
Figure 1.
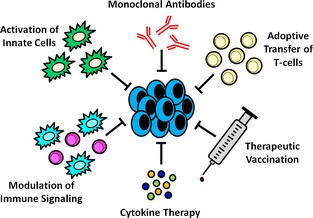
General categories of antitumor immunotherapy (clockwise from top). Monoclonal antibodies (mAbs) can be used directly against tumor cells or targeted towards the tumor microenvironment. Direct killing of tumor cells via mAbs is typically through receptor antagonist or agonist activity, but can also target enzymatic activities within the tumor cells. Conjugation of cytotoxic drugs to mAbs is another mechanism of direct tumor killing. These mechanisms can also be applied to the tumor microenvironment. Enhanced immune‐mediated killing of tumor cells can also be harnessed through mAbs via enhancement of phagocytosis, antibody‐dependent cellular cytotoxicity (ADCC), complement activation, or T‐cell cross‐presentation and activation. Adoptive transfer of T‐cells specific for certain tumor cell antigens can enhance antitumor immunity. T‐cells can be genetically engineered to express T‐cell receptors that recognize specific tumor cell antigens or tumor‐specific autologous T‐cells can be isolated from the tumor itself with subsequent expansion and reinfusion into the host for the exertion of therapeutic activities. Therapeutic vaccination is aimed at redirecting or enhancing immune responses to tumors. Some therapeutic vaccines employ ex vivo expansion of autologous antigen‐presenting cells (APC) with a common tumor antigen or focus on the modification of tumor cells to express or secrete cytokines that enhance APC activation; in both situations these cells are reinfused into the patient. Other therapeutic vaccines focus on delivery of a specific protein that is overexpressed by the tumor of interest or serves a specific immune function, delivery of an infectious agent to enhance general antitumor immunity, or a combination thereof. Cytokine therapies, such as IL‐2 or the interferons, can be used in vivo to enhance immune responses, but can also be employed in the ex vivo expansion of immune cells for cell‐based therapies. Modulation of immune signaling with agents such as BCG and muramyl peptides refers to enhancement of beneficial antitumor immune responses or blockade of immunosuppressive signaling. Manipulation of tumor cells to express costimulatory molecules can enhance immune activation, while blockade of inhibitory immune cells (such as Tregs or MDSCs) or inhibitory immune receptors (such as CTLA‐4) can prevent tumor‐based immunosuppression. Activation of innate immune cells, such as dendritic cells, can be achieved through ex vivo cytokine activation, in vivo treatment with toll‐like receptor (TLR) ligands or targeted antigen‐loaded antibodies, or even occur naturally secondary to tumor cell death from radiation therapy or chemotherapy.