

Abstract
Background:
Sylvian dissection is an essential microneurosurgical skill for neurosurgeons. The safe and accurate opening of the sylvian fissure is desirable for a good prognosis.
Methods:
The aim of this report is to demonstrate the use of indocyanine green (ICG) videoangiography to recognize the superficial sylvian vein (SSV) and thus enable a wide opening of the sylvian fissure, especially in patients with subarachnoid hemorrhage (SAH).
Results:
The small tributary flowing into the SSV was distinguishable from a passing one, which deeply entered the insula. In addition, an entering point of a tributary to the SSV, which ran perpendicular to the insula, was occasionally determined. SSV, which was barely discernable in a reddish SAH involving the sylvian fissure, was clearly demarcated using ICG videoangiography. Two representative cases of sylvian dissection are herein presented.
Conclusion:
The performance of ICG videoangiography before sylvian dissection is a simple and useful method for identifying a vital approach route for safe and accurate sylvian dissection, and it reduces the risk of causing any accidental injury to the veins in the sylvian fissure.
Keywords: Distal sylvian dissection, indocyanine green videoangiography, superficial sylvian vein
INTRODUCTION
Sylvian dissection is a mandatory skill for exposing the insula and reaching the deep areas of the brain in vascular and neoplastic surgery. The many variations of the sylvian veins consist of superficial and deep sylvian veins, which are three-dimensionally anastomosed with the tributaries from the frontal, temporal, parietal lobes, and the insula.[2,6] The superficial sylvian vein (SSV) is located on the surface of the sylvian fissure, which is like an entrance into the deep brain area. The sacrifice of the tributaries when entering SSV may potentially cause a catastrophic venous infarction. SSV enters many tributaries from the frontal and temporal lobes and occasionally becomes a severe gatekeeper by blocking access to the deep region. The techniques that are required to mobilize SSV and its tributaries have been described in previous studies.[3,7] However, an SSV that is buried in a subarachnoid hemorrhage (SAH) may be difficult to recognize before sylvian dissection. In microsurgery, indocyanine green (ICG) videoangiography is frequently used to provide arterial information;[4,5] however, a few studies have applied ICG to the venous system.[1,8] The detection of the running course of the SSV may help reduce the incidence of accidental injuries of SSV, especially in SAH patients. This is the first report to describe the utilization of ICG for demarcation of the SSV in a distal transsylvian approach.
MATERIALS AND METHODS
After a dural incision, an injection of ICG (5 mg) (Daiichi Sankyo Co., Ltd., Tokyo, Japan) and bolus saline (20 ml) was observed through an FL800 system mounted on a Leica OH-4 microscope (Leica Microsystems GmbH, Wetzlar, Germany).
RESULTS
A tributary flowing into SSV was distinguished from one which passed the SSV [Figure 1a, Video 1a]. If the sylvian fissure was loose, the small vein which arose from the insula and connected to SSV was observed [Figure 1b, Video 1b]. According to a patient with SAH, a thick SAH was observed in the operative field before the sylvian dissection. The demarcation of the SSV was vague in the reddish SAH, and it was difficult to recognize its location and running course. After the administration of ICG, the branches of the middle cerebral arteries (MCAs) were easily distinguished in the early phase and the location of the sylvian fissure was recognized. Subsequently, SSV and its tributaries were observed at the late phase to find the venous pattern of SSV bridging between the frontal and temporal lobes.
Figure 1.
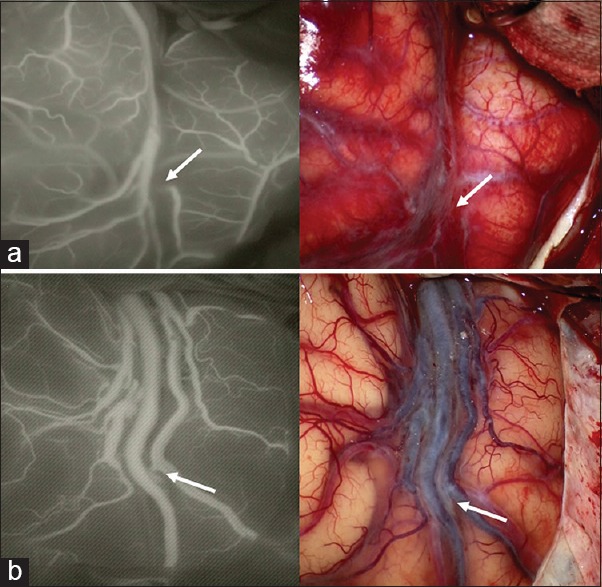
(a) Indocyanine green videoangiography demonstrated that a temporosylvian vein (arrow) is recognized to pass by the superficial sylvian vein, and not to flow into it. (b) Insular veins (arrow), which deeply appeared from the insula, are observed to enter each frontal and temporal superficial sylvian vein. These insular veins were barely detectable without indocyanine green videoangiography. The arrows show the same positions of the veins
We herein present two representative cases of patients with SAH. Patient 1 showed a thick SAH with a ruptured MCA bifurcation aneurysm [Figure 2, Video 2]. It was not possible to visualize SSV or the MCA branches due to SAH and the swelling of the patient's brain. ICG videoangiography disclosed the location of the sylvian fissure and venous drainage pattern. SSV, which was undeveloped in the distal sylvian fissure, bridged from the frontal to the temporal lobe in the proximal sylvian fissure. The hypoplasticity of SSV had caused the distal sylvian fissure to adhere to the pia mater. To achieve a wide sylvian opening, it was necessary to completely skeletonize the proximal SSV from the temporal lobe.
Figure 2.
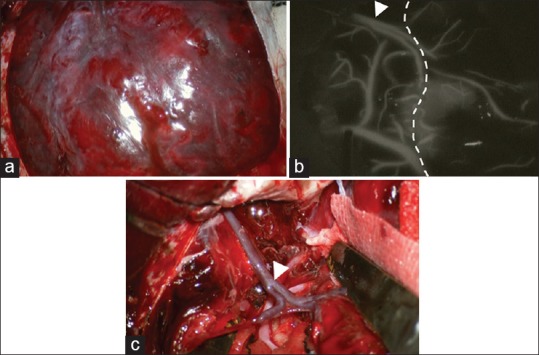
(a) The bulging and reddish brain appearance of the surface with the subarachnoid hemorrhage after the dural incision. (b) Indocyanine green videoangiography. The sylvian fissure (dotted line) is estimated from the branches of the middle cerebral artery. The superficial sylvian vein is clearly identified after the administration of indocyanine green. The frontosylvian and temporosylvian veins empty into the superficial sylvian vein (arrowhead) and flow toward the temporal lobe. (c) A wide sylvian opening is obtained after the skeletonization of the superficial sylvian vein (arrowhead) from the temporal lobe. The arrowheads show the same positions of the superficial sylvian vein
Patient 2 had a ruptured internal carotid-posterior communicating artery aneurysm with a hypoplastic SSV at the proximal sylvian fissure [Figure 3]. SSV was expected to move to the frontal side because there were no tributaries from the temporal lobe. In addition, the dissection from the frontal side was added in the distal sylvian fissure to skeletonize SSV because the temporal dissection risked causing a contusion of the temporal lobe due to the long distance between SSV and sylvian fissure. In both patients, these inevitabilities were predicted by ICG videoangiography before the sylvian dissection.
Figure 3.
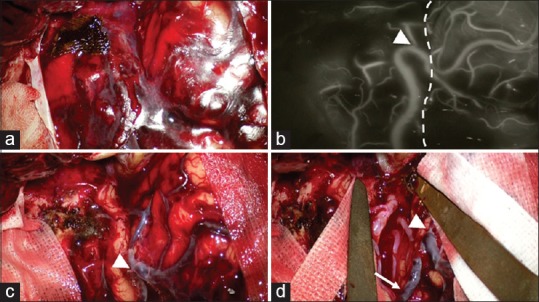
(a) The brain surface with the subarachnoid hemorrhage. (b) The locations of the superficial sylvian vein (arrowhead) and the sylvian fissure (dotted line) as visualized by indocyanine green videoangiography. No tributaries from the temporal lobe enter the superficial sylvian vein. (c) The temporal side of the superficial sylvian vein (arrowhead) is dissected and the superficial sylvian vein is moved to the frontal side. (d) The superficial sylvian vein at the distal sylvian fissure (arrow) is skeletonized from the frontal and temporal sides by dissection, resulting in a space of sufficient width for the sylvian fissure. The arrowheads show the same positions of the superficial sylvian vein
DISCUSSION
The superficial and deep sylvian veins are key structures for achieving a wide opening of the sylvian fissure. A distal part of the sylvian fissure shows anatomically complicated venous drainage to achieve a wide sylvian opening. Frigeri et al.[2] demonstrated that the frontosylvian, temporosylvian, and parietosylvian veins all join into SSV at the distal sylvian fissure. In addition, the insular veins ascend vertically from the deep sylvian fissure and are three-dimensionally anastomosed to SSV.[6] There are five to six sylvian veins on each frontal and temporal lobe, and a few of them are flowing into SSVs. ICG videoangiography can detect the tributaries entering SSV. Furthermore, the tributaries from the insula are occasionally recognized as presented in Figure 1. However, it is unfortunately difficult for ICG videoangiography to observe all deep venous drainages before dissection. In spite of the limitations in the detection of the surface of the sylvian veins, ICG videoangiography provides the neurosurgeon with information on the surface anatomy of SSV.
The cerebral vein is easily damaged due to its relatively thin walls, thus meticulous manipulation is required to preserve these veins during sylvian dissection and avoid causing brain swelling and venous infarction. The risk of injury to the vein, however, increases in patients with SAH because SSV is barely distinguishable within SAH, and the adhesion among the veins, arachnoid, and pia mater on the bulging brain surface makes dissection difficult. The application of ICG in the visualization of venous circulation has been reported with regard to predicting venous sacrifice[1] or confirming the arterial and venous vessel architecture in cases of arteriovenous malformation.[8] Its use to confirm the anatomy of the SSV to assist in facilitating the wide opening of the sylvian fissure has not yet been well described. There are, in general, three patterns of managing the SSV: Dissection on the frontal or temporal side, or complete skeletonization where SSV is detached from both sides.[3,7] ICG videoangiography assists the neurosurgeon in determining a strategy for dissecting the SSV, which functions as an entrance into the deep brain area, at the beginning of the dissection.
CONCLUSION
The performance of ICG videoangiography before dissection may help reduce the incidence of accidental injury of the veins in the sylvian fissure. The authors hope that this method will be widely utilized at the beginning of sylvian dissection.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos Available on: www.surgicalneurologyint.com
Footnotes
Contributor Information
Hisashi Kubota, Email: kubopo@gmail.com.
Yasuhiro Sanada, Email: ysanada@med.kindai.ac.jp.
Kazuhiro Nagatsuka, Email: kaznagatu@med.kindai.ac.jp.
Hiromasa Yoshioka, Email: yoshioka2327@med.kindai.ac.jp.
Michihiro Iwakura, Email: iwak@med.kindai.ac.jp.
Amami Kato, Email: akato-osk@umin.org.
REFERENCES
- 1.Ferroli P, Acerbi F, Tringali G, Albanese E, Broggi M, Franzini A, et al. Venous sacrifice in neurosurgery: New insights from venous indocyanine green videoangiography. J Neurosurg. 2011;115:18–23. doi: 10.3171/2011.3.JNS10620. [DOI] [PubMed] [Google Scholar]
- 2.Frigeri T, Paglioli E, de Oliveira E, Rhoton AL., Jr Microsurgical anatomy of the central lobe. J Neurosurg. 2015;122:483–98. doi: 10.3171/2014.11.JNS14315. [DOI] [PubMed] [Google Scholar]
- 3.Kazumata K, Kamiyama H, Ishikawa T, Takizawa K, Maeda T, Makino K, et al. Operative anatomy and classification of the sylvian veins for the distal transsylvian approach. Neurol Med Chir (Tokyo) 2003;43:427–33. doi: 10.2176/nmc.43.427. [DOI] [PubMed] [Google Scholar]
- 4.Kuroda K, Kinouchi H, Kanemaru K, Wakai T, Senbokuya N, Horikoshi T. Indocyanine green videoangiography to detect aneurysm and related vascular structures buried in subarachnoid clots. J Neurosurg. 2011;114:1054–6. doi: 10.3171/2010.11.JNS1036. [DOI] [PubMed] [Google Scholar]
- 5.Roessler K, Krawagna M, Dörfler A, Buchfelder M, Ganslandt O. Essentials in intraoperative indocyanine green videoangiography assessment for intracranial aneurysm surgery: Conclusions from 295 consecutively clipped aneurysms and review of the literature. Neurosurg Focus. 2014;36:E7. doi: 10.3171/2013.11.FOCUS13475. [DOI] [PubMed] [Google Scholar]
- 6.Tanriover N, Rhoton AL, Jr, Kawashima M, Ulm AJ, Yasuda A. Microsurgical anatomy of the insula and the sylvian fissure. J Neurosurg. 2004;100:891–922. doi: 10.3171/jns.2004.100.5.0891. [DOI] [PubMed] [Google Scholar]
- 7.Yaºargil MG. Vol. 1. Stuttgart, New York: Georg Thieme-Verlag; 1984. Microneurosurgery; pp. 165–8. [Google Scholar]
- 8.Zaidi HA, Abla AA, Nakaji P, Chowdhry SA, Albuquerque FC, Spetzler RF. Indocyanine green angiography in the surgical management of cerebral arteriovenous malformations: Lessons learned in 130 consecutive cases. Neurosurgery. 2014;10(Suppl 2):246–51. doi: 10.1227/NEU.0000000000000318. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.