
Figure 1.
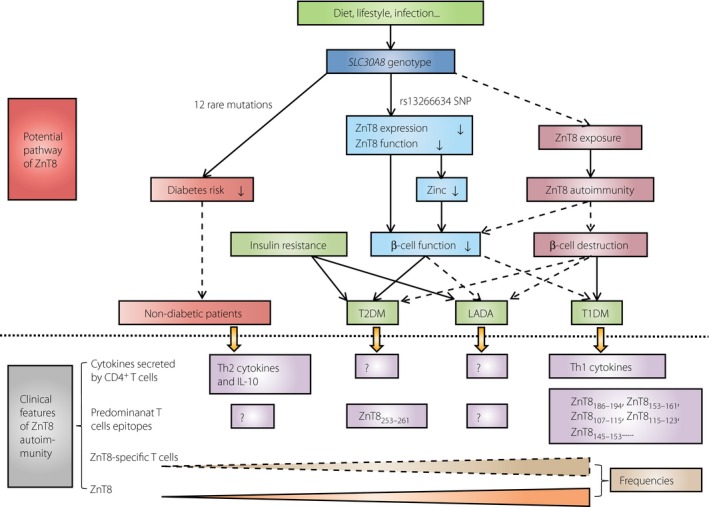
The clinical features (below the dotted line) and potential pathway (above the dotted line) of zinc transporter 8 (ZnT8)in diabetes. The initial phase of diabetes might be the interaction between genetic and environmental factors. One or more of the 12 rare mutations of SLC30A8 might be dominant to environmental factors and reduce the risk of diabetes (protect effect). In contrast, the C allele of rs13266634 single nucleotide polymorphism might downregulate ZnT8 protein expression and transporter activity causing decreased zinc concentration (indirect biological effect), and subsequently impaired β‐cell function (direct biological effect). In addition, during the biosynthesis and secretion of insulin, exocytosis of insulin granules can increase the chance of ZnT8 exposed to the cell surface, which initiates ZnT8 epitope‐specific T cells‐mediated β‐cell destruction, and cause type 1 diabetes mellitus (T1DM; autoimmune injury), or cause type 2 diabetes mellitus (T2DM) and latent autoimmune diabetes in adults (LADA; combined with insulin resistance). The prevalence of ZnT8A and ZnT8‐specific T cells is gradiently decreased from T1DM, through T2DM, then to healthy controls clinically. The cytokine secretion and T cell epitopes of ZnT8‐specific T cells are different in T1DM and T2DM. The solid lines represent certain effect. The dashed line represents the possible effect. The symbol ‘?’ represents the lack of relevant data. IL‐10, interleukin‐10; Th1, type 1 T helper; Th2, type 2 T helper.