

Article first published online 23 November 2015.
Key Words: inflammatory bowel disease, ulcerative colitis, randomized clinical trial, SIRT1 activator, SRT2104
Abstract
Background:
Sirtuins are a class of proteins with important physiologic roles in metabolism and inflammation. Sirtuin (silent mating type information regulation 2 homolog) 1, or SIRT1, activation is an unexplored therapeutic approach for the treatment of ulcerative colitis (UC).
Methods:
Patients with mild to moderately active UC were blindly randomized to 50 mg or 500 mg daily of SRT2104, a selective activator of SIRT1, for 8 weeks. Colonic exposure and safety were assessed, as well as blinded endoscopic scoring and disease activity by Mayo score, Simple Clinical Colitis Activity Index and fecal calprotectin.
Results:
Across both SRT2104 groups, only 3 of 26 evaluable subjects achieved remission on blinded endoscopic assessment. Clinical remission (Mayo score ≤2, no subscore >1) was achieved in 4 patients (2 of 13 evaluable patients in each dose group). Fecal calprotectin levels declined with treatment in both groups, but after 56 days of treatment subjects were still found to have levels approximately 4-fold elevated above normal. One subject experienced an SAE requiring study withdrawal and another was withdrawn for a severe UC flare; 19 subjects (61%) across both treatment groups experienced at least 1 treatment emergent adverse event. Average drug exposure increased in a dose-dependent manner for escalating doses of SRT2104, and colonic exposure was 140 to 160 times higher than plasma exposures.
Conclusions:
SRT2104 did not demonstrate significant clinical activity in mild to moderately active UC. This suggests that further evaluation of SRT2104 as a therapeutic strategy for the treatment of UC is not warranted.
Ulcerative colitis (UC) is a chronic, immune-mediated condition characterized by ongoing inflammation of the large bowel. Symptomatic flares of UC are the result of mucosal inflammation, and patients experience diarrhea, usually with passage of blood, abdominal cramping, and tenesmus. Treatment is directed at reducing inflammation, initially through the use of anti-inflammatory agents such as 5-aminosalicylates1 or corticosteroids administered orally or topically per rectum or immune-suppressing medications such as oral thiopurine agents and systemically delivered biologic agents such as anti-TNF antibodies,2 and more recently the anti-α4β7 integrin antibody, vedolizumab.3 Despite the availability of these therapies, treatment may be ineffective for many patients, and particularly systemically delivered immune-suppressing agents are associated with serious infections and other adverse effects. Additional therapies with novel mechanisms and improved safety profiles are needed.
Sirtuins (also called silent information regulator 2 [Sir2] proteins) are a class of proteins with important biological functions in organisms ranging from prokaryotes to eukaryotes.4 They are NAD+-dependent deacetylases, with numerous well-defined substrates, that may play a role in a number of different diseases.5–7 The mammalian sirtuins include a family of 7 recognized members, designated as SIRT1 through SIRT7,4 and are implicated in various physiological roles in metabolism and inflammation.8,9 SIRT1 is best known for its role as a mediator in extending longevity through calorie restriction (CR),10–12 but varieties of other beneficial metabolic and anti-inflammatory effects have been demonstrated.13–17 Resveratrol, a component of red wine, is an SIRT1 activator, and has been shown to have metabolic and anti-inflammatory benefits, as well as an anticancer effect, and in addition may inhibit ischemic injury.18–28 However, resveratrol is not a highly potent nor selective SIRT1 activator and, therefore, a variety of more potent SIRT1 activators have been developed to explore their potential therapeutic effect in diseases of aging and inflammation.29
To explore the effects of SIRT1 activation in UC, we assessed the safety, tolerability, colonic tissue exposure, and anti-inflammatory effects of 2 different doses of SRT2104, a SIRT1 activator, in subjects with mild to moderate UC.
MATERIALS AND METHODS
Study Subjects
Men and women aged 18 to 75 with mild to moderately active UC as evidenced by Mayo score1 6 to 10 (inclusive) with rectal bleeding score >1, endoscopy score between 2 and 3 (inclusive), and physician's rating of disease activity <3 at day 5 were enrolled. Subjects had confirmed diagnosis of UC for at least 3 months before the screening visit and colonic inflammation extending proximal to the rectum (ie, >15 cm in extent) on baseline sigmoidoscopy at day 5. Subjects with infectious colitis as evidenced by positive stool culture for enteric pathogens or positive stool Clostridium difficile cytotoxin assay at visit 1 were excluded, and other significant medical disorders (respiratory, cardiovascular, renal or liver impairment, or hemoglobin less than 8.5 g/dL at visit 1) were excluded, as were subjects with flat or unresected raised colonic dysplasia. Treatment with oral aminosalicylates at doses ≤4.8 g per day was permitted if they were begun at least 4 weeks before study day 5. Rectal aminosalicylates at any dose within 2 weeks of study day 5, systemic or rectal corticosteroids within 4 weeks of study day 5, TNFα inhibitors or other biologics within 2 months before study day 5, or thiopurine agents initiated within 3 months before study day 5, or if changed in terms of dose within 3 months before study day 5 were not permitted. Previous participation in a clinical trial and treatment with a study drug within 3 months before visit 1 was also an exclusion factor.
Study Design
This study was conducted as a parallel group randomized, double-blind, study using 2 doses of SRT2104 (50 and 500 mg) at 13 centers in the United States. The first subject visit occurred on February 13, 2012, and the final visit on March 18, 2013. The clinical research was reviewed and approved by GSKs internal review panels and by both regional and local institutional review boards for each participating study site.
There was a screening period, an 8-week treatment period with 3 on-treatment visits (days 1, 28, and 56), and a follow-up visit (day 70), and phone follow-ups on days 14 and 42 to assess adverse events (AEs), as well as to complete the Simple Clinical Colitis Activity Index (SCCAI) score30 and the partial Mayo score.31
Eligible subjects were randomized in a 1:1 ratio at visit 2 (day 5) to either 50 mg or 500 mg SRT2104 according to a computer-generated randomization schedule with no stratification; investigators and evaluators were blinded to treatment assignment factors.
Subjects received SRT2104 by mouth once daily from day 1 through day 56 (8 weeks). AEs were monitored from visit 2 (day 5) through the follow-up visit (day 70). Physical examinations findings, vital signs, clinical laboratory results (hematology, chemistry, urinalysis), and electrocardiograms were assessed at periodic intervals through day 70 and reviewed by an Internal Safety Review Committee. Two flexible sigmoidoscopies and colon biopsies were performed, 1 on day 5 (±2 days), before randomization, and 1 on day 56, to assess tissue levels of SRT2104, changes in UC histopathology scores and effects of SRT2104 on histologic markers of inflammation. Endoscopic scoring of UC lesions and the Mayo score were also assessed at both time points. Histopathologic specimens were paired for each subject and were analyzed by an independent pathologist who was blinded to dose of SRT2104 and to the time point the specimen was obtained (i.e., pre- or post-study drug exposure). Similarly, endoscopies were recorded; paired recordings were interpreted by an independent assessor who was blinded to the dose administered and time point. The SCCAI score and partial Mayo score were conducted at all study visits to evaluate the effect of SRT2104 on clinical signs and symptoms of UC. Blood was obtained on day 56 for the assessment of SRT2104 concentration.
Subjects who prematurely discontinued from the study completed day 56 assessments at the time of discontinuation pending discussion with the medical monitor. All subjects, including those who discontinued early, were asked to return for a safety follow-up visit approximately 14 days after their last visit.
Study Evaluations
The primary clinical end points were colonic exposure levels, safety, and tolerability. Safety evaluations were based on the incidence, severity, and type of AEs and clinically significant changes in the subject's vital signs, electrocardiogram, and clinical laboratory results during the course of the study. Safety variables were listed by treatment group, 50 mg or 500 mg SRT2104. SRT2104 drug levels as measured in colonic tissue samples were a key primary end point apart from safety and tolerability assessments. The secondary end points included response and complete remission rates based on changes in endoscopic assessment scores from baseline (day 5) to day 56, response and complete remission rates based on Mayo scores and partial Mayo scores from baseline (day 5) to day 56, mean change in Mayo scores, response and complete remission rates based on changes in SCCAI scores from baseline (day 5) to days, 28, and 56, mean changes in SCCAI sores, changes in fecal calprotectin from visit 1 to day 56, and changes in histopathologic scores from baseline (day 5) to day 56. In addition, a blood sample was collected on day 56 at the time of colon biopsy for the assessment of SRT2104 plasma concentration. Exploratory end points included biomarker changes in tissue from day 5 to day 56. Colon tissue samples were collected for exploratory biomarkers including, but not limited to, gene expression and cytokines. Blood was collected for exploratory biomarkers including, but not limited to, various proinflammatory cytokines. Exposure to study drug and reasons for discontinuation of study treatment were tabulated. In addition, the proportion of subjects who achieved response or remissions was tabulated. Exact methods were used to calculate response proportions and their confidence intervals (CIs). Change from baseline in Mayo and SCCAI scores were analyzed using a mixed model and included corresponding baseline score as covariate, subject as random effect, and treatment arm as a fixed effect. The mean change from baseline, difference between treatment groups, and the 90% CI of the difference were estimated.
Sample Size
The primary focus of this study was to evaluate the safety, tolerability, and colonic tissue exposure in subjects with mild to moderate UC. Therefore, a formal sample size determination was not performed. Approximately, 24 subjects were planned for this study. Twelve subjects per arm would produce a 92% CI plus or minus 23% points when the response proportion is 60%. Also, with a sample size of 12 subjects per arm, the probability of observing at least 1 AE of a given type is 85.8% when the actual probability of this given AE is 15%.
Statistical Analysis
The safety data were summarized and listed by treatment group; for the pharmacokinetic data, the plasma and colon tissue concentrations were listed by treatment group and descriptively summarized without statistical analyses. For the clinical activity/pharmacodynamic analyses, no formal hypothesis was tested. The proportion of subjects who achieved response or remission based on the Mayo, endoscopy (independent assessment) and SCCAI scorings32 were tabulated with a 95% CI.
Mean change from baseline/percent change from baseline to day 56 for Mayo, histology (Geboes),33 and SCCAI scores were summarized descriptively by treatment group. Similarly, a change in fecal calprotectin from day 1 (day 21 to 4) to day 56 was descriptively summarized by treatment group and visit. A Mayo score response was defined as a reduction from baseline in Mayo score of either ≥3 and a 30% reduction from baseline and either a decrease in rectal bleeding subscore of ≥1 or an absolute rectal bleeding score ≤1. A Mayo score remission was defined as Mayo score ≤2 and no subscore >1. An endoscopic response was defined as reduction from baseline in endoscopy score ≥1. An endoscopic remission was defined as an endoscopy score 0. SCCAI clinical response was defined as a reduction from baseline in SCCAI score ≥2 and clinical remission was defined as an SCCAI score ≤3.
The change from baseline and differences between treatment arms in Mayo and SCCAI scores were analyzed using a mixed model and included corresponding baseline score as covariate, subject as random effect, and treatment arm as a fixed effect. The mean change from baseline in histology, Mayo, and SCCAI at day 56 were estimated. A similar analysis was performed to compare the endoscopic score/Mayo score by the central reviewer against what the on-site investigator recorded. Distributional assumptions underlying the statistical analyses were assessed by visual inspection of residual plots. Normality was examined by normal probability plots, whereas homogeneity of variance was assessed by plotting the residuals against the predicted values for the model. The proportion of subjects who fell into different category within each item with respect to Mayo/SCCAI/histology scales was summarized by treatment and visit.
Biomarker analyses the changes in tissue biomarkers from day 5 to day 56 were summarized using descriptive statistics. Raw data change from baseline for blood biomarker end points were summarized descriptively, graphically presented, and listed by visit and each treatment group.
For gene expression microarray analysis, the colon samples obtained on day 5 and day 56 were hybridized to Affymetrix GeneChip HG-U133A-v2 and differential gene expression analysis and cluster analysis were performed.
Ethical Conduct of the Study
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki (version October, 2008) and the relevant regulations under 21 CFR parts 312, 50, and 56. A signed informed consent was obtained from each patient before performing any study related procedures. The study protocol and ICF were approved by institutional review boards of each participating study site. The first subject visited on February 13, 2012, and the last subject visit was March 18, 2013 (clinicaltrials.gov NCT01453491).
RESULTS
A total of 56 subjects were screened of which 24 did not meet entry criteria, the remaining 32 subjects were randomized and 31 received study medication during this study (Fig. 1; Tables 1 and 2).
FIGURE 1.
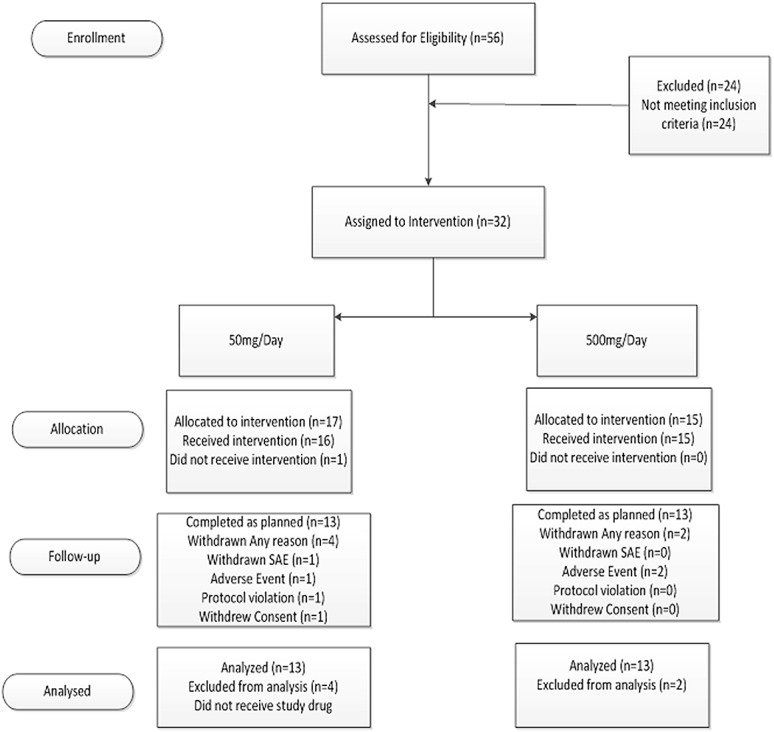
Consort diagram. One subject was excluded from analysis in the 50 mg/d group due to a major protocol violation.
TABLE 1.
Demographics, Baseline Characteristics, and Disease Activity
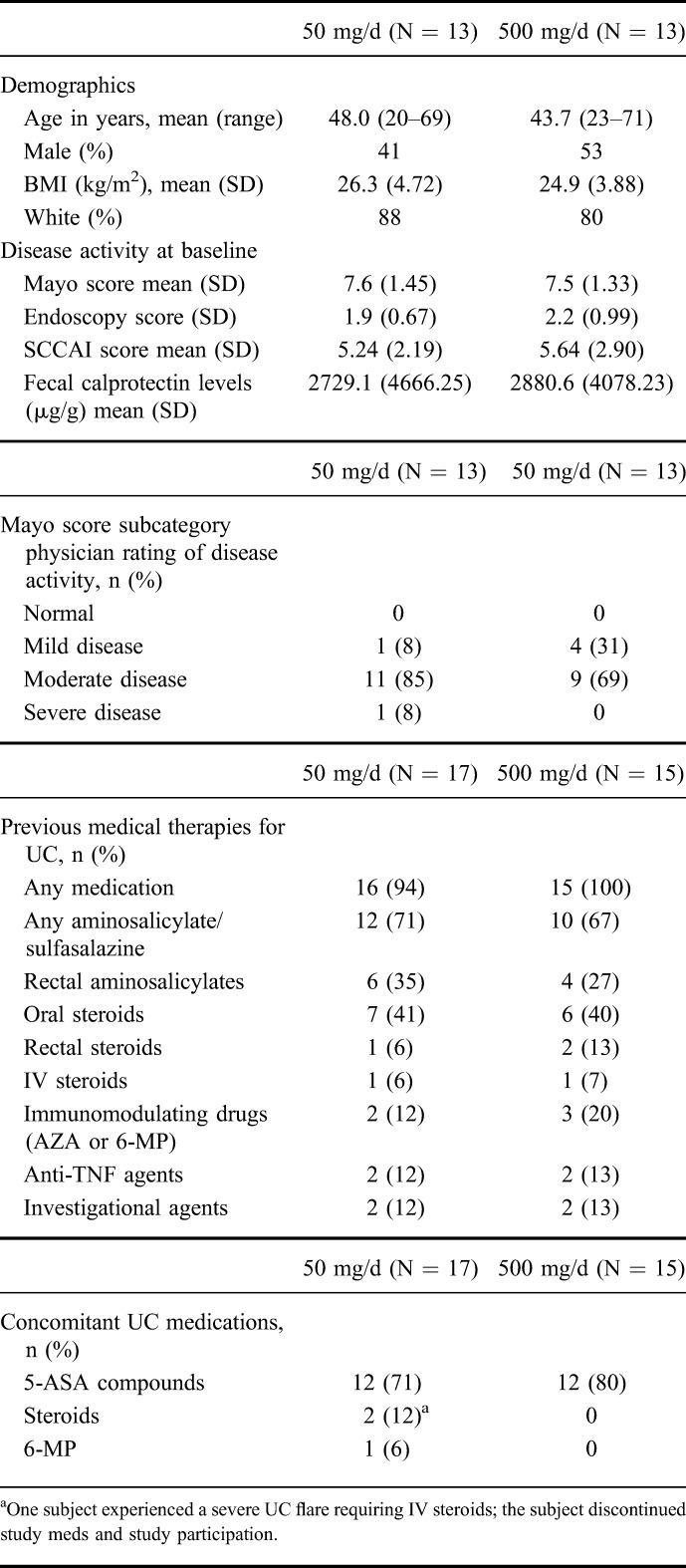
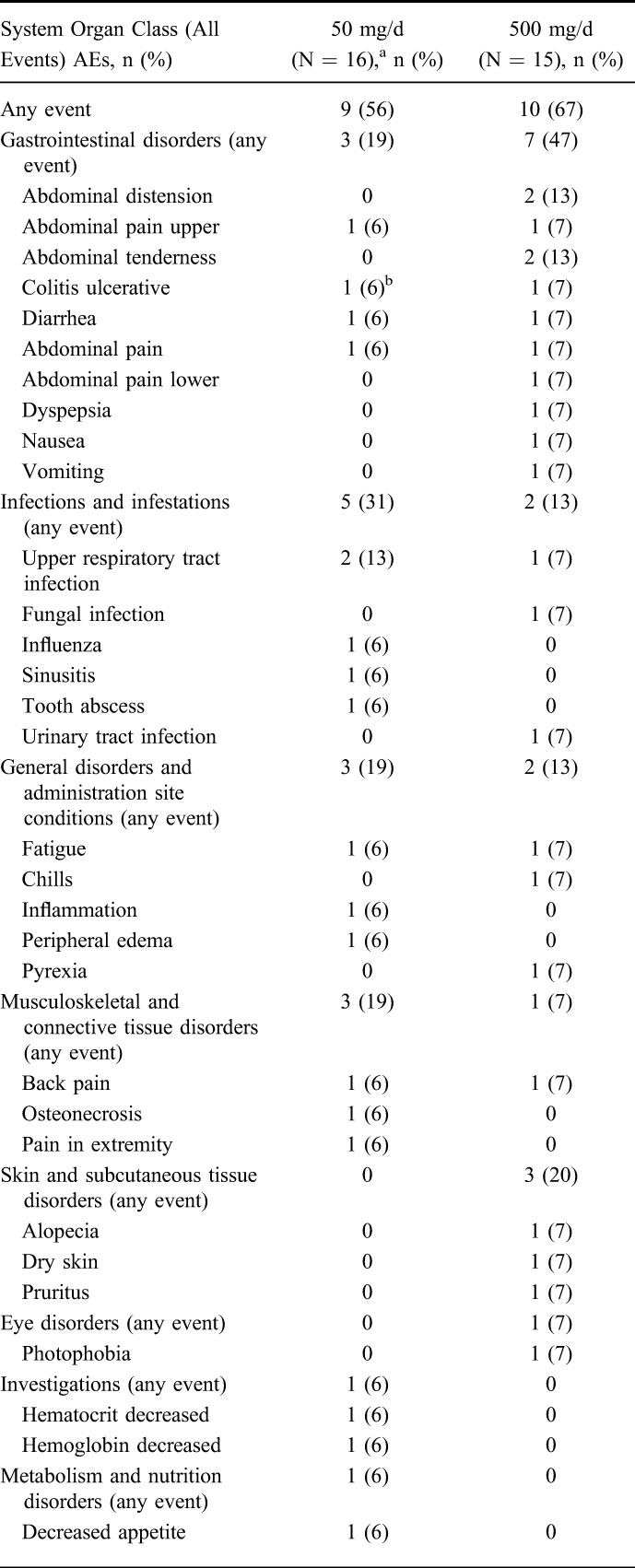
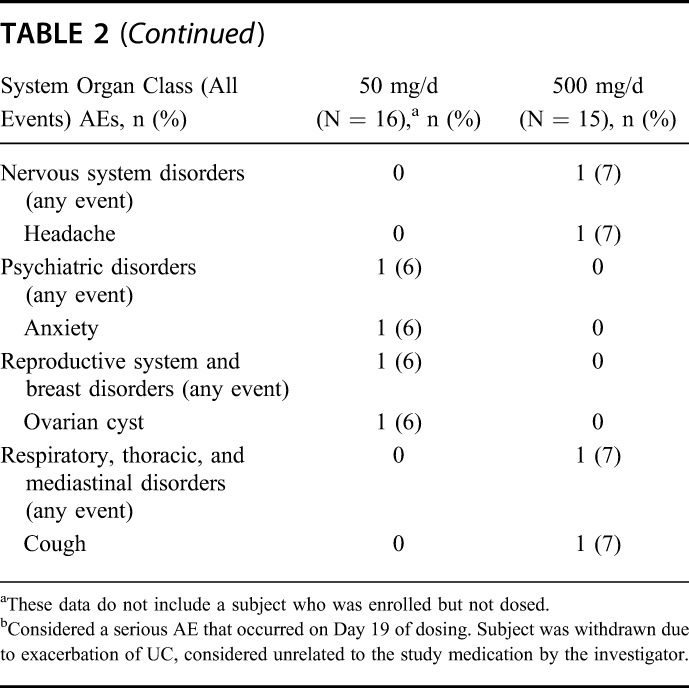
TABLE 2.
Summary of Number of Subjects Reporting AEs (Safety Population)
Safety Results
Overall, the frequency of subjects reporting any AE was similar between the 50 mg and 500 mg groups; however, there were proportionately more subjects with gastrointestinal AEs in the 500 mg group. Except for 2 cases of severe UC, all other AEs were mild to moderate in intensity. One subject in the 50 mg/d group was withdrawn due to a severe UC on day 19 that was considered serious but unrelated to the study medication by the investigator. This SAE was reported as resolving at study completion. One subject in the 500 mg/d was reported with a severe flare of UC, but not an SAE, resulting in withdrawal, which was reported as resolved at study completion.
In total, 4 subjects were withdrawn due to AEs. In addition to a subject withdrawn for UC, 1 subject in the 50 mg group was withdrawn on day 1 for abdominal pain upper (related) and fatigue (related) and another in the 500 mg was withdrawn on day 2 for photophobia (related-day 1), diarrhea (related-day 2), and headache (unrelated-day 2).
There were no clinically significant findings in the clinical laboratory values, vital signs, and electrocardiograms. There were isolated abnormal values in clinical chemistry and hematology laboratory values, but none was considered clinically significant.
Pharmacokinetic Results
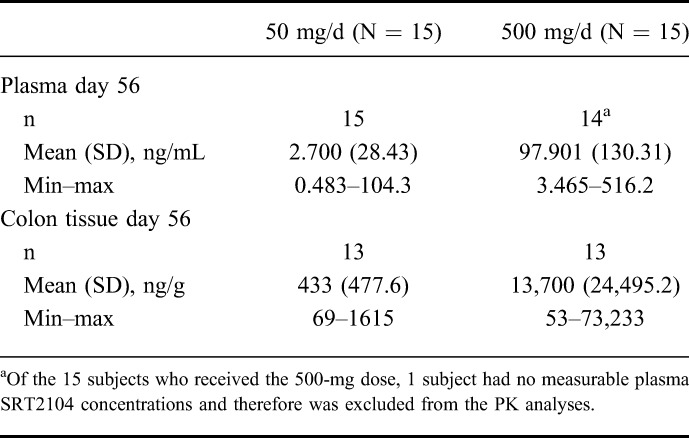
Plasma and colon tissue concentrations of SRT2104 for day 56 are summarized in Table 3. The colonic tissue concentrations of SRT2104 achieved were approximately 140 to 160-fold the concentrations achieved in the plasma. In addition, there were dose-related increases in both the plasma and tissue concentrations when comparing 50 mg/d with 500 mg/d groups.
TABLE 3.
Summary of Plasma and Colon Tissue SRT2104 Concentration–Time Data
Clinical Activity/Pharmacodynamic Results
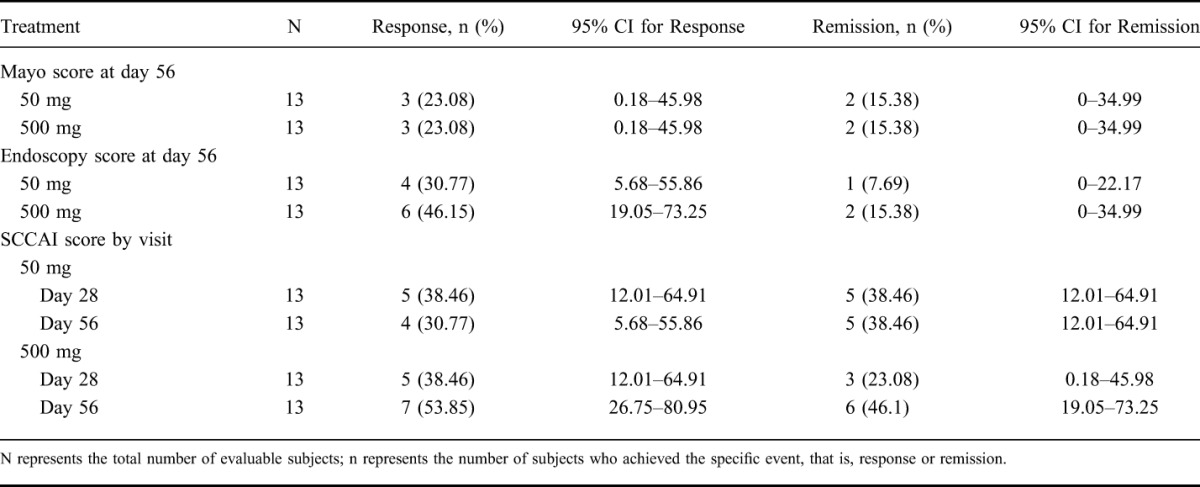
The rates of remission and clinical response were low at both doses of SRT2104 administered based on the following assessment scores on day 56: Mayo, SCCAI, and endoscopy scores (4). Anti-inflammatory potential of SRT2104 was also not demonstrated based on histopathological scoring of colonic tissue biopsies.
A comparison of baseline and week 8 of cytokines were measured from repeated serial colon biopsies. The changes for the 50 and 500 mg/d during the treatment interval revealed changes, which were highly variable, and therefore their clinical significance was unclear (data not shown).
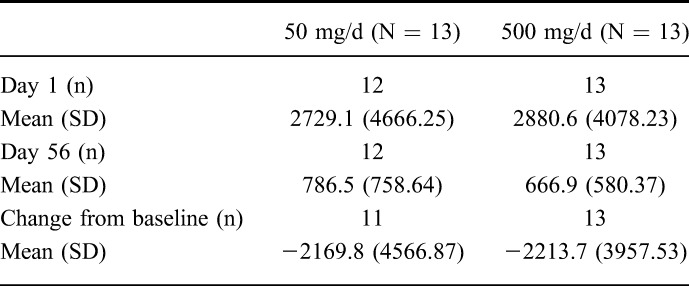
With respect to fecal calprotectin, changes in levels of measured biomarkers demonstrated reductions in both treatment groups (Table 4). Baseline values of fecal calprotectin were comparable in both groups, a reduction was noted in fecal calprotectin levels from baseline to day 56 values in both treatment groups, and overall there was slightly larger decline in the 500 mg/d group compared with the 50 mg/d group. But at day 56, fecal calprotectin levels were still elevated relative to normal.
TABLE 4.
Summary of Fecal Calprotectin by Study Day (Microgram/Gram)
Gene Expression Analysis Results
After QC analysis and preprocessing, a total of 33 microarray samples remained from 22 patients with day 5, day 56 data, or both were analyzed. No statistically significant gene expression changes were observed for day 5, day 56 comparisons, or for high-dose versus low-dose treatment comparisons. Cluster analysis of the top most variable genes (i.e., unbiased list of differentially regulated genes) showed significant enrichment of immune response–related biological pathways and processes, such as inflammatory response, cytokine activity, and leukocyte chemotaxis. Together, these results suggest relatively high heterogeneity between patient samples that precludes any conclusive findings. When limiting the analysis to samples from the 6 patients who responded to either treatment, a total of 36 genes had significantly altered expression levels (at least 2-fold upregulation or downregulation and unadjusted P value <5%). Of these, 5 genes were downregulated posttreatment and 31 were upregulated. The top downregulated genes include FOSB and GBP1. The topmost upregulated genes include DEFA6, HMGCS2, TM4SF20, UGT1A8, and DPP4. Because of the low number of samples, these results require further validation.
DISCUSSION
One novel therapeutic approach to treating inflammatory bowel disease and other diseases of inflammation has come from the study of aging and CR. CR is a dietary regimen in which 30%–40% fewer calories than those required to maintain ideal body weight are consumed. It has been demonstrated that CR extends lifespan in lower organisms and mammals and improves a number of metabolic and inflammatory parameters.10–12 As such, the molecular components of the aging pathways downstream of CR may provide relevant intervention points for the development of therapeutic drugs to treat inflammatory and metabolic disease.8,9
SIRT1 is a member of the sirtuin family of NAD+-dependent deacetylases.5–7 There are seven human sirtuins (SIRT1–7) with different subcellular compartmentalization and downstream targets.4 SIRT1 is predominantly nuclear and is upregulated in tissues of calorically restricted animals.34 The precise biological pathway whereby SIRT1 promotes the beneficial effects of CR is an area of intense study, but it seems that the ability of SIRT1 to interact and deacetylate PGC-1α is an important component.35 PGC-1α controls energy metabolism and muscle function with an inhibitory role in proinflammatory cytokine production36 and has been implicated as a key mediator of the effects of CR.37 In addition, a number of other cellular substrates for SIRT1 have been identified, including NCoR, p300, NFκβ, FOXO, and p53.13,15,17,35,38–43 For example, SIRT1 has been shown to physically interact with and deacetylate the RelA/p65 subunit of NFκβ, and thereby inhibit NFκβ-induced transcription,43 which is involved in upregulation of proinflammatory cytokines such as TNF-α and IL-6. Furthermore, SIRT1 activators have been shown to inhibit TNF-α secretion in both in vitro14,44 and in vivo (Sirtris unpublished data) lipopolysaccharide (LPS)-induced cellular and animal models. A recent study of SRT2104 (a selective SIRT1 activator) in a human endotoxemia model of inflammation supports the preclinical findings. SRT2104 demonstrated an anti-inflammatory signal in this model, suppressing a number of cytokines and activation of coagulation in response to LPS administration45 compared with placebo control. Through modulation of the activities of a number of proteins, SIRT1 regulates inflammation, cellular differentiation and survival, mitochondrial biogenesis, and glucose metabolism.11,15,34,46
SRT2104 is a potent and selective small molecule activator of SIRT1. SIRT1 is known to deacetylate numerous substrates including the rel/p65 component of NFkB. Through deacetylation of this substrate, NFkB transcriptional activity is reduced, and thus there is a reduction in proinflammatory cytokine production. This is 1 mechanism whereby an SIRT1 activator, such as SRT2104, may exhibit anti-inflammatory activity. SRT2104 has been shown to be effective in vitro and in vivo in preclinical inflammatory studies, suppressing cytokine production in response to LPS and reducing disease activity in animal models including the DSS and TNBS models of IBD. In addition, SRT2104 was shown to reduce cytokine production in human volunteers in response to LPS administration. This earlier study confirmed the anti-inflammatory activity of SRT2104 in humans and supported studying the potential therapeutic use of SRT2104 in chronic inflammatory disorders such as UC. SRT2104, despite poor pharmacokinetics, also showed benefit in moderate to severe psoriasis patients treated for 12 weeks.47
In this clinical trial, overall SRT2104 was well tolerated, with the majority of study subjects completing the 8 weeks of treatment. The plasma exposures in UC patients are within the expected ranges (Table 3) when compared with previous experience in healthy volunteers29 but are low and with very high inter subject variability. Colon tissue concentrations achieved were 140- to 160-fold plasma concentrations (Table 3). The response and remission rates based on Mayo score, endoscopy score by a blinded central reader, and the SCCAI scores (Table 5) reveal, in general, no dose–response relationship and overall a disappointing clinical effect. Preclinical data with SRT2104 in animal models of UC had suggested that SRT2104 would have a primarily local effect in the colon with little systemic exposure. The data presented here suggest that this is not the case in patients with UC and that an effect on circulating leukocytes may be necessary. This is further evidenced by the modest response with respect to changes in fecal calprotectin, as fecal calprotectin levels were approximately 4-fold higher than the normal values after SRT2104 treatment. Normalization of fecal calprotectin can be achieved when highly effective therapies are used to treat UC.48 In addition, the multiple cytokines measured from colon biopsy specimens revealed no clear and meaningful trends. Similarly, no conclusive findings were identified from the genetic expression analysis. The absence of a signal identified by the blinded central reader on endoscopy provides for no rationale for the continued development of SRT2104 in patients with UC. A limitation of this study was the absence of a placebo arm, a purposeful decision which was taken to facilitate patient recruitment. The decision unfortunately precludes evaluation of the magnitude of responses to SRT2104 relative to placebo responses. Thus, we are left to make comparisons of all measured responses compared with average historical responses, not taking into account placebo response rates.
TABLE 5.
Summary of Remission and Clinical Response
CONCLUSIONS
The SIRT1 activator SRT2104 was well tolerated in a population of UC patients at doses of 50 and 500 mg/d, but the clinical response was disappointing and does not support any further development of SRT2104 in patients with UC.
ACKNOWLEDGMENTS
The authors acknowledge the investigators Dr. Ian Baird, Dr. Charles Barish, Dr. Ronald Fogel, Dr. Lev Ginzburg, Dr. Robert Hardi, Dr. Kevin Kuettel, Dr. Philip Miner, Dr. Mark Noar, and Dr. Salam Zakko. All listed authors meet the criteria for authorship set forth by the International Committee for Medical Journal Editors.
Author contributions: Conceived and designed the experiments, B. E. Sands, E. Hoffmann, E. Jacobson; analyzed the data, B. E. Sands, S. Joshi, J. Haddad, J. M. Freudenberg, E. Hoffmann, S. W. McCallum, and E. Jacobson; wrote the article, B. E. Sands, S. Joshi, J. Haddad, J. M. Freudenberg, E. Hoffmann, S. W. McCallum, and E. Jacobson; oversight of the clinical study, B. E. Sands, D. E. Oommen, and E. Jacobson; interim review of data, S. Joshi, J. Haddad, D. E. Oommen, E. Hoffmann, and E. Jacobson.
Footnotes
Funding for this study was provided by GlaxoSmithKline (NCT01453491).
S. Joshi, J. Haddad, J. M. Freudenberg, and S. W. McCallum are GSK employees and shareholders. D. E. Oommen, E. Hoffmann, and E. Jacobson were employees of GSK at the time this research was conducted. The remaining author has no conflict of interest to disclose.
REFERENCES
- 1.Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987;317:1625–1629. [DOI] [PubMed] [Google Scholar]
- 2.Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353:2462–2476. [DOI] [PubMed] [Google Scholar]
- 3.Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369:699–710. [DOI] [PubMed] [Google Scholar]
- 4.Blander G, Guarente L. The Sir2 family of protein deacetylases. Annu Rev Biochem. 2004;73:417–435. [DOI] [PubMed] [Google Scholar]
- 5.Imai S, Armstrong CM, Kaeberlein M, et al. Transcriptional silencing and longevity protein Sir2 is an NAD-dependent histone deacetylase. Nature. 2000;403:795–800. [DOI] [PubMed] [Google Scholar]
- 6.Frye RA. Phylogenetic classification of prokaryotic and eukaryotic Sir2-like proteins. Biochem Biophys Res Commun. 2000;273:793–798. [DOI] [PubMed] [Google Scholar]
- 7.Frye RA. Characterization of five human cDNAs with homology to the yeast SIR2 gene: Sir2-like proteins (sirtuins) metabolize NAD and may have protein ADP-ribosyltransferase activity. Biochem Biophys Res Commun. 1999;260:273–279. [DOI] [PubMed] [Google Scholar]
- 8.Weindruch R, Keenan KP, Carney JM, et al. Caloric restriction mimetics: metabolic interventions. J Gerontol A Biol Sci Med Sci. 2001;56:20–33. Spec No 1. [DOI] [PubMed] [Google Scholar]
- 9.Ingram DK, Zhu M, Mamczarz J, et al. Calorie restriction mimetics: an emerging research field. Aging Cell. 2006;5:97–108. [DOI] [PubMed] [Google Scholar]
- 10.Fontana L. The scientific basis of caloric restriction leading to longer life. Curr Opin Gastroenterol. 2009;25:144–150. [DOI] [PubMed] [Google Scholar]
- 11.Heilbronn LK, Ravussin E. Calorie restriction and aging: review of the literature and implications for studies in humans. Am J Clin Nutr. 2003;78:361–369. [DOI] [PubMed] [Google Scholar]
- 12.Roth GS, Ingram DK, Lane MA. Caloric restriction in primates and relevance to humans. Ann N Y Acad Sci. 2001;928:305–315. [DOI] [PubMed] [Google Scholar]
- 13.Nemoto S, Fergusson MM, Finkel T. SIRT1 functionally interacts with the metabolic regulator and transcriptional coactivator PGC-1{alpha}. J Biol Chem. 2005;280:16456–16460. [DOI] [PubMed] [Google Scholar]
- 14.Yoshizaki T, Schenk S, Imamura T, et al. SIRT1 inhibits inflammatory pathways in macrophages and modulates insulin sensitivity. Am J Physiol Endocrinol Metab. 2010;298:E419–E428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Picard F, Kurtev M, Chung N, et al. Sirt1 promotes fat mobilization in white adipocytes by repressing PPAR-gamma. Nature. 2004;429:771–776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Milne JC, Lambert PD, Schenk S, et al. Small molecule activators of SIRT1 as therapeutics for the treatment of type 2 diabetes. Nature. 2007;450:712–716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Brunet A, Sweeney LB, Sturgil JF, et al. Stress-dependent regulation of FOXO transcription factors by the SIRT1 deacetylase. Science. 2004;303:2011–2015. [DOI] [PubMed] [Google Scholar]
- 18.Gu XS, Wang ZB, Ye Z, et al. Resveratrol, an activator of SIRT1, upregulates AMPK and improves cardiac function in heart failure. Genet Mol Res. 2014;13:323–335. [DOI] [PubMed] [Google Scholar]
- 19.Sharma S, Misra CS, Arumugam S, et al. Antidiabetic activity of resveratrol, a known SIRT1 activator in a genetic model for type-2 diabetes. Phytother Res. 2011;25:67–73. [DOI] [PubMed] [Google Scholar]
- 20.Yu W, Wan Z, Qiu XF, et al. Resveratrol, an activator of SIRT1, restores erectile function in streptozotocin-induced diabetic rats. Asian J Androl. 2013;15:646–651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dong W, Zhang X, Gao D, et al. Cerebral angiogenesis induced by resveratrol contributes to relieve cerebral ischemic-reperfusion injury. Med Hypotheses. 2007;69:226–227. [DOI] [PubMed] [Google Scholar]
- 22.Juhasz B, Das DK, Kertesz A, et al. Reduction of blood cholesterol and ischemic injury in the hypercholesteromic rabbits with modified resveratrol, longevinex. [corrected]. Mol Cell Biochem. 2011;348:199–203. [DOI] [PubMed] [Google Scholar]
- 23.Li C, Yan Z, Yang J, et al. Neuroprotective effects of resveratrol on ischemic injury mediated by modulating the release of neurotransmitter and neuromodulator in rats. Neurochem Int. 2010;56:495–500. [DOI] [PubMed] [Google Scholar]
- 24.Li H, Yan Z, Zhu J, et al. Neuroprotective effects of resveratrol on ischemic injury mediated by improving brain energy metabolism and alleviating oxidative stress in rats. Neuropharmacology. 2011;60:252–258. [DOI] [PubMed] [Google Scholar]
- 25.Liu XQ, Wu BJ, Pan WH, et al. Resveratrol mitigates rat retinal ischemic injury: the roles of matrix metalloproteinase-9, inducible nitric oxide, and heme oxygenase-1. J Ocul Pharmacol Ther. 2013;29:33–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ren J, Fac C, Chen N, et al. Resveratrol pretreatment attenuates cerebral ischemic injury by upregulating expression of transcription factor Nrf2 and HO-1 in rats. Neurochem Res. 2011;36:2352–2362. [DOI] [PubMed] [Google Scholar]
- 27.Vin AP, Hu H, Zhai Y, et al. Neuroprotective effect of resveratrol prophylaxis on experimental retinal ischemic injury. Exp Eye Res. 2013;108:72–75. [DOI] [PubMed] [Google Scholar]
- 28.Wang Q, Xu J, Rottinghaus GE, et al. Resveratrol protects against global cerebral ischemic injury in gerbils. Brain Res. 2002;958:439–447. [DOI] [PubMed] [Google Scholar]
- 29.Hoffmann E, Wald J, Lavu S, et al. Pharmacokinetics and tolerability of SRT2104, a first-in-class small molecule activator of SIRT1, after single and repeated oral administration in man. Br J Clin Pharmacol. 2013;75:186–196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Walmsley RS, Ayres RC, Pounder RE, et al. A simple clinical colitis activity index. Gut. 1998;43:29–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lewis JD, Chuai S, Nessel L, et al. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm Bowel Dis. 2008;14:1660–1666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Higgins PD, Schwartz M, Mapili J, et al. Patient defined dichotomous end points for remission and clinical improvement in ulcerative colitis. Gut. 2005;54:782–788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Geboes K, Riddell R, Ost A, et al. A reproducible grading scale for histological assessment of inflammation in ulcerative colitis. Gut. 2000;47:404–409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cohen HY, Miller C, Bitterman KJ, et al. Calorie restriction promotes mammalian cell survival by inducing the SIRT1 deacetylase. Science. 2004;305:390–392. [DOI] [PubMed] [Google Scholar]
- 35.Rodgers JT, Lerin C, Haas W, et al. Nutrient control of glucose homeostasis through a complex of PGC-1alpha and SIRT1. Nature. 2005;434:113–118. [DOI] [PubMed] [Google Scholar]
- 36.Handschin C, Spiegelman BM. The role of exercise and PGC1alpha in inflammation and chronic disease. Nature. 2008;454:463–469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Corton JC, Brown-Borg HM. Peroxisome proliferator-activated receptor gamma coactivator 1 in caloric restriction and other models of longevity. J Gerontol A Biol Sci Med Sci. 2005;60:1494–1509. [DOI] [PubMed] [Google Scholar]
- 38.Bouras T, Fu M, Sauve AA, et al. SIRT1 deacetylation and repression of p300 involves lysine residues 1020/1024 within the cell cycle regulatory domain 1. J Biol Chem. 2005;280:10264–10276. [DOI] [PubMed] [Google Scholar]
- 39.Luo J, Nikolaev AY, Imai S, et al. Negative control of p53 by Sir2alpha promotes cell survival under stress. Cell. 2001;107:137–148. [DOI] [PubMed] [Google Scholar]
- 40.Motta MC, Divecha N, Lemieux M, et al. Mammalian SIRT1 represses forkhead transcription factors. Cell. 2004;116:551–563. [DOI] [PubMed] [Google Scholar]
- 41.van der Horst A, Tertoolen LG, de Vries-Smits LM, et al. FOXO4 is acetylated upon peroxide stress and deacetylated by the longevity protein hSir2(SIRT1). J Biol Chem. 2004;279:28873–28879. [DOI] [PubMed] [Google Scholar]
- 42.Vaziri H, Dessain SK, Ng Eaton E, et al. hSIR2(SIRT1) functions as an NAD-dependent p53 deacetylase. Cell. 2001;107:149–159. [DOI] [PubMed] [Google Scholar]
- 43.Yeung F, Hoberg JE, Ramsey CS, et al. Modulation of NF-kappaB-dependent transcription and cell survival by the SIRT1 deacetylase. EMBO J. 2004;23:2369–2380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Smith JJ, Kenney RD, Gagne DJ, et al. Small molecule activators of SIRT1 replicate signaling pathways triggered by calorie restriction in vivo. BMC Syst Biol. 2009;3:31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.van der Meer A, et al. The first demonstration of clinical activity by a small molecule sirt1 activator: srt2104 reduces cytokine release and coagulation activation in a human endotoxemia model. In: Inflammation Research. Basel, Switzerland: Birkhauser Aerlag AG Viadukstrasse; 2011:40–44. [Google Scholar]
- 46.Nisoli E, Tonella C, Cardile A, et al. Calorie restriction promotes mitochondrial biogenesis by inducing the expression of eNOS. Science. 2005;310:314–317. [DOI] [PubMed] [Google Scholar]
- 47.Jacobson EW, Suárez-Fariñas M, Cueto I, et al. 12 weeks of treatment with an oral SIRT1 activator, SRT2104, leads to clinical improvement and skin microarray modification in patients with psoriasis. J Invest Dermatol. 2013;133(suppl):159. [Google Scholar]
- 48.Smith LA, Gaya DR. Utility of faecal calprotectin analysis in adult inflammatory bowel disease. World J Gastroenterol. 2012;18:6782–6789. [DOI] [PMC free article] [PubMed] [Google Scholar]