
Figure 7-5.
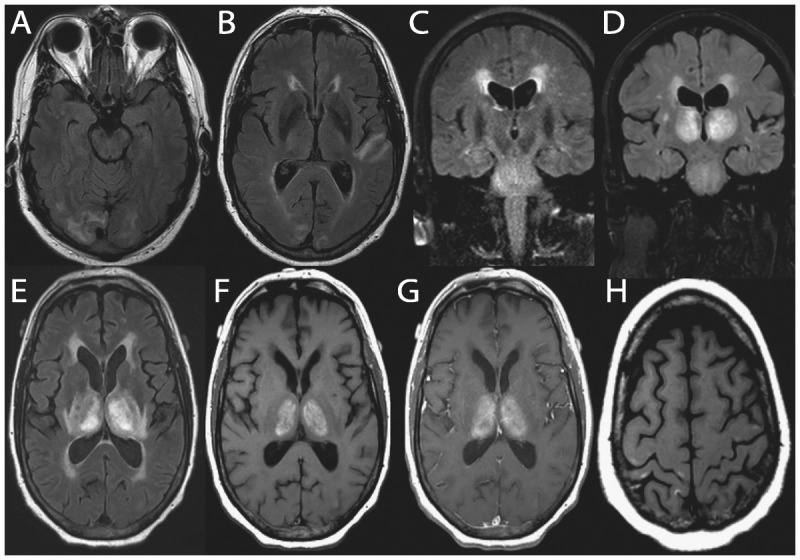
Brain MRI of a 68-year-old man with recent hyperintensive encephalopathy leading to subacute diencephalic angioencephalopathy. His first symptoms were hypernasal dysarthria and palatal weakness that resolved over 3 months after treatment of hypertension. Thirteen months after initial onset, he developed headaches, confusion, and speech and language problems due to hyperintensive encephalopathy, which again resolved with treatment. About 15 months after initial onset, he began a downward, but fluctuating course (with treatments), over 8 weeks, of a rapidly progressive neurologic decline leading to his death. Brain autopsy revealed findings consistent with subacute diencephalic angioencephalopathy. Nonenhancing, confluent subcortical axial fluid-attenuated inversion recovery (FLAIR) hyperintensities in the occipital lobes (A) and left temporal lobe (B) at the time of initial onset. Confluent nonenhancing abnormal coronal T2-weighted signal symmetrically in the pons, as well as confluent periventricular FLAIR signal, at 13 months after onset (C). One month later, imaging demonstrated bilaterally symmetric T1 and T2/FLAIR hyperintense abnormal signal in the thalami (D, coronal FLAIR; E, axial FLAIR). Thalamic abnormalities enhanced minimally following gadolinium administration on axial T1-weighted images (F, unenhanced; G, enhanced). Small T1-weighted (H) and T2-weighted hyperintense cortical foci were also seen.
Reprinted with permission from Graffeo CS, et al, J Clin Neurosci.34 www.jocn-journal.com/article/S0967-5868(15)00354-9/abstract. © 2015 Elsevier Ltd.