

Abstract
Cases of vascular anomalies of the iliac and femoral vessels are rare. We report a complete absence of the right common iliac artery in a 21-year-old woman, incidentally discovered by CT during the work-up for acute abdominal pain. A network of prominent collateral arteries reconstituted the distal portion of the right external iliac artery and the common femoral artery, forming the arterial supply of the right lower limb. Multiple collaterals were also observed reconstituting the right internal iliac artery. At the time of presentation, the patient had no signs or symptoms to suggest lower extremity ischemia, however this may become a problem in the future. Recognition of vascular abnormalities can dictate extra caution when planning abdominal surgery.
Abbreviations: CT, computed tomography
Introduction
Vascular malformations involving the iliac and femoral vessels are far more rare than those involving the thoracic and abdominal aorta and may be discovered incidentally or during the work-up for lower extremity ischemia. The exact prevalence of iliofemoral anomalies is unknown, but Greeb identified no more than 6 cases by angiography in a series of 8000 symptomatic patients [1]. Among the vascular anomalies involving the iliac and femoral arteries, aplasia associated with persistent sciatic artery or atresia with residual cord has often been described [2, 3, 4, 5, 6]. In the case of a persistent sciatic artery, there is a high prevalence of aneurysms and arteriosclerosis [7]. Other cases involve hypoplasia of the iliofemoral artery and are also associated with occlusive symptoms due to associated atherosclerosis [8, 9]. In addition, complex genitourinary malformations are sometimes associated with these anomalies [3, 10].
Complete absence of the common iliac artery specifically is an extremely rare anomaly. Mansfield and Howard showed the autopsy specimen of a patient with congenital bilateral absence of the common iliac arteries. In that case, the aorta divided directly into two internal iliac arteries and two external iliac arteries [11]. Dumanian presented a case report of a 44-year-old man with long standing bilateral intermittent claudication secondary to congenital absence of the left common iliac and both external and common femoral arteries [4]. More recently, Llauger described congenital absence of a right common iliac vessel in an asymptomatic patient in whom the blood supply to the right pelvis and the right lower extremity derived from an anomalous vessel originating from the left hypogastric artery [12].
Oduro exemplified the clinical importance of early recognition of several of these malformations in a patient whose blood supply to the left lower extremity arose from an anomalous external iliac artery that branched from the left renal artery. Unfortunately, in that case, the anomaly was not identified until the patient presented with left lower limb claudication following an elective left nephrectomy during which time the anomalous vessel was inadvertently tied off [13].
More recently, Harb et al. described a case of congenital absence of the bilateral internal iliac arteries that was incidentally noted at the time of surgery of a ruptured mycotic abdominal aortic aneurysm. In that case, prominent lumbar arteries compensating for the absent internal iliac arteries bilaterally were noted [14]. Koyama et al. reported a patient with absence of the left external iliac artery. In that case, a well-developed left internal iliac artery appeared to be continuous with the left common femoral artery, thus providing blood supply to the lower extremity [15].
Case Report
A 21-year-old woman with no significant past medical history, including an uneventful c-section two months prior, presented to the emergency room with crampy lower abdominal pain. She was menstruating and noted that her last bowel movement was three days prior and consisted of well-formed brown stool. She denied hematochezia, melena, fever, chills, nausea and vomiting. There was no history of prior trauma or instrumentation of the iliac arteries in this patient. Laboratory studies were unremarkable. Pelvic ultrasound to evaluate for gynecological causes of abdominal pain was unremarkable. CT scan performed to further evaluate the patient's abdominal pain showed a left common iliac artery with well-developed internal and external branches. However, the aorta appeared to end abruptly at the point where the right common iliac would be expected to originate (Figure 1A, Figure 1B, Figure 1C, Figure 1D). Multiple lumbar and retroperitoneal collaterals reconstituted the right internal iliac artery (Figure 1B, Figure 1C, Figure 1D).
Figure 1A.
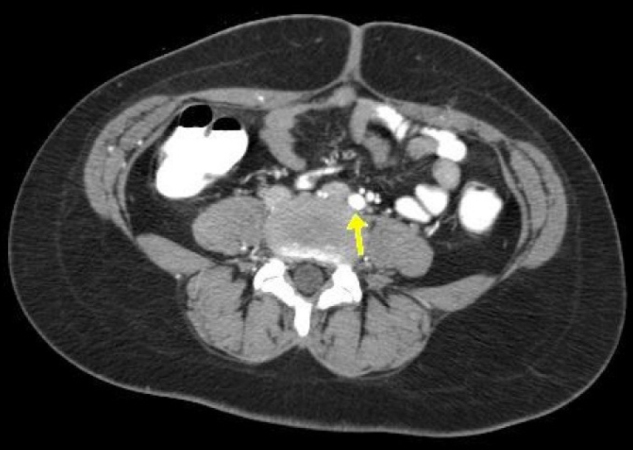
Contrast-enhanced axial CT. The absence of the right common iliac artery is presented. The left common iliac artery (arrow) is visualized.
Figure 1B.

The left internal (green arrow) and external (red arrow) iliac arteries are also seen. Retroperitoneal collaterals (yellow arrow) reconstitute the right internal iliac artery.
Figure 1C.

Lumbar collaterals (arrow) also reconstituted the right internal iliac artery.
Figure 1D.
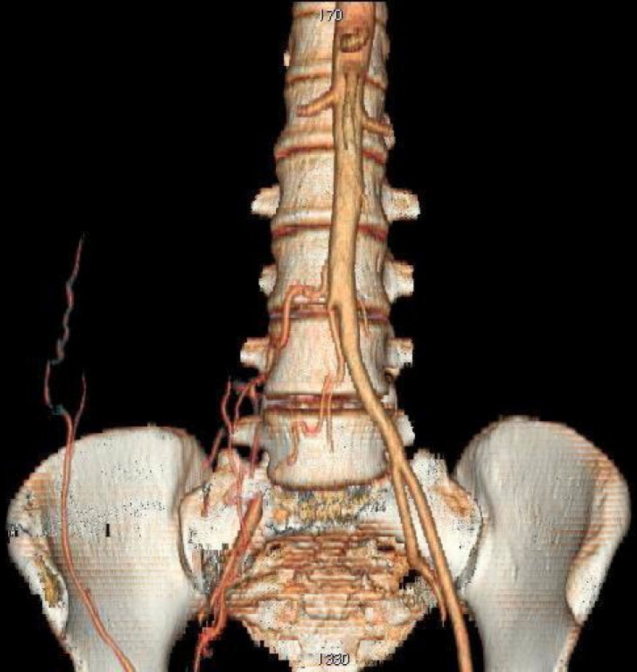
3-D surface-rendered image of CT data summarizes these findings.
The proximal portion of the external iliac artery was not visualized. The distal portion and the right common femoral artery were reconstituted from the right inferior epigastric artery, deep circumflex iliac artery and the contralateral common femoral artery (Figure 2A, Figure 2B, Figure 2C). A retroaortic left renal vein was also noted. There was no evidence on CT for atherosclerotic disease or acute abdominal process. Upon further questioning, the patient denied a history of lower extremity pain or any limitation to activities such as running or prolonged walking due to pain or fatigue.
Figure 2A.
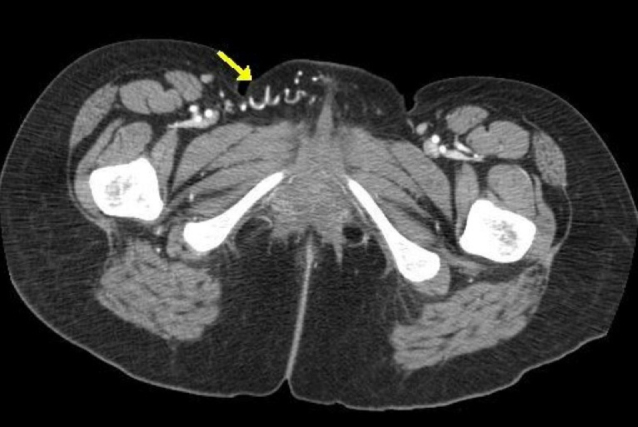
Contrast-enhanced axial CT shows tortuous collateral vessels on the right (arrow).
Figure 2B.

These vessels originated from the contralateral femoral artery and are seen emerging from the left (arrows).
Figure 2C.
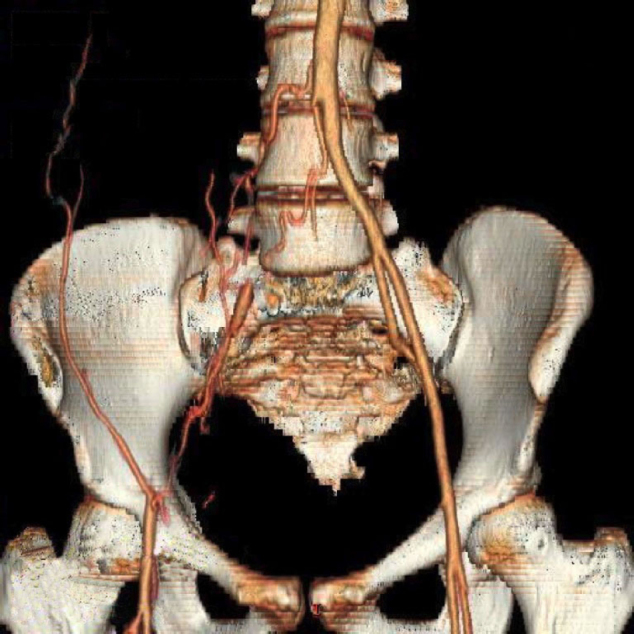
3-D surface-rendered image of CT data shows the distal portion of the right external iliac artery and the right common femoral artery reconstituting from the right inferior epigastric artery, deep circumflex iliac artery and the contralateral common femoral artery.
Examination of lower extremities showed no evidence of asymmetry or muscular hypotrophy or atrophy. Extremities were warm with normal coloration. The lower extremity pulses were palpable bilaterally. Although no specific etiology could be attributed to the patient's abdominal pain, it is unlikely that it was related to the incidental vascular malformation discovered on CT.
Discussion
The sciatic artery is the main artery of the lower extremity in the early embryo. It arises dorsally from the umbilical artery, and as development proceeds, it retreats as the ventral branch of the umbilical artery forms the external iliac and femoral arteries. Parts of the sciatic artery persist however as the inferior gluteal, popliteal and peroneal arteries. The initial segment of the umbilical artery becomes the common iliac artery [16]. It is likely that the absence of the right common iliac artery observed in our patient is congenital in nature, given the prominence of the collateral vessels.
Leriche described a syndrome that includes fatigue, pain throughout the lower extremities appearing after exercise, pallor of the legs on elevation, absent or weak pulses in the lower extremities and impotence. The primary etiological agent for this syndrome is atherosclerotic involvement of the aortic bifurcation [17]. Although both occlusive disease of the terminal aorta and congenital absence of the iliac arteries can both present with claudication, there are some differences. In particular, with iliac artery atresia, impotence is not characteristic and the thigh and hips are spared from ischemic symptoms. Some authors have argued that while congenital absence of the iliac arteries is rare, it should be included in the differential diagnosis for intermittent claudication of the legs [4, 18]. This case is most likely congenital given the presence of prominent collateral vessels. Furthermore, there is no history of prior instrumentation or trauma to the iliac arteries to suggest traumatic thrombus formation. It is unlikely that the imaging findings are due to fibromuscular dysplasia. Although, this is more common in younger patients, fibromuscular dyplasia often has a beaded appearance on imaging. Furthermore, all other vascular segments were normal in appearance. Fibromuscular dyplasia tend to involve more than one vascular segment [19].
The renal arteries and the abdominal aorta were normal in our patient. A retroaortic left renal vein was seen, which represents a common variation. In addition, our patient appeared to have well developed collateral vessels that continue to provide adequate blood flow to her lower extremities. Although she is currently asymptomatic, absence of the right common iliac artery may pose a problem in the future in the setting of atherosclerosis and thrombosis or if the collateral vessels are inadvertently disrupted by abdominal surgery for unrelated symptoms.
Footnotes
Published: January 13, 2008
Contributor Information
Donnette A. Dabydeen, Email: ddabydeen@partners.org.
Anatoli Shabashov, Email: ashabashov@challiance.org.
Kitt Shaffer, Email: kshaffer@challiance.org.
References
- 1.Greebe J. Congenital anomalies of the iliofemoral artery. J Cardiovasc Surg. 1977 May-Jun;18(3):317–323. [PubMed] [PubMed] [Google Scholar]
- 2.Howard JM, Goudelock WJ, Couves CM. Congenital atresia of the external iliac artery. Arch Surg. 1957 Aug;75(2):296–299. doi: 10.1001/archsurg.1957.01280140134025. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Appleberg M. Congenital atresia of the external iliac artery. S Afr Med J. 1975 Oct 25;49(45):1885–1886. [PubMed] [PubMed] [Google Scholar]
- 4.Dumanian AV, Frahm CJ, Benchik FA, Wooden TF. Intermittent claudication secondary to congenital absence of iliac arteries. Arch Surg. 1965 Oct;91(4):604–606. doi: 10.1001/archsurg.1965.01320160058013. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Williams LR, Flanigan DP, O'Connor RJ, Schuler JJ. Persistent sciatic artery. Clinical aspects and operative management. Am J Surg. 1983 May;145(5):687–693. doi: 10.1016/0002-9610(83)90122-8. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Martin KW, Hyde GL, McCready RA, Hull DA. Sciatic artery aneurysms: report of three cases and review of the literature. J Vasc Surg. 1986 Oct;4(4):365–371. [PubMed] [PubMed] [Google Scholar]
- 7.McLellan GL, Morettin LB. Persistent sciatic artery: clinical, surgical, and angiographic aspects. Arch Surg. 1982 Jun;117(6):817–822. doi: 10.1001/archsurg.1982.01380300057013. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.DeLaurentis DA, Friedman P, Wolferth CC, Jr, Wilson A, Naide D. Atherosclerosis and the hypoplastic aortoiliac system. Surgery. 1978 Jan;83(1):27–37. [PubMed] [PubMed] [Google Scholar]
- 9.Seghezzi R, Rossi G, Chierichetti F, Lovotti M, Salvini M. A case of congenital hypoplasia of the right external iliac artery. J Cardiovasc Surg. 1991 Nov-Dec;32(6):775–777. [PubMed] [PubMed] [Google Scholar]
- 10.Saalfeld J, Walsh PC, Goodwin WE. Ureterovaginoplasty for vaginal atresia (unique technique in treatment): a case report with description of associated arterial anomalies and retroiliac artery ureters. J Urol. 1973 Jun;109(6):1039–1045. doi: 10.1016/s0022-5347(17)60619-0. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Mansfield AO, Howard JM. Absence of both common iliac arteries. A Case report. Anat Rec. 1964 Dec;150:363–364. doi: 10.1002/ar.1091500404. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Llauger J, Sabate JM, Guardia E, Escudero J. Congenital absence of the right common iliac artery: CT and angiographic demonstration. Eur J Radiol. 1995 Dec 15;21(2):128–130. doi: 10.1016/0720-048x(95)00701-q. [PubMed] [DOI] [PubMed] [Google Scholar]
- 13.Oduro GD, Cope LH, Rogers IM. Case report: lower limb arterial blood supply arising from the renal artery with congenital absence of the ipsilateral iliac arteries. Clin Radiol. 1992 Mar;45(3):215–217. doi: 10.1016/s0009-9260(05)80649-x. [PubMed] [DOI] [PubMed] [Google Scholar]
- 14.Harb Z, William S, Rutter P. Bilateral congenital absence of internal iliac arteries, prominent lumbar arteries, and a ruptured mycotic aneurysm of the abdominal aorta. Ann R Coll Surg Engl. 2006 Jul;88(4):W3–W5. doi: 10.1308/147870806X95285. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Koyama T, Kawada T, Kitanaka Y, Katagiri K, Ohno M, Ikeshita M, Yamate N. Congenital anomaly of the external iliac artery: a case report. J Vasc Surg. 2003 Mar;37(3):683–685. doi: 10.1067/mva.2003.102. [PubMed] [DOI] [PubMed] [Google Scholar]
- 16.Senior HD. The development of the arteries of the human lower extremities. Am J Anat. 1919;25:55–95. [Google Scholar]
- 17.Leriche R, Morel A. Syndrome of Thrombotic Obliteration of Aortic Bifurcation. Ann Surg. 1948;127(1):193–206. doi: 10.1097/00000658-194802000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Narverud G, Myhre HO. Congenital hypoplasia of the lower limb arteries. A report of two cases. Scand J Thorac Cardiovasc Surg. 1974;8:70–72. doi: 10.3109/14017437409129066. [PubMed] [DOI] [PubMed] [Google Scholar]
- 19.Lüscher TF, Keller HM, Imhof HG, Greminger P, Kuhlmann U, Largiader F, Schneider E, Schneider J, Vetter W. Fibromuscular hyperplasia: extension of the disease and therapeutic outcome. Results of the University Hospital Zurich Cooperative Study on Fibromuscular Hyperplasia. Nephron. 1986;44(Suppl 1):109–114. doi: 10.1159/000184059. [PubMed] [DOI] [PubMed] [Google Scholar]