

Abstract
We report a case of an 11-year-old patient who underwent CT imaging for complications of sinusitis, and showed incidental development of an interhemispheric cyst in association with an intracranial lipoma over a 10-year interval. Cysts and lipomas are well described in association with dysgenesis of the corpus callosum. We present an uncommon association, of a new cyst in association with an intracranial lipoma, in a patient with a normal corpus callosum.
Abbreviations: MRI, magnetic resonance imaging; CT, computed tomography
Introduction
Intracranial lipomas are congenital, non-neoplastic lesions that may be an incidental finding on CT or MR imaging. The most common theory regarding their etiology points to abnormal persistence and differentiation of the meninx primitiva during embryology. The most common associated finding with intracranial lipomas is partial or complete agenesis of the corpus callosum; dysgenesis of other portions of the brain is a less commonly reported phenomenon. A few reports in the literature have also documented obstructive hydrocephalus in association with lipomas of the quadrigeminal plate cistern and ambient cistern. We present the following case as an uncommon phenomenon, the development of an interhemispheric cyst adjacent to a lipoma.
Case report
An 11-year-old male child presented to the Emergency Department with left periorbital swelling and pain. A contrast-enhanced CT of the sinuses and head revealed pansinus disease with a subperiosteal abscess along the medial left orbital wall (Fig. 1, arrow). Adjacent to the falx, there was a bilobed, fluid-density structure that measured 4.7 cm × 4 cm in greatest transaxial dimensions (Fig. 2A), without any rim enhancement. Incidental note was made of a linear midline fat-density structure along the falx, adjacent to the cyst, with extension to the right trigonal choroid plexus (Figs. 2B-C, arrows). A remote comparison MR image that had been obtained for focal alopecia 10 years before demonstrated the interhemispheric lipoma (Fig. 3A, arrow), without any associated fluid collection (Fig. 3B, arrow). The remote MR image had also demonstrated a normal corpus callosum (Fig. 3A).
Figure 1.

11-year-old male with interhemispheric lipoma. Axial postcontrast CT image shows left ethmoid opacities and a thin, rim-enhancing fluid collection along the lamina papyracea of the medial left orbit, consistent with a subperiosteal abscess (arrow).
Fig. 2.

11-year-old male with interhemispheric lipoma. Axial postcontrast CT images obtained at a level superior to the lateral ventricles (A at standard brain window, and B at expanded windows at levels) show a fluid-density, bilobed simple cyst along the falx, without rim enhancement, and without obvious extension into the lateral ventricles. There is a lipoma associated with the cyst (B, arrow) that extends from the right atrium of the lateral ventricle (C, arrow), adjacent to the choroid, to superiorly along the falx.
Figure 3.
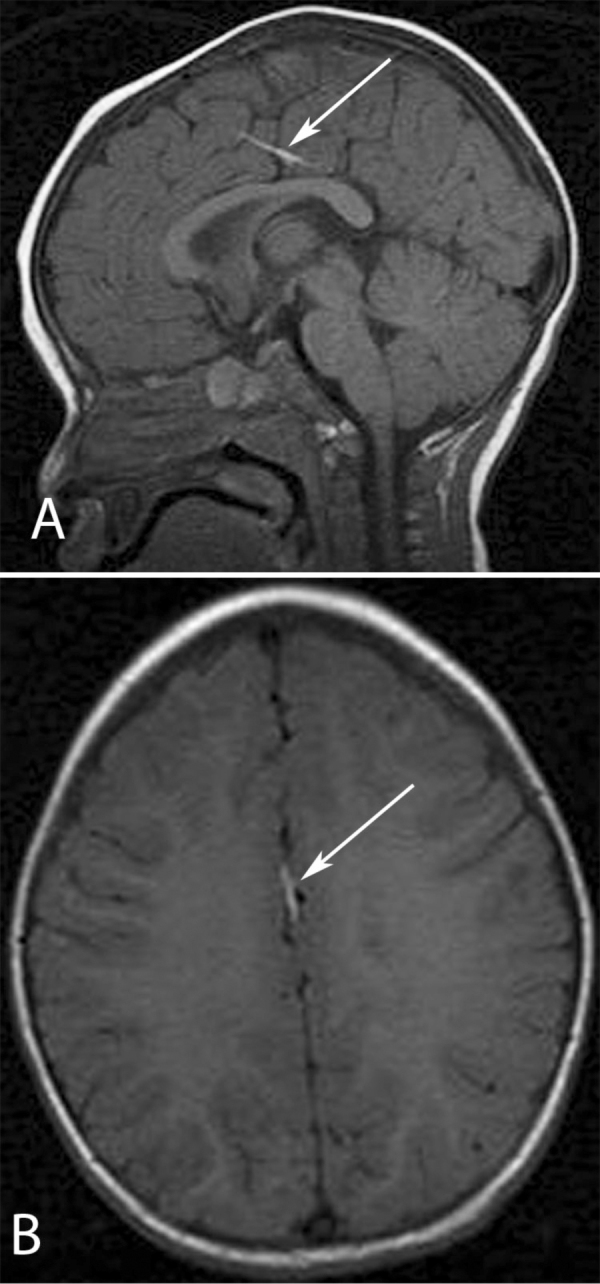
11-year-old male with interhemispheric lipoma. Midline, sagittal, T1-weighted image (A) from an MRI obtained 10 years before demonstrates a normal-appearing corpus callosum and a high-signal intensity band, consistent with an intracranial lipoma. Axial T1-weighted image (B) above the level of the corpus callosum, at approximately the level of the CT images shown in Figs. 2A-B, shows no cyst.
The patient was admitted to the hospital and successfully treated for the sinusitis and subperiosteal abscess with intravenous antibiotics, with an unremarkable hospital course. A followup visit with the otolaryngology consultant nine days after presentation documented near-resolution of his symptoms. A subsequent visit eight months after presentation demonstrated no abnormal neurological symptoms
Discussion
Intracranial lipomas are generally regarded as incidental findings that in themselves are typically of negligible clinical significance. They are of congenital origin (1), rarely are symptomatic, and typically are nonoperatively managed (2). Rarely, they may cause obstructive hydrocephalus (3, 4, 5, 6). In addition, they may be seen in association with other, potentially symptomatic, conditions such as partial or complete agenesis of the corpus callosum (1, 7) and intracranial aneurysm (8, 9). Dysgenesis of the corpus callosum is the most commonly associated finding in patients with an intracranial lipoma (1). We present our case of the interval formation of an interhemispheric cyst in a patient with an intracranial lipoma as an unreported associated finding.
The entities associated with intracranial lipomas may be static, such as callosal dysgenesis. Alternatively, associated abnormalities are potentially dynamic, such as intracranial aneurysms and, as in our case, cysts. In our presented case, the presence of a new interhemispheric cystic mass was confounded by the patient’s presenting illness of sinusitis. The absence of abnormal enhancement of the cyst walls and brain parenchyma, and the lack of parenchymal edema or mass effect, helped to eliminate a complication of sinusitis (that is, intracranial abscess) from the differential diagnosis (10).
Cysts have been well documented in association with callosal agenesis (11). The appearance of a new cyst has also previously been reported with agenesis of the corpus callosum (12). To our knowledge, a new cyst has not been reported with an intracranial lipoma. Despite the size of the intracranial cyst, the patient remained asymptomatic with respect to the cyst at an 8-month followup examination. Given the development and growth of the cyst over a 10-year interval, however, it is possible that the lesion could become symptomatic if growth continues. Thus, the cyst may require future imaging and/or intervention.
The etiology of the cyst is uncertain. We favor an arachnoid cyst over a ependymal or neurenteric cyst, due to the location and simple-fluid density. The pathophysiology causing its growth is similarly unclear. It is possible that the pathophysiology is similar to those proposed in the expansion of arachnoid cysts, including a ball-valve phenomenon, osmotic gradients between the cyst and CSF spaces, or fluid production by the cells lining the cyst walls (13). Obstruction of the ventricular system has been attributed to lipomas of the quadrigeminal plate (3), quadrigeminal plate cistern (4), choroid plexus (5), and ambient cistern (6) in previous case reports. In our case, it seems unlikely that the growth of the cyst is directly related to obstruction of the ventricular system, given that the cyst is remote from the ventricular system.
In summary, this case suggests that intracranial lipomas may be associated with new and potentially dynamic cysts. While intracranial lipomas in themselves are nonoperative lesions, the growth of an associated cyst raises the potential necessity of future imaging and intervention, should clinical symptoms develop.
Footnotes
Published: July 12, 2011
References
- 1.Truwit CL, Barkovich AJ. Pathogenesis of intracranial lipoma: an MR study in 42 patients. AJR. 1990 Oct;155(4):855–864. doi: 10.2214/ajr.155.4.2119122. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Yilmaz N, Unal O, Kiymaz N, Yilmaz C, Etlik O. Intracranial lipomas—a clinical study. Clin Neurol Neurosurg. 2006 Jun;108(4):363–368. doi: 10.1016/j.clineuro.2005.04.003. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Halmagyi GM, Evans WA. Lipoma of the quadrigeminal plate causing progressive obstructive hydrocephalus. Case report. J Neurosurg. 1978 Sep;49(3):453–456. doi: 10.3171/jns.1978.49.3.0453. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.Kawamata T, Aoki N, Sakai T, Takakura K. Congenital triventricular hydrocephalus associated with a small lipoma in the quadrigeminal plate cistern. Childs Nerv Syst. 1995 Feb;11(2):121–123. doi: 10.1007/BF00303819. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Kazner E, Stochdorph O, Wende S, Grumme T. Intracranial lipoma: diagnostic and therapeutic considerations. J Neurosurg. 1980 Feb;52(2):234–245. doi: 10.3171/jns.1980.52.2.0234. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Maiuri F, Corriero G, Gallicchio B, Simonetti L. Lipoma of the ambient cistern causing obstructive hydrocephalus. J Neurosurg Sci. 1987 Apr-Jun;31(2):53–58. [PubMed] [PubMed] [Google Scholar]
- 7.Kieslich M, Ehlers S, Bollinger M, Jacobi G. Midline developmental anomalies with lipomas in the corpus callosum region. J Child Neurol. 2000 Feb;15(2):85–89. doi: 10.1177/088307380001500205. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Futami K, Kimura A, Yamashita J. Intracranial lipoma associated with cerebral saccular aneurysm. Case Report. J Neurosurg. 1992 Oct;77(4):640–642. doi: 10.3171/jns.1992.77.4.0640. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.Yamamoto M, Kuwabara S, Uozumi T. Lipoma of the corpus callosum associated with distal anterior cerebral artery aneurysm. A case report. Hiroshima J Med Sci. 1989 Sep;38(3):157–160. [PubMed] [PubMed] [Google Scholar]
- 10.Reid JR. Complications of pediatric paranasal sinusitis. Pediatr Radiol. 2004 Dec;34(12):933–942. doi: 10.1007/s00247-004-1252-2. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Barkovich AJ, Simon EM, Walsh CA. Callosal agenesis with cyst: A better understanding and new classification. Neurology. 2001 Jan 23;56(2):220–227. doi: 10.1212/wnl.56.2.220. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Stroustrup Smith A, Levine D. Appearance of an interhemispheric cyst associated with agenesis of the corpus callosum. AJNR. Am J Neuroradiol. 2004 Jun-Jul;25(6):1037–1040. [PubMed] [PMC free article] [PubMed] [Google Scholar]
- 13.Gosalakkal JA. Intracranial arachnoid cysts in children: A review of pathogenesis, clinical features, and management. Pediatr Neurol. 2002 Feb;26(2):93–98. doi: 10.1016/s0887-8994(01)00329-0. [PubMed] [DOI] [PubMed] [Google Scholar]