brown masses.[3,8] On microscopy, teratocarcinosarcomas are characterized by a combination of epithelial and mesenchymal tissue components with variable growth patterns. The epithelial components include glandular or ductal structures lined by benign-appearing, partly ciliated columnar epithelium with transitional areas of nonkeratinizing squamous epithelium, with or without clear cells. In addition, areas of squamous carcinoma and adenocarcinoma are present. The mesenchymal components may include fibroblasts or myofibroblasts of benign and malignant appearance, benign cartilage with an immature appearance and chondrosarcoma or osteogenic tissue. The teratoid components include “fetal appearing” clear cell squamous epithelium, organoid structures or neural tissue in the form of neural rosettes and neurofibrillary matrix are also seen. The “fetal-appearing” clear cell squamous epithelium represents a characteristic histologic finding in this entity and is a supportive evidence of the teratoid nature of this neoplasm. Foci of seminoma, choriocarcinoma or embryonal carcinoma have not been found in association with these tumors.[1,2,3,8,9]
Inadequate sampling may lead to erroneous diagnoses of olfactory neuroblastoma, squamous cell carcinoma, undifferentiated carcinoma, adenocarcinoma, malignant salivary gland-type tumors and adenosquamous carcinoma.[3,13]
Immunohistochemical staining is dependent on the cell type; epithelial components are cytokeratin and epithelial membrane antigen positive; neuroepithelial components are neuron-specific enolase, CD99, chromogranin, synaptophysin, glial fibrillary acidic protein and S-100 protein positive; mesenchymal components are vimentin positive and depending on cell types may be reactive for myogenic markers or smooth muscle actin.[8,14]
These tumors are locally aggressive, rapidly invade soft tissue and bone as well as the orbit and cranial cavities. They also have the potential to metastasize to regional lymph nodes and distant sites, mainly the lungs. The average survival is <2 years with 60% of the patients not surviving beyond 3 years. Recurrence is common and usually appears within 3 years.[1,2,3,4,5,6,7,8,9]
There are three significant case series studies which have emphasized on clinical features, histopathological diagnosis and treatment options of this tumor.
Heffner and Hyams did the first case series study on twenty cases from Armed Forces Institute of Pathology, Washington, DC. They ranged from 18 to 79 years with median age of 60 years. From this study, they first named this tumor teratocarcinosarcoma. They found that teratocarcinosarcoma is highly aggressive tumor and suggested multimodality treatment.[5]
Next case series study was done by Smith et al. on 10 cases from Texas, ranging in age from 35 to 69 years (mean age of 53 years). They had a brief episode of symptoms with an average duration of 3.5 months. Nine of them presented with nasal obstruction and epistaxis. Histologically, the tumors showed primitive neuroepithelial elements and various malignant epithelial and mesenchymal components. Six patients had no evidence of disease by the end of follow-up, which ranged from 72 to 372 months. Three patients died of disease and one patient was lost to follow-up. From that study, they concluded that sinonasal teratocarcinosarcoma of the head and neck is histologically and biologically a heterogeneous malignant neoplasm that is best managed with surgery and postoperative radiotherapy.[15]
Another case series study was done by Budrukkar et al. They reviewed the medical records of 22 patients (21 male and one female) with histopathologically proven sinonasal teratocarcinosarcoma diagnosed during the period 1993–2007, among which treatment was completed in 16 patients. Fourteen patients underwent surgery, which was followed by radiation therapy with or without chemotherapy in 11 patients. Two patients received chemoradiation as the definitive treatment. At median follow-up of 34 months (range 1–180 months) in the surviving patients, only five were under control. Disease recurred in 11 patients, with a median time to recurrence of 7 months. The 2-year disease-free survival rate and the overall survival rate were 28% and 46%, respectively. From that study, they proposed that multimodality treatment, in the form of a combination of surgery, radiation therapy and chemotherapy appears to be the optimal approach for this tumor.[16]
CONCLUSION
Teratocarcinosarcoma is a rare sinonasal tumor. Total excision of the tumor and aggressive sampling for histopathological examination is necessary to avoid erroneous diagnosis. Multimodality treatment in the form of chemotherapy, with or without radiotherapy following surgery is mandatory for the good clinical outcome. Very aggressive follow-up is necessary to detect early recurrences. Early diagnosis and management before regional spread can give a better prognosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Shanmugaratnam K. Geneva: WHO; 1991. Histological Typing of Tumours of the Upper Respiratory Tract and Ear; pp. 173–5. [Google Scholar]
- 2.Redondo Martínez E, Rey López A, Reguera Parra V, Bolaños Rodríguez C. Sinusal teratocarcinosarcoma. Acta Otorrinolaringol Esp. 1991;42:363–7. [PubMed] [Google Scholar]
- 3.Barnes L, Eveson JW, Reichart P, Sidransky D. 3rd ed. Lyon: International Agency for Research on Cancer; 2005. World Health Organization Classification of Tumours: Pathology and Genetics of Head and Neck Tumours; pp. 76–7. [Google Scholar]
- 4.Batsakis JG, el-Naggar AK, Luna MA. Teratomas of the head and neck with emphasis on malignancy. Ann Otol Rhinol Laryngol. 1995;104:496–500. doi: 10.1177/000348949510400616. [DOI] [PubMed] [Google Scholar]
- 5.Heffner DK, Hyams VJ. Teratocarcinosarcoma (malignant teratoma?) of the nasal cavity and paranasal sinuses a clinicopathologic study of 20 cases. Cancer. 1984;53:2140–54. doi: 10.1002/1097-0142(19840515)53:10<2140::aid-cncr2820531025>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 6.Prasad KC, Pai RR, Padmanabhan K, Chawla S. Teratocarcinosarcoma of the nose, paranasal sinuses and nasopharynx. J Laryngol Otol. 2003;117:321–4. doi: 10.1258/00222150360600986. [DOI] [PubMed] [Google Scholar]
- 7.Chao KK, Eng TY, Barnes J, Dahiya R. Sinonasal teratocarcinosarcoma. Am J Clin Oncol. 2004;27:29–32. doi: 10.1097/01.coc.0000045851.76922.2e. [DOI] [PubMed] [Google Scholar]
- 8.Fletcher CD. 4th ed. Philadelphia: Elsevier Saunders; 2013. Diagnostic Histopathology of Tumors; pp. 143–4. [Google Scholar]
- 9.Wei S, Carroll W, Lazenby A, Bell W, Lopez R, Said-Al-Naief N. Sinonasal teratocarcinosarcoma: Report of a case with review of literature and treatment outcome. Ann Diagn Pathol. 2008;12:415–25. doi: 10.1016/j.anndiagpath.2007.05.003. [DOI] [PubMed] [Google Scholar]
- 10.Agrawal N, Chintagumpala M, Hicks J, Eldin K, Paulino AC. Sinonasal teratocarcinosarcoma in an adolescent male. J Pediatr Hematol Oncol. 2012;34:e304–7. doi: 10.1097/MPH.0b013e318266baa8. [DOI] [PubMed] [Google Scholar]
- 11.Sarin YK. An unusual congenital nasopharyngeal teratoma. Pediatr Surg Int. 1999;15:56–7. doi: 10.1007/s003830050512. [DOI] [PubMed] [Google Scholar]
- 12.Crazzolara R, Puelacher W, Ninkovic M, Zelger B, Buchberger W, Meister B, et al. Teratocarcinosarcoma of the oral cavity. Pediatr Blood Cancer. 2004;43:687–91. doi: 10.1002/pbc.20139. [DOI] [PubMed] [Google Scholar]
- 13.Endo H, Hirose T, Kuwamura KI, Sano T. Case report: Sinonasal teratocarcinosarcoma. Pathol Int. 2001;51:107–12. doi: 10.1046/j.1440-1827.2001.01170.x. [DOI] [PubMed] [Google Scholar]
- 14.Pai SA, Naresh KN, Masih K, Ramarao C, Borges AM. Teratocarcinosarcoma of the paranasal sinuses: A clinicopathologic and immunohistochemical study. Hum Pathol. 1998;29:718–22. doi: 10.1016/s0046-8177(98)90281-7. [DOI] [PubMed] [Google Scholar]
- 15.Smith SL, Hessel AC, Luna MA, Malpica A, Rosenthal DI, El-Naggar AK. Sinonasal teratocarcinosarcoma of the head and neck: A report of 10 patients treated at a single institution and comparison with reported series. Arch Otolaryngol Head Neck Surg. 2008;134:592–5. doi: 10.1001/archotol.134.6.592. [DOI] [PubMed] [Google Scholar]
- 16.Budrukkar A, Agarwal JP, Kane S, Siddha M, Laskar SG, Pai P, et al. Management and clinical outcome of sinonasal teratocarcinosarcoma: Single institution experience. J Laryngol Otol. 2010;124:739–43. doi: 10.1017/S0022215109992866. [DOI] [PubMed] [Google Scholar]