

Abstract
Physical symptoms are common in depression, and, in fact, vague aches and pain are often the presenting symptoms of depression. These symptoms include chronic joint pain, limb pain, back pain, gastrointestinal problems, tiredness, sleep disturbances, psychomotor activity changes, and appetite changes. A high percentage of patients with depression who seek treatment in a primary care setting report only physical symptoms, which can make depression very difficult to diagnose. Physical pain and depression have a deeper biological connection than simple cause and effect; the neurotransmitters that influence both pain and mood are serotonin and norepinephrine. Dysregulation of these transmitters is linked to both depression and pain. Antidepressants that inhibit the reuptake of both serotonin and norepinephrine may be used as first-line treatments in depressed patients who present with physical symptoms. Many physicians consider patients to be in remission when their acute emotional symptoms have abated, but residual symptoms—including physical symptoms—are very common and increase the likelihood of relapse. All symptoms must be measured in order to achieve full remission. There are a number of short yet accurate measurement tools (rating scales) available that effectively measure the remission of physical symptoms as well as emotional symptoms.
PHYSICAL SYMPTOMS IN DEPRESSION
Physical symptoms are common in major depression and may lead to chronic pain and complicate treatment. Symptoms associated with depression include joint pain, limb pain, back pain, gastrointestinal problems, fatigue, psychomotor activity changes, and appetite changes. In the primary care setting, a high percentage of patients with depression present exclusively with physical symptoms. Simon et al.1 analyzed a World Health Organization study of somatic symptoms in the presentation of depression. Of the 1146 patients in 14 countries included in the survey who met the criteria for depression, 69% reported only somatic symptoms as the reason for their visit. Unfortunately, depression can often go undiagnosed in these patients, as the physical symptoms associated with depression may be interpreted as symptoms of a somatic illness.
Patients who present with a high number of physical symptoms may be more likely to have a mood disorder than patients who present with only a few physical symptoms. Kroenke et al.2 studied 1000 adult primary care clinic patients and found that the number of physical symptoms present was highly predictive of mood disorders and functional impairment. In patients who reported 0 or 1 physical symptom, 2% were found to have a mood disorder, but among patients who reported 9 or more physical symptoms, 60% were found to have a mood disorder (Figure 1). Overall, the presence of any physical symptom approximately doubled the likelihood that the patient had a mood disorder.
Figure 1.

Physical Symptoms as a Predictor of Mood Disordersa
In general, the worse the painful physical symptoms, the more severe the depression. Physical symptoms have been found to increase the duration of depressed mood. In a study of chronic pain as a predictor of depressive morbidity in the general population, Ohayon and Schatzberg3 found that of the study participants who reported at least 1 key symptom of depression, those with a chronic painful physical condition reported a longer duration of depressed mood (19.0 months) than those without chronic pain (13.3 months).
Physical symptoms are also generally accompanied by a significant level of dysfunction in depressed patients. Elevated rates of suicidal thoughts are found in patients with chronic pain. Ohayon and Schatzberg3 reported that, among patients who reported at least 1 key symptom of depression, 33% of those who reported suicidal thoughts (N = 687) also reported a painful condition. A review of the literature by Fishbain4 found that suicidal ideation, suicide attempts, and suicide completions are commonly found in patients with chronic pain. Fishbain noted that several of the reviewed studies indicated that chronic pain may be a suicide risk factor.
The link between pain and depression appears to be a shared neurologic pathway.5 Response to painful physical stimuli is moderated in the brain by serotonin and norepinephrine, which also affect mood. Patients with neurotransmitter dysregulation may have an imbalance of serotonin and norepinephrine, which may explain the connection between painful physical symptoms and depression. When a patient with depression complains that he or she is feeling physical pain, there may be a chemical reason.
Therefore, antidepressants that inhibit the reuptake of both norepinephrine and serotonin have the best chance to reduce physical symptoms in patients with depression because they target the pathways that mediate both pain and depression in the brain and in the spinal cord.6 Antidepressant medications that act as dual serotonin-norepinephrine reuptake inhibitors, such as venlafaxine and duloxetine, may aid in correcting the imbalance of serotonin and norepinephrine neurotransmission in the brain.
INCORPORATING PHYSICAL SYMPTOMS INTO TREATMENT GOALS
As with any general medical disorder, full remission should be the long-range objective in the treatment of mood disorders. Many physicians consider a patient to be in remission from depression when his or her acute emotional symptoms have abated, but residual symptoms, including physical symptoms, increase the likelihood of relapse. Physicians should move beyond simple treatment of acute symptoms to a model in which patients are treated until full remission is achieved; a virtually asymptomatic state rather than simple response should be the ultimate goal of therapy. Many patients treated with antidepressants fail to achieve full remission, and the costs, both social and economic, of relapse or residual symptoms are high.
Numerous studies have shown7–9 that patients with major depression who have residual symptoms after treatment have higher relapse rates and they relapse earlier than do those without residual symptoms. In fact, relapse rates are 3 times higher in individuals who have residual symptoms after they have achieved significant improvement than in individuals with no residual symptoms.8 One may infer, then, that the likelihood of relapse is significantly reduced in patients who attain asymptomatic remission.
Paykel et al.7 studied residual symptoms after partial remission in 64 patients with unipolar depression identified at presentation at a treatment facility; they found that residual symptoms were an important predictor of relapse of depression. All but 4 of the patients had remitted by 15 months, and 19 of those who were considered to have remitted had residual symptoms. Of the 17 individuals with residual symptoms who were followed to completion, 13 (76%) relapsed within 15 months, compared with 10 (25%) of the 40 individuals who remitted without physical symptoms (Figure 2).
Figure 2.

The Relation of Residual Symptoms to Relapse in Depressiona,b
Psychiatrists and primary care physicians are beginning to recognize that even though symptom domains in the areas of motivation and physical illness are frequently part of depression, they are often ignored in the assessment of depression and, subsequently, in the treatment goals. Often, pain is not included in the treatment goals because it is interpreted as a sign of a somatic illness. When treating mood disorders such as depression that are frequently associated with painful physical symptoms, the pain component of treatment needs to be given full consideration. Symptom relief that does not include relief of pain may result in an incomplete or false remission. Significant improvement in all symptoms, including physical symptoms as well as general functioning, is necessary not only in the acute period but also in the maintenance phase to prevent relapse and ensure full remission of mood disorders.
The degree of impairment associated with all symptoms of depression, including physical symptoms, should be considered when deciding on a treatment plan. Core symptoms typically dissipate early in the treatment of depression, but physical symptoms such as pain may linger. Treatment should not be discontinued until all symptoms have abated and the patient is in full remisssion.
ACHIEVING REMISSION IN PATIENTS WITH PHYSICAL SYMPTOMS
Treating both the emotion and the physical symptoms associated with depression together is an important part of achieving remission. Unlike selective serotonin reuptake inhibitors such as sertraline and paroxetine, the dual-action antidepressants venlafaxine and duloxetine inhibit the reuptake of both serotonin and norepinephrine. This dual action gives them a robust efficacy in combating depression and preventing the persistence of symptoms, which increases the likelihood of achieving remission. Numerous reports have indicated that therapeutic agents that act on multiple neurotransmitters are associated with higher rates of remission than are single agents.10–13 The selection of therapeutic agents proven to effectively promote both an elimination of a broad spectrum of symptoms and a return to full social functioning is important to the treatment of depression.
Because a majority of patients with depression initially seek treatment for the physical symptoms of depression rather than for their emotional symptoms, physicians are often aware of patients' physical symptoms when treatment commences. Primary care physicians may want to consider using dual-action antidepressants as a first line-treatment in depressed patients who present with physical symptoms.
Treating depression aggressively from the start may increase the chance of remission, as patients who fully remit in the acute stage tend to do better in the continuation phase. Duration of pharmacotherapy is also an important factor in achieving full remission. It is especially important to continue pharmacotherapy into the long term in patients who initially achieve only a partial remission.14 Discontinuing pharmacotherapy too early may disrupt the patient's improvement and cause regression of symptoms.
PHYSICAL SYMPTOMS AND OUTCOME MEASURES
In addition to choosing the most appropriate pharmacotherapeutic approach to treating the symptoms of depression, clinical management of depression should include the screening and monitoring of all symptom domains. All symptoms, including physical ones, must be measured in order to be treated fully. The symptoms still present in incomplete remission are important markers of vulnerability to relapse, and if all types of symptoms are not included in assessments, physicians cannot fully assess the treatment response and follow up on unresolved symptoms. Physicians and patients need to become aware of the broad spectrum of symptoms in depression in order to evaluate treatment effectiveness.
Reliable and effective assessment of Axis I disorders often includes utilization of a variety of rating scales used for both diagnostic purposes and follow-up evaluation. Recently there has been a call for including on rating scales all the symptom domains and social functioning/quality of life measures in the requirements for remission, but physicians may not be aware that there are already numerous standardized scales that measure these aspects of depression.
The most commonly used scales for measuring the symptoms of depression have been the Hamilton Rating Scale for Depression (HAM-D)15 and the Montgomery-Asberg Depression Rating Scale (MADRS).16 These 2 scales have traditionally been used in clinical trials for the express purpose of showing initial drug-placebo separation, but they are long and difficult to use in routine clinical practice. Neither scale includes all 9 DSM-IV criteria for major depressive disorder. Additionally, the parameters used to define remission on both the HAM-D and the MADRS are too inclusive. At a score of ≤ 7 on the HAM-D or ≤ 10 on the MADRS, which are often considered to indicate remission, patients may have shown improvement but are still clearly symptomatic. In addition, due to the demanding nature of these 2 rating scales, the chance they will be frequently used in primary care practices is small.
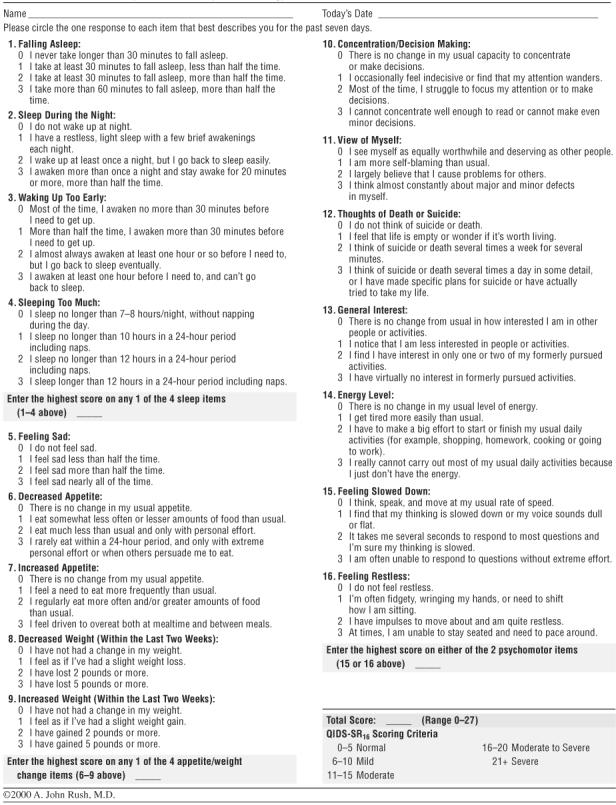
There are several other rating scales to choose from, however. One that has been used for a number of years at the University of Texas Southwestern Medical School is the Inventory of Depressive Symptomatology (IDS).17 The IDS began as a 30-item rating scale, but has now been reduced to a 16-item scale, the Quick Inventory of Depressive Symptomatology (QIDS),18 that includes all 9 DSM-IV depression criteria. The advantage of the IDS and the QIDS is that they have both a clinician-rated version (IDS-C and QIDS-C16) and a self-rated version (IDS-SR and QIDS-SR16). The QIDS-SR16 takes about 5 to 7 minutes for patients to complete, and they can take it repeatedly to measure their progress during treatment (Appendix 1). Patients reportedly find it user-friendly. The psychometrics have been established enough to say that a score of 5 on the QIDS-SR16 can be defined as remission.18
Rush et al.18 have published data showing that, in nonpsychotic major depressive disorder, the self-rated versions of scales produce a significant correlation with the results of the clinician-rated versions and can be substituted easily. They are extremely useful and effective for both diagnosis and measuring improvement. There are a number of other self-rated scales available, including the Beck Depression Inventory,19 the Zung Self-Rating Depression Scale,20 and the Patient Health Questionnaire for depression (PHQ-9)21 (Table 1). Although the PHQ-9 has been traditionally used as a screening instrument, it is increasingly viewed as a brief and accurate tool to measure symptoms during the course of treatment.
Table 1.
Patient-Rated Depression Rating Scales

CONCLUSION
Although the diagnostic criteria emphasize emotional and vegetative symptoms, major depression is also associated with painful physical symptoms such as headache, backache, stomach ache, joint ache, and muscle ache. Because depression and pain share a common neuro-chemical pathway in that they are both influenced by serotonin and norepinephrine, depression and associated painful physical symptoms must be treated together in order to achieve remission. In fact, research22 has shown that physical symptom improvement was correlated with the improvement of other depression symptoms, which suggests that the patient's ability to achieve depression remission may be directly related to the reduction of painful physical symptoms. Patients may experience significant response to treatment; however, if residual symptoms persist, patients might not fully remit and might be at greater risk for subsequent relapse. A treatment regimen that does not address physical symptoms and only focuses on core emotional symptoms could result in an incomplete remission and a poor treatment prognosis for the patient. It is necessary to choose efficacious therapeutic agents that promote the elimination of both the core symptoms and associated physical symptoms of depression to ensure remission and a return to full social functioning and to prevent relapse. There are many standardized rating scales that effectively measure the remission of physical symptoms as well as emotional symptoms.
Drug names: paroxetine (Paxil and others), sertraline (Zoloft), and venlafaxine (Effexor).
Appendix 1.
Quick Inventory of Depressive Symptomatology (Self-Report) (QIDS-SR16)
Footnotes
This article is derived from the teleconference “New Treatments for Depression Characterized by Physical Symptoms,” which was held May 15, 2003, and supported by an unrestricted educational grant from Eli Lilly and Company.
Disclosure of off-label usage: The author has determined that, to the best of his knowledge, no investigational information about pharmaceutical agents has been presented in this article that is outside U.S. Food and Drug Administration–approved labeling.
REFERENCES
- Simon GE, Von Korff M, and Piccinelli M. et al. An international study of the relation between somatic symptoms and depression. N Engl J Med. 1999 341:658–659. [DOI] [PubMed] [Google Scholar]
- Kroenke K, Spitzer RL, and Williams JB. et al. Physical symptoms in primary care: predictors of psychiatric disorders and functional impairment. Arch Fam Med. 1994 3:774–779. [DOI] [PubMed] [Google Scholar]
- Ohayon MM, Schatzberg AF. Using pain to predict depressive morbidity in the general population. Arch Gen Psychiatry. 2003;60:39–47. doi: 10.1001/archpsyc.60.1.39. [DOI] [PubMed] [Google Scholar]
- Fishbain DA. The association of chronic pain and suicide. Semin Clin Neuropsychiatry. 1999;4:221–227. doi: 10.153/SCNP00400221. [DOI] [PubMed] [Google Scholar]
- Basbaum AI, Fields HL. Endogenous pain control mechanisms: review hypothesis. Ann Neurol. 1978;4:451–462. doi: 10.1002/ana.410040511. [DOI] [PubMed] [Google Scholar]
- Stahl SM. Does depression hurt? [BRAINSTORMS] J Clin Psychiatry. 2002;63:273–274. doi: 10.4088/jcp.v63n0401. [DOI] [PubMed] [Google Scholar]
- Paykel ES, Ramana R, and Cooper Z. et al. Residual symptoms after partial remission: an important outcome in depression. Psychol Med. 1995 25:1171–1180. [DOI] [PubMed] [Google Scholar]
- Judd LL, Akiskal HS, and Maser JD. et al. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as predictor of rapid relapse. J Affect Disord. 1998 50:97–108. [DOI] [PubMed] [Google Scholar]
- Kanai T, Takeuchi H, and Furukawa TA. et al. Time to recurrence after recovery from major depressive episodes and its predictors. Psychol Med. 2003 33:839–845. [DOI] [PubMed] [Google Scholar]
- Anderson IM. SSRIs versus tricyclic antidepressants in depressed inpatients: a meta-analysis of efficacy and tolerability. Depress Anxiety. 1998 7suppl 1. 11–17. [PubMed] [Google Scholar]
- Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry. 2001;178:234–241. doi: 10.1192/bjp.178.3.234. [DOI] [PubMed] [Google Scholar]
- Entsuah AR, Huang H, Thase ME. Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J Clin Psychiatry. 2001;62:869–877. doi: 10.4088/jcp.v62n1106. [DOI] [PubMed] [Google Scholar]
- Tran P, Bymaster FP, and McNamara RK. et al. Dual monoamine modulation for improved treatment of major depressive disorder. J Clin Psychopharmacol. 2003 23:78–86. [DOI] [PubMed] [Google Scholar]
- Paykel ES. Continuation and maintenance therapy in depression. Br Med Bull. 2001;57:145–149. doi: 10.1093/bmb/57.1.145. [DOI] [PubMed] [Google Scholar]
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62. doi: 10.1136/jnnp.23.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montgomery SA, Asberg M. A new depression rating scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382–389. doi: 10.1192/bjp.134.4.382. [DOI] [PubMed] [Google Scholar]
- Rush AJ, Giles DE, and Schlesser MA. et al. The Inventory for Depressive Symptomatology (IDS): preliminary findings. Psychiatry Res. 1986 18:65–87. [DOI] [PubMed] [Google Scholar]
- Rush AJ, Trivedi MH, and Ibrahim HM. et al. The 16-item Quick Inventory of Depressive Symptomatology (QIDS), Clinician Rating (QIDS-C), and Self-Report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry. 2003 54:573–583. [DOI] [PubMed] [Google Scholar]
- Beck AT, Ward CH, and Mendelson M. et al. An inventory for measuring depression. Arch Gen Psychiatry. 1961 4:561–571. [DOI] [PubMed] [Google Scholar]
- Zung WWK. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi: 10.1001/archpsyc.1965.01720310065008. [DOI] [PubMed] [Google Scholar]
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Denniger JW, Mahal Y, and Merens W. et al. The relationship between somatic symptoms and depression. In: New Research Abstracts of the 155th annual meeting of the American Psychiatric Association. 21May2002 Philadelphia, Pa. Abstract NR251:68–69. [Google Scholar]