

Abstract
Purpose of review:
To summarize the literature on Alice in Wonderland syndrome (AIWS), a disorder characterized by distortions of visual perception, the body schema, and the experience of time.
Recent findings:
On the basis of 169 published case descriptions, the etiology of AIWS is divided into 8 main groups, with neurologic disorders affecting mostly adults and elderly patients and encephalitides affecting mostly patients aged ≤18 years. Symptoms of AIWS are also experienced in the general population, with up to 30% of adolescents reporting nonclinical symptoms.
Summary:
In clinical cases of AIWS, auxiliary investigations (including blood tests, EEG, and brain MRI) are strongly advised. Treatment should be directed at the suspected underlying condition, although reassurance that the symptoms themselves are not harmful seems to suffice in about 50% of the cases. International classifications such as the DSM and ICD should consider placing the syndrome on their research agenda.
First described in 1955, Alice in Wonderland syndrome (AIWS) is a perceptual disorder characterized by distortions of visual perception (metamorphopsias), the body schema, and the experience of time. The name refers to Lewis Carroll's well-known children's book Alice's Adventures in Wonderland,1 in which Alice feels (among other things) her body growing both larger and smaller (figures 1 and 2). After 60 years of relative obscurity, AIWS has begun to receive scientific attention. This renewed interest is in part because of the current possibility to explore the brain's networks responsible for mediating its symptoms with the aid of functional imaging techniques.2–6 AIWS symptoms have both diagnostic and therapeutic consequences that differ substantially from those in schizophrenia spectrum disorders and other hallucinatory syndromes. This article presents an overview of the literature on AIWS published over the past 60 years and summarizes its implications for clinical practice and research.
Figure 1. Alice experiences total-body macrosomatognosia. Illustration by John Tenniel (1865).

Figure 2. (A) Alice experiences partial macrosomatognosia, and (B) Alice experiences total-body microsomatognosia. Illustrations by John Tenniel (1890).

METHODS
A systematic literature search was carried out in PubMed (until June 2015) using the search terms “Alice in Wonderland syndrome,” “syndrome of Alice in Wonderland,” and variants thereof. Included were articles in the English, Dutch, German, French, Spanish, and Italian languages. All cross-references were checked systematically. In this article, symptoms of AIWS experienced by patients diagnosed with a neurologic, psychiatric, or other medical condition are referred to as “clinical,” and symptoms of AIWS experienced by individuals in the general population who have not sought medical attention are referred to as “nonclinical.”
RESULTS
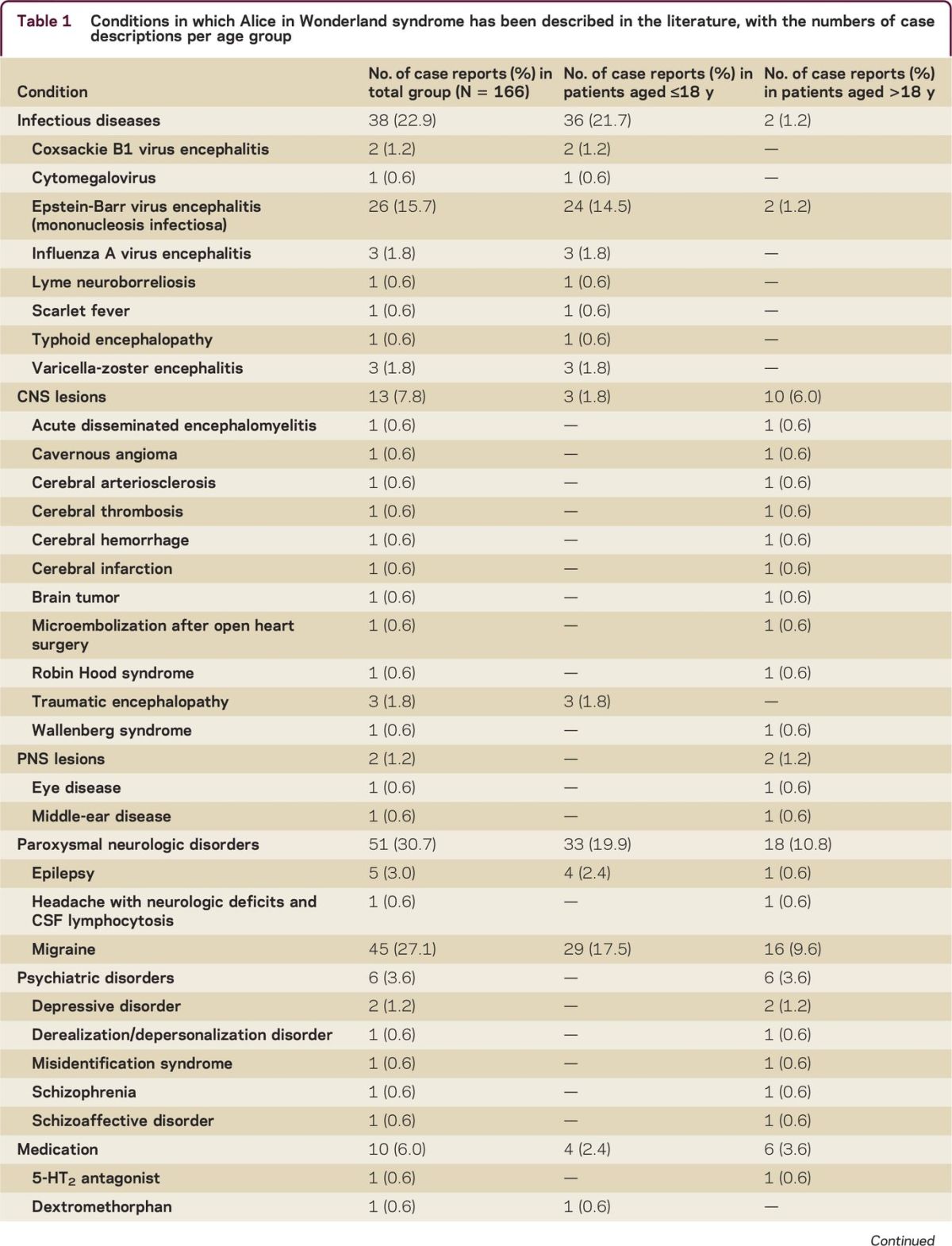
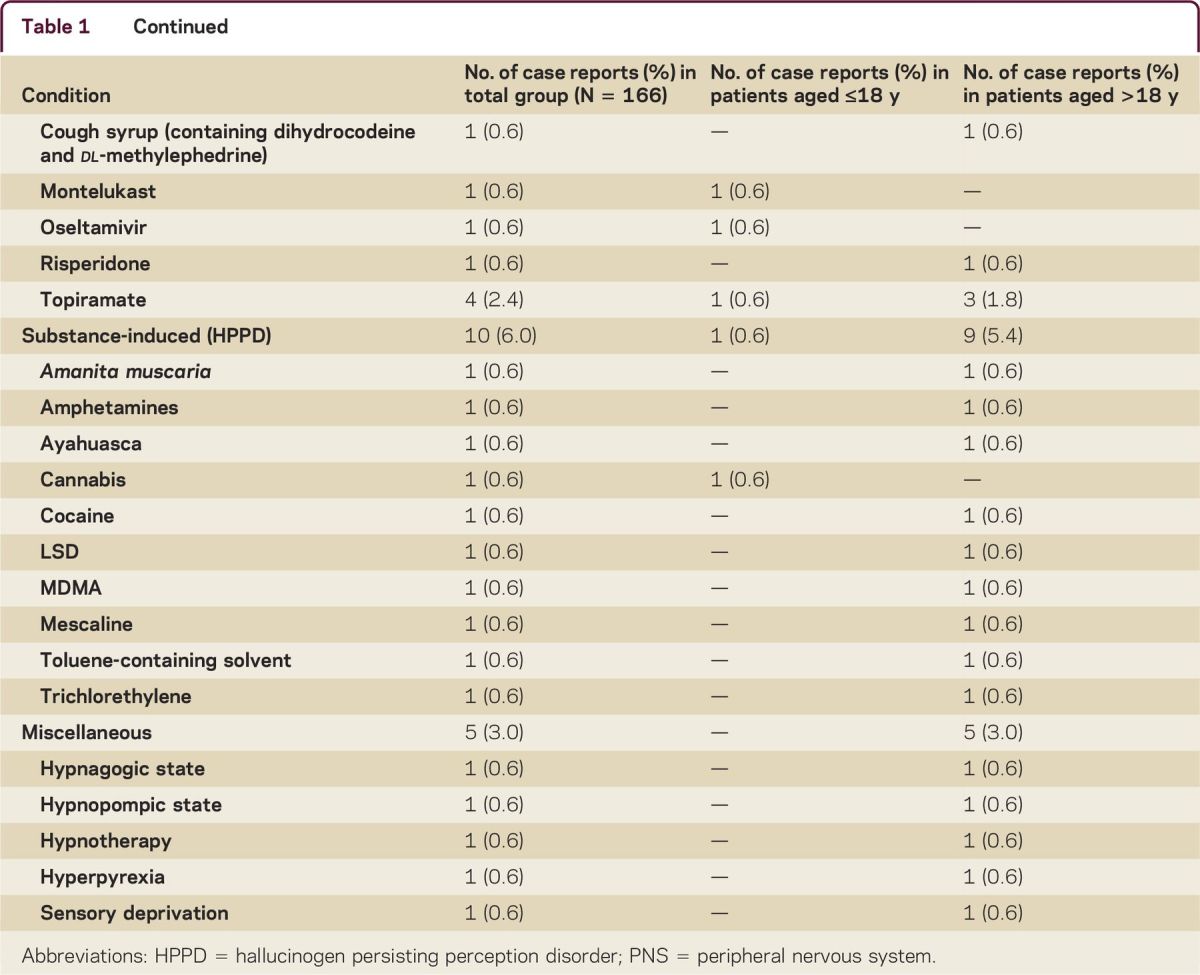
The search terms yielded 130 hits in PubMed. Of these, 59 articles had AIWS as their main subject. Via cross-references an additional 11 articles were found, yielding a total of 70 articles. Of these, more than 50% were published during the prior decade. A total of 170 patients were described, 20 from one case series7 and 48 from another case series.8 The majority of the remaining articles consisted of individual case descriptions. Because one patient was described twice,9,10 the total number of original case descriptions was 169. Patient sex was mentioned for 162 patients; 55.6% of them were male. Age was mentioned in 166 patients; mean age was 15.5 years. A total of 132 patients were ≤18 years, with a mean age of 9 years, and 34 patients were 19 years and older, with a mean age of 40 years. Table 1 presents an overview of the many disorders, intoxications, and other conditions that have been described in the context of AIWS. Among youths, the most frequently described condition was encephalitis (21.7% vs 1.2% among adults and elderly patients), with the Epstein-Barr virus being the most frequently reported pathogen (68.4% of all cases of encephalitis). Among the group of adults and elderly patients, neurologic disorders were most frequently described (16.8%); of all these disorders, migraine was the most prevalent condition (9.6%). The course and outcome were described in 150 patients. In 54 patients (36.0%) the treatment regimen was also specified; this mostly involved pharmacologic treatment aimed at alleviating the underlying condition. One patient received electroconvulsive treatment11 and another patient received repetitive transcranial magnetic stimulation2; both treatments were successful. The remaining patients received no treatment or it was unspecified. Full remission was obtained in 46.7% of all patients, and partial or temporary remission in 11.3%. In chronic conditions such as epilepsy and migraine, full remission was obtained only rarely.
Table 1.
Conditions in which Alice in Wonderland syndrome has been described in the literature, with the numbers of case descriptions per age group
DISCUSSION
Historical perspective
The term Alice in Wonderland syndrome was introduced in 1955 by the British psychiatrist John Todd (1914–1987) to cover a group of symptoms “… intimately associated with migraine and epilepsy, although not confined to these disorders.”12 As envisioned by Todd,12 the group comprised derealization, depersonalization, hyperschematia, hyposchematia, and somatopsychic duality, as well as illusory changes in the size, distance, or position of stationary objects in the visual field; illusory feelings of levitation; and illusory alterations in the sense of the passage of time. Incidentally, Todd was well aware that he was not the first to describe those individual symptoms. Many of them had appeared before in the literature on hysteria,13 on general neurology,14–17 and on soldiers with occipital wounds after World Wars I and II.18,19 Moreover, in 1933 and 1952, Coleman20 and Lippman,21 respectively, had already drawn comparisons between those symptoms and the experiences of Alice in Wonderland, albeit without turning the name into an eponym. Lippman21 was also the first to suggest that the bodily changes experienced by Alice might well be inspired by body schema illusions Lewis Carroll had experienced himself. Carroll (pseudonym of the British mathematician Charles Lutwidge Dodgson, 1832–1898) had migraines, and his diaries indicate that his attacks were sometimes preceded by aural phenomena.22 However, historians consider Lippman's hypothesis inconclusive, as the diaries fail to demonstrate that Dodgson experienced any aural phenomena before he wrote his book.23 An alternative hypothesis is that Dodgson had knowledge of—or perhaps had experimented with—the hallucinogenic mushroom Amanita muscaria.24 Whatever the exact course of events may have been, with Alice in Wonderland, Dodgson created a character that appealed as much to physicians as it did to the book's intended audience. And Todd, by adopting the name, chose a memorable moniker for a group of symptoms hitherto described in isolation of each other.
Phenomenology
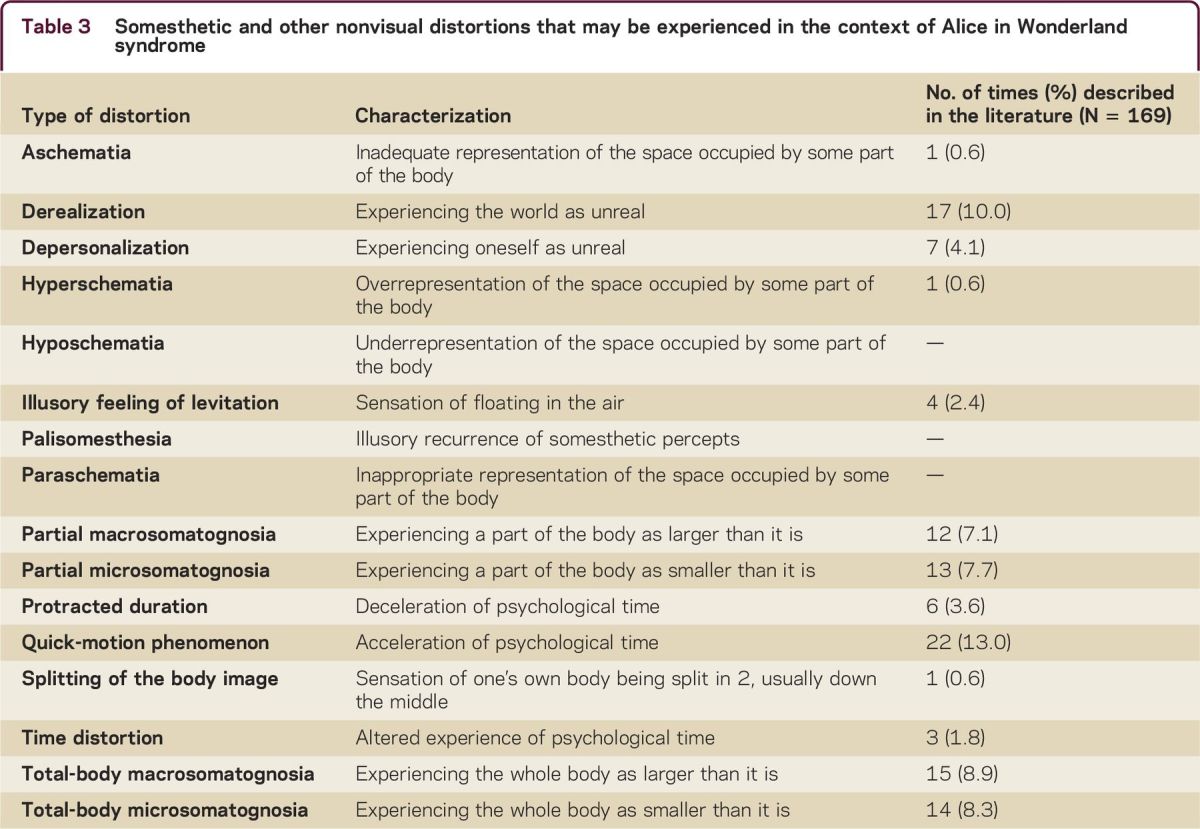
Over the past 60 years, AIWS symptoms have come to include 42 visual symptoms (table 2) and 16 somesthetic and other nonvisual symptoms (table 3). What these symptoms have in common with each other is that they constitute distortions of sensory perception rather than hallucinations or illusions.25 Hallucinations are percepts experienced in the absence of an appropriate stimulus from the outside world, such as a voice heard in the absence of sound production or a cat seen that is not there. Illusions do have a source in the outside world, albeit one that is (often fleetingly) misperceived or misinterpreted. Thus music may be heard in the drone of passing traffic and a curtain moving in the wind may be mistaken for an intruder. Like illusions, distortions are based on sensory impressions, but they feature highly specific changes in highly specific aspects of the sensory input picture. For example, all straight lines may be perceived as wavy (dysmorphopsia), all vertical lines as slanted (plagiopsia), all stationary objects as moving (kinetopsia), or all eyes as unnaturally big (prosopometamorphopsia). Tables 2 and 3 describe the many possible variants and also how often they have been described in case reports of AIWS. Strikingly, micropsia and macropsia have been described most frequently in the literature (in 58.6% and 45.0% of all patients, respectively), which might indicate that they are the most prevalent types of distortion but also that they are the best known and therefore studied most frequently.
Table 2.
Visual distortions (metamorphopsias) that may be experienced in the context of Alice in Wonderland syndrome
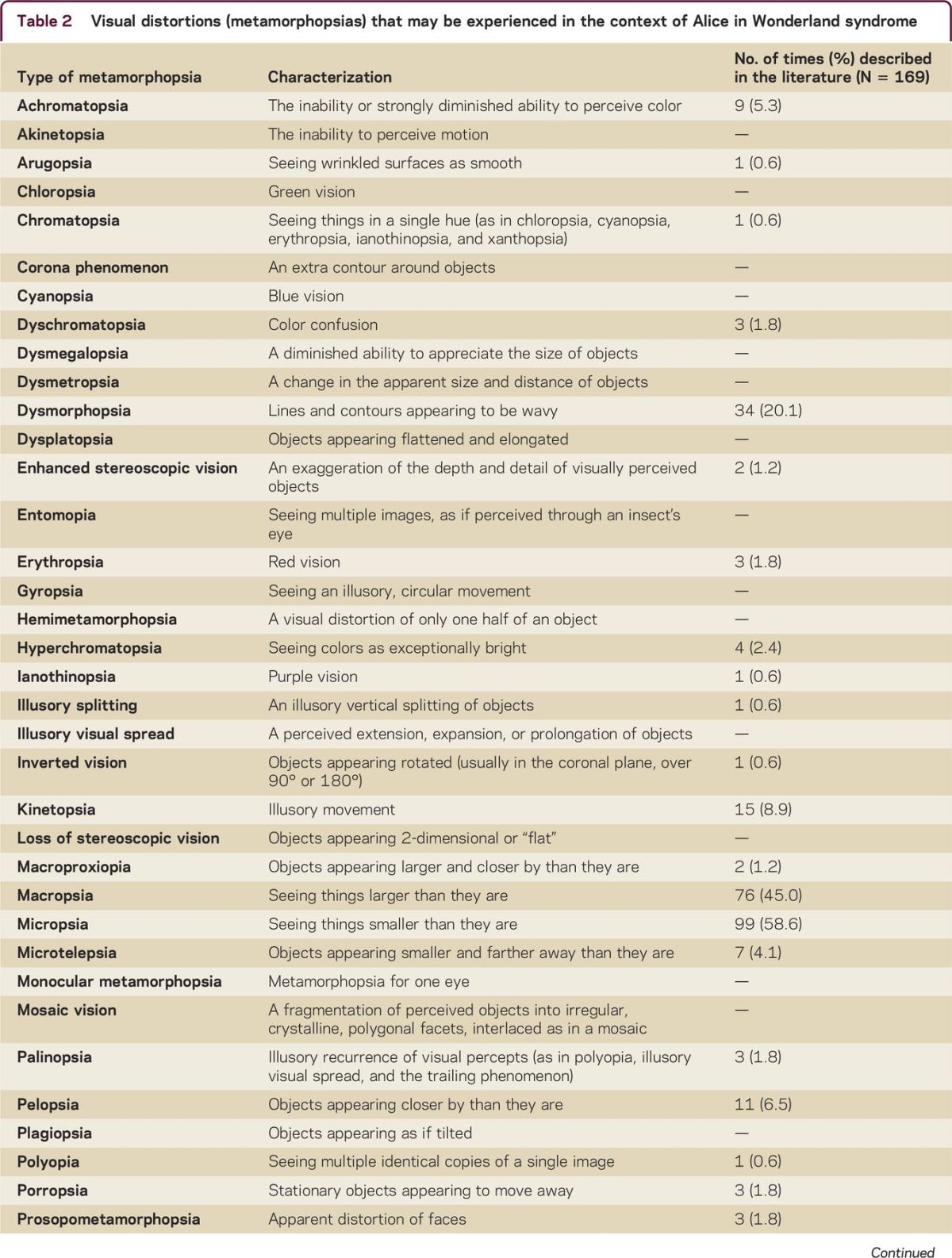
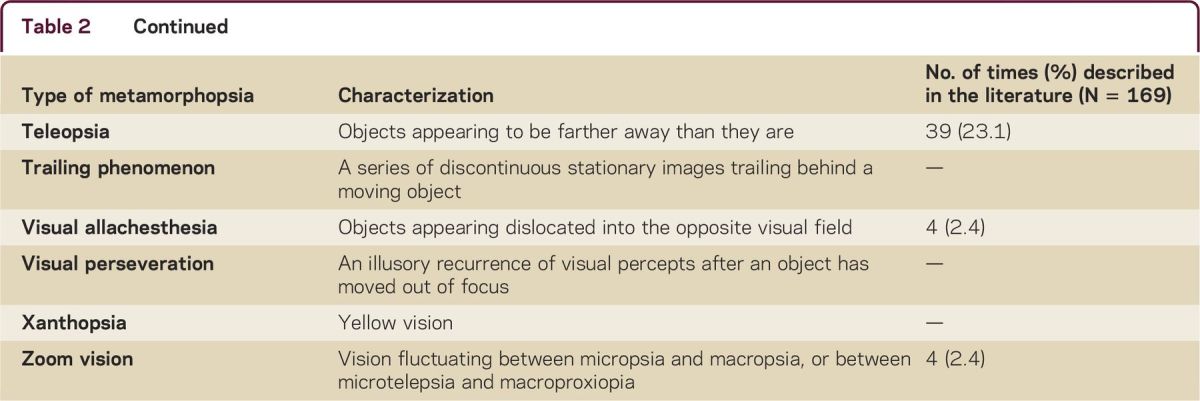
Table 3.
Somesthetic and other nonvisual distortions that may be experienced in the context of Alice in Wonderland syndrome
The duration of symptoms of AIWS tends to be short, mostly on the order of minutes to days26; however, symptoms may also persist for years2 or even be lifelong.27 A salient detail is that after visual fixation on an object, metamorphopsias may sometimes arise after an interval of seconds to minutes.27,28 After that temporal delay, objects are perceived in a distorted manner, but during the delay the perceptual process is undisturbed. In the historical literature this phenomenon has been explained as a sign of cerebral asthenopia28,29 (i.e., an unusual fatigability of the perceptual system).
Epidemiology
No epidemiologic data on AIWS in the population at large are available. Although it is generally assumed that the syndrome is rare, clinical studies among patients with migraine indicate that the prevalence rate in this group may be around 15%.23,30 Moreover, some studies indicate that individual symptoms of AIWS are not rare in the general population. A cross-sectional study of 1,480 adolescents31 found a lifetime prevalence of micropsia and/or macropsia of 5.6% for males and 6.2% for females. A second cross-sectional study of 3,224 high school students32 found 6-month prevalence rates of 3.8% for micropsia, 3.9% for macropsia, 2.5% for protracted duration, and 1.3% for the quick-motion phenomenon. A third cross-sectional study33 of 297 individuals with a median age of 25.7 years found lifetime prevalence rates of 30.3% for teleopsia, 18.5% for dysmorphopsia, 15.1% for macropsia, and 14.1% for micropsia. This study also showed that 38.9% of the affected individuals experienced a single symptom, 33.6% experienced 2, 10.6% experienced 3, and 16.8% experienced 4. This buildup might indicate a common underlying etiologic process responsible for the mediation of all 4 symptoms or a stochastic process in which the presence of one symptom lowers the threshold for another one to join in.
Pathophysiology
The symptoms of AIWS are attributed to functional and structural aberrations of the perceptual system.34 On the whole, central pathology is considered the most prevalent cause; however, dysmorphopsia, for example, is also experienced in the context of retinal ablation and some other types of eye disease, and plagiopsia (visual tilt) is also experienced in the context of labyrinthine disease.35 Nevertheless, most symptoms of AIWS are attributed to centrally located neuron populations and even cell columns that respond selectively to specific types of sensory input (for vision, notably cortical areas V1–V5). Area V4 of the extrastriate visual cortex, for example, responds selectively to color, whereas area V5 responds to movement. Both areas also respond to shape and depth, but bilateral loss of function of V4 results in achromatopsia (the inability to see color) and bilateral loss of V5 results in akinetopsia (the inability to see motion). The inability to visually perceive vertical lines (plagiopsia) or lines under a different angle is attributed to loss of function of orientation columns that are grouped together throughout the horizontal layers of visual cortex. Similarly, various neuron populations have been identified as being responsible for mediating different types of metamorphopsia, and for other metamorphopsias educated guesses have been made.36 Sometimes this involves higher-order mismatches between larger components of the visual network, which can vary interindividually. An example of the latter situation can be found in complex types of prosopometamorphopsia, in which human faces may be perceived consistently as animal faces,27 and even in an apparently straightforward symptom such as micropsia, which was found to be associated with a consistent pattern of occipital hypoactivation and parietal hyperactivation in an fMRI study.6
Mutatis mutandis, the same would seem to hold true for somesthetic distortions, in the sense that functional and/or structural aberrations of specific neuron populations in somatosensory cortical areas are responsible for mediating body schema illusions such as microsomatognosia, palisomesthesia, aschematia, etc. In these cases, parts of the network located around the parieto-temporo-occipital junction are responsible,37 although here too a mismatch between higher-order components of the network as a whole may be at play, as in ischemia of distal parts of the anterior cerebral arteries that supply parts of the perceptual network responsible for integrating composite sensory data for awareness of the body schema.38 Whether similar mechanisms are responsible for mediating time distortions is as yet unknown.
Etiology
The conditions responsible for mediating the symptoms of AIWS are legion. Table 1 presents those described so far in the literature, classified into 8 main groups. One of those groups is “substance-induced,” also known as hallucinogen persisting perception disorder (HPPD),39 a nosologic construct featured in the DSM-540 and other classifications as a separate diagnostic category that covers perceptual symptoms that arise during (or after the cessation of) the use of illicit substances. The list of conditions associated with AIWS is long and is expected to grow even longer when more cases and case series are published.
Diagnosis and differential diagnosis
AIWS does not feature in major classifications such as the ICD-1041 and the DSM-5.40 As a consequence, in clinical practice the diagnosis of AIWS stands and falls with proper history-taking, a thorough physical (including neurologic and often otologic and/or ophthalmic) examination, and sound knowledge of the many and varying symptoms characteristic of AIWS and their possible causes. Cases with a suspected central origin should prompt auxiliary investigations including blood tests, EEG, and brain MRI scan, even though the chances of finding any demonstrable lesions are generally considered to be low.8
The differential diagnosis of AIWS and its individual symptoms is complex, as it involves at least 3 levels of conceptualization. First, the symptoms need to be distinguished from other positive disorders of perception such as hallucinations and illusions, with which they may be easily confused. Second, their most likely cause needs to be established. As table 1 indicates, many diagnoses are possible. Therefore, third, whether the diagnosed condition may be responsible for mediating the symptoms must be established. Because metamorphopsias and other distortions are also experienced by individuals in the general population, situations may arise in which the disorder diagnosed is not causally connected with the symptoms at hand or in which a therapeutic intervention turns out to be the actual cause.
Treatment and prognosis
Most nonclinical and clinical cases of AIWS are considered benign, in the sense that full remission of the symptoms can often be obtained, sometimes spontaneously and in other cases after proper treatment. However, in clinical cases with an underlying chronic condition (such as migraine and epilepsy), symptoms tend to recur in concordance with active phases of the disease, and in cases of encephalitis the prognosis may also vary. As a consequence, the need to treat requires careful assessment, proper knowledge of the natural course of the various underlying conditions that are possible, and a careful explanation to the patient of what to expect from which therapeutics under which circumstances. In many cases reassurance will suffice. Whenever treatment is considered useful and necessary, it needs to be aimed at the suspected underlying condition. In clinical practice this mostly involves the prescription of antiepileptics, migraine prophylaxes, antiviral agents, or antibiotics. The literature indicates that antipsychotics are rarely prescribed7 and that in most cases their effectiveness is considered marginal. Moreover, when distortions are experienced as comorbid symptoms in patients with psychosis, it is important to take into account the possibility that they can sometimes be induced or aggravated by antipsychotics because of their potential to lower the threshold for epileptic activity (as has been described for risperidone).42
Limitations
The number of case descriptions of AIWS is small, especially considering the fact that the syndrome appears to be seriously underdiagnosed and that individual symptoms may be systematically neglected. This may be at least partly because international diagnostic classifications have so far refrained from including the syndrome. The operational definition of AIWS and its diagnostic criteria are in need of further development. More specifically, the question remains whether distortions in the olfactory, gustatory, auditory, sexual, coenesthetic, kinesthetic, proprioceptive, algesic, vestibular, and thermic modalities should be added to the list of possible symptoms of AIWS. More importantly, however, the validity of AIWS as an independent nosologic construct needs to be assessed, as well as its overlap with related syndromes such as HPPD (which is also referred to in the literature as “LSD-induced Alice in Wonderland syndrome”43). Other limitations are the lack of systematic epidemiologic data and our limited insight into the many etiologic and pathophysiologic mechanisms possible in this context. Functional imaging techniques such as SPECT and fMRI have the potential to aid in localizing the network structures involved in mediating the symptoms of AIWS; however, so far, only 5 case reports have been published,2–6 probably because patients with longer-lasting distortions are hard to find and contrast signals in individual patients may be weak.
CONCLUSIONS
Since 1955, no more than 169 case descriptions of AIWS have been published. The literature indicates that this may be only the tip of the iceberg, with many individual symptoms of AIWS being experienced (albeit occasionally and only fleetingly) by up to 30% of adolescents in the general population. Although reassurance seems to suffice in roughly half of the clinical cases, the suspicion of a central origin of the symptoms should prompt auxiliary investigations in the form of blood tests, EEG, and brain MRI. Although firm evidence to justify these auxiliary investigations is lacking, I recommend them on clinical grounds because of the spectrum of known etiologies and the prospect of improved outcome in a substantial number of cases after adequate treatment. Treatment, if necessary, needs to be directed at the suspected underlying cause. Regarding research, much larger patient sample sizes are needed to allow for sufficient statistical power of empirical studies of AIWS and its individual symptoms. In addition, epidemiologic surveys in the population at large are needed to establish sound prevalence data. As an alternative or an adjuvant strategy, one might consider creating an international database for cases of AIWS, with special attention paid to phenomenological characteristics, diagnostic findings (including substance abuse), natural course, and treatment results. For such a database to be effective, all new cases of AIWS should be subjected to a systematic assessment, including proper history-taking, neurologic and other physical examinations, and auxiliary investigations. In chronic cases, functional imaging techniques may be helpful in establishing specific neurobiological correlates of individual symptoms (although there are often various practical obstacles to be overcome). AIWS is in need of proper representation in international diagnostic classifications such as the ICD (for example under the heading of “Diseases of the Nervous System, Episodic and Paroxysmal Disorders” or “Other Disorders of the Nervous System”) and the DSM (preferably under a new heading called “Perceptual Disorders,” which in future editions might also include other nonpsychotic perceptual disorders such as the Charles Bonnet syndrome, exploding head syndrome, and cenesthesiopathy). Last but not least, our insight into the nature of AIWS might be enhanced by network analyses of the mutual relationships of individual symptoms as well as their relationships with the perceptual networks underlying them. In the meantime, however, it is possible to carry out a careful diagnostic procedure to help this partly hidden group of patients obtain a proper diagnosis and, if possible, adequate reassurance and, if necessary, appropriate treatment.
Take-home points
AIWS is characterized by perceptual distortions rather than hallucinations or illusions and therefore needs to be distinguished from schizophrenia spectrum and other psychotic disorders
When symptoms of AIWS are transient and not associated with any other pathology, reassurance that the symptoms themselves are not harmful may suffice
Based on the large spectrum of known etiologies and the prospect of improved outcome, I recommend auxiliary investigations to address symptom reoccurrence causing major distress or dysfunction, with or without other pathology
In clinical cases, treatment needs to be directed at underlying conditions
Footnotes
Supplemental data at Neurology.org/cp
AUTHOR CONTRIBUTIONS
Drafting/revising the manuscript, study concept or design, and analysis or interpretation of data.
STUDY FUNDING
No targeted funding reported.
DISCLOSURES
J.D. Blom received publishing royalties for Katatonie en Dissociatie (AccreDidact/Prelum, 2014), Visuele Hallucinaties en Andere Positieve Visuele Waarnemingsstoornissen (AccreDidact/Prelum, 2013), Hallucinations: Research and Practice (Springer, 2012), and A Dictionary of Hallucinations (Springer, 2010). Full disclosure form information provided by the author is available with the full text of this article at Neurology.org/cp.
REFERENCES
- 1.Carroll L. Alice's Adventures in Wonderland. London: MacMillan and Co.; 1865. [Google Scholar]
- 2.Blom JD, Looijestijn J, Goekoop R, et al. Treatment of Alice in Wonderland syndrome and verbal auditory hallucinations using repetitive transcranial magnetic stimulation. A case report with fMRI findings. Psychopathology 2011;44:337–344. [DOI] [PubMed] [Google Scholar]
- 3.Morland D, Wolff V, Dietemann JL, et al. Robin Hood caught in Wonderland: brain SPECT findings. Clin Nucl Med 2013;38:979–981. [DOI] [PubMed] [Google Scholar]
- 4.Kuo YT, Chiu NC, Shen EY, Ho CS, Wu MC. Cerebral perfusion in children with Alice in Wonderland syndrome. Pediatr Neurol 1998;19:105–108. [DOI] [PubMed] [Google Scholar]
- 5.Gencoglu EA, Alehan F, Erol I, Koyuncu A, Aras M. Brain SPECT findings in a patient with Alice in Wonderland syndrome. Clin Nucl Med 2005;30:758–759. [DOI] [PubMed] [Google Scholar]
- 6.Brumm K, Walenski M, Haist F, Robbins SL, Granet DB, Love T. Functional magnetic resonance imaging of a child with Alice in Wonderland syndrome during an episode of micropsia. J AAPOS 2010;14:317–322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Losada-Del Pozo R, Cantarín-Extremera V, García-Peñas JJ, et al. Caracteristícas y evolución de los pacientes con síndrome de Alicia en el País de las Maravillas. Rev Neurol 2011;53:641–648. [PubMed] [Google Scholar]
- 8.Liu AM, Liu JG, Liu GW, Liu GT. “Alice in Wonderland” syndrome: presenting and follow-up characteristics. Pediatr Neurol 2014;51:317–320. [DOI] [PubMed] [Google Scholar]
- 9.Eshel GM, Eyov A, Lahat E, Brauman A. Alice in Wonderland syndrome, a manifestation of acute Epstein-Barr virus infection. Pediatr Infect Dis J 1987;6:68. [DOI] [PubMed] [Google Scholar]
- 10.Lahat E, Eshel G, Arlazoroff A. “Alice in Wonderland” syndrome: a manifestation of infectious mononucleosis in children. Behav Neurol 1991;4:163–166. [DOI] [PubMed] [Google Scholar]
- 11.Bui E, Chatagner A, Schmitt L. Alice in Wonderland syndrome in major depressive disorder. J Neuropsychiatry Clin Neurosci 2010;22:352. [DOI] [PubMed] [Google Scholar]
- 12.Todd J. The syndrome of Alice in Wonderland. Can Med Assoc J 1955;73:701–704. [PMC free article] [PubMed] [Google Scholar]
- 13.Charcot JM. Leçons du Mardi à La Salpêtrière. Policlinique 1888–1889. Paris: E. Lecrosnier & Babé; 1889. [Google Scholar]
- 14.Veraguth O. Ueber Mikropsie und Makropsie. Dtsch Z Nervenheilkd 1903;24:453–464. [Google Scholar]
- 15.Bonnier P. L'aschématie. Rev Neurol 1905;13:605–609. [Google Scholar]
- 16.Wilson SAK. Dysmetropsia and its pathogenesis. Trans Ophthalmol Soc U K 1916;36:412–444. [Google Scholar]
- 17.Pötzl O. Über Anfälle vom Thalamustypus. Z Gesamte Neurol Psychiatr 1943;176:793–800. [Google Scholar]
- 18.Gelb A, Goldstein K. Zur Psychologie des optischen Wahrnehmungs- und Erkennungsvorganges. Z Gesamte Neurol Psychiatr 1918;41:1–141. [Google Scholar]
- 19.Seitelberger F. Über Phantomerscheinungen bei Thalamuserkrankungen. Wien Z Nervenheilkd Grenzgeb 1952;4:259–265. [Google Scholar]
- 20.Coleman SM. Misidentification and non-recognition. J Ment Sci 1933;79:42–51. [Google Scholar]
- 21.Lippman CW. Certain hallucinations peculiar to migraine. J Nerv Ment Dis 1952;116:346–351. [DOI] [PubMed] [Google Scholar]
- 22.Podoll K, Robinson D. Lewis Carroll's migraine experiences. Lancet 1999;353:1366. [DOI] [PubMed] [Google Scholar]
- 23.Restak RM. Alice in migraineland. Headache 2006;46:306–311. [DOI] [PubMed] [Google Scholar]
- 24.Carmichael C. Wonderland revisited. London Miscellany 1996;28:19–28. [Google Scholar]
- 25.Blom JD. A Dictionary of Hallucinations. New York, NY: Springer; 2010. [Google Scholar]
- 26.Lanska JR, Lanska DJ. Alice in Wonderland syndrome: somesthetic vs visual perceptual disturbance. Neurology 2013;80:1262–1264. [DOI] [PubMed] [Google Scholar]
- 27.Blom JD, Sommer IEC, Koops S, Sacks OW. Prosopometamorphopsia and facial hallucinations. Lancet 2014;384:1998. [DOI] [PubMed] [Google Scholar]
- 28.Willanger R, Klee A. Metamorphopsia and other visual disturbances with latency occurring in patients with diffuse cerebral lesions. Acta Neurol Scand 1966;42:1–18. [Google Scholar]
- 29.Pötzl O. Die Optisch-Agnostische Störungen. Leipzig: F. Deuticke; 1928. [Google Scholar]
- 30.Smith RA, Wright B, Bennett S. Hallucinations and illusions in migraine in children and the Alice in Wonderland syndrome. Arch Dis Child 2015;100:296–298. [DOI] [PubMed] [Google Scholar]
- 31.Abe K, Suzuki T. Prevalence of some symptoms in adolescence and maturity: social phobias, anxiety symptoms, episodic illusions and idea of reference. Psychopathology 1986;19:200–205. [DOI] [PubMed] [Google Scholar]
- 32.Abe K, Oda N, Araki R, Igata M. Macropsia, micropsia, and episodic illusions in Japanese adolescents. J Am Acad Child Adolesc Psychiatry 1989;28:493–496. [DOI] [PubMed] [Google Scholar]
- 33.Lipsanen T, Lauerma H, Peltola P, Kallio S. Visual distortions and dissociation. J Nerv Ment Dis 1999;187:109–112. [DOI] [PubMed] [Google Scholar]
- 34.ffytche DH, Howard RJ. The perceptual consequences of visual loss: “positive” pathologies of vision. Brain 1999;122:1247–1260. [DOI] [PubMed] [Google Scholar]
- 35.Deecke L, Mergner T, Plester D. Tullio phenomenon with torsion of the eyes and subjective tilt of the visual surround. Ann NY Acad Sci 1981;374:650–655. [DOI] [PubMed] [Google Scholar]
- 36.ffytche DH, Blom JD, Catani M. Disorders of visual perception. J Neurol Neurosurg Psychiatry 2010;81:1280–1287. [DOI] [PubMed] [Google Scholar]
- 37.Ceriani F, Gentileschi V, Muggia S, et al. Seeing objects smaller than they are: micropsia following right temporo-parietal infarction. Cortex 1998;34:131–138. [DOI] [PubMed] [Google Scholar]
- 38.Kew J, Wright A, Halligan PW. Somesthetic aura: the experience of “Alice in Wonderland.” Lancet 1998;351:1934. [DOI] [PubMed] [Google Scholar]
- 39.Litjens RP, Brunt TM, Alderliefste GJ, et al. Hallucinogen persisting perception disorder and the serotonergic system: a comprehensive review including new MDMA-related clinical cases. Eur Neuropsychopharmacol 2014;24:1309–1323. [DOI] [PubMed] [Google Scholar]
- 40.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed Washington, DC: American Psychiatric Association; 2013. [Google Scholar]
- 41.World Health Organization. The International Classification of Diseases, 10th Revision. Geneva: World Health Organization; 1992. [Google Scholar]
- 42.Morehead DB. Exacerbation of hallucinogen-persisting perception disorder with risperidone. J Clin Psychopharmacol 1997;17:327–328. [DOI] [PubMed] [Google Scholar]
- 43.Lerner AG, Lev Ran S. LSD-associated “Alice in Wonderland syndrome” (AIWS): a hallucinogen persisting perception disorder (HPPD) case report. Isr J Psychiatry Relat Sci 2015;52:67–69. [PubMed] [Google Scholar]