

Abstract
Purpose:
To assess the quality of life (QOL) of elderly people in the “Academia da Cidade program” (ACP), a public Brazilian Government Program encourages physical and leisure activity in Recife, Brazil.
Materials and Methods:
This cross-sectional study evaluated 181 elderly people attending the “ACP” at least twice a week. Demographic, socioeconomic, and clinical data were presented according to World Health Organization QOL (WHOQOL)-BREF and WHOQOL-OLD scores.
Results:
Univariate analysis showed that WHOQOL-BREF and WHOQOL-OLD scores were positively associated with longer duration of participation in “ACP,” P < 0.030 and P < 0.003, respectively, a multivariate regression analysis showed that duration of participation in “ACP” remained associated with higher WHOQOL-BREF (P = 0.023) and WHOQOL-OLD (P = 0.038) scores.
Conclusion:
A longer duration of participation in a community-based physical activity program, “ACP,” may contribute to a better QOL for the elderly in Brazil.
Keywords: Academia da Cidade program, elderly, physical activity, quality of life
Introduction
The quality of life (QOL) assessment in elderly people has been a priority in many developed countries to guide public policy, including social, health, and environmental actions.[1,2] The World Health Organization (WHO) developed an international cross-culturally comparable QOL assessment instrument, WHOQOL. To adapt WHOQOL to use with elderly people, a specific version was created and validated namely WHOQOL-OLD.[3,4]
Physical activity has been associated with better QOL and fewer chronic diseases.[5] Despite the benefits of physical activity, physical inactivity prevalence is high, especially among the elderly. Physical inactivity has been associated with chronic disease.[6] For this reason, public policy encourages physical activity as necessary. Some physical activity programs for inactive people have been developed in Europe and America.[7,8] However, physical activity programs are needed, especially in countries such as Brazil, which is experiencing a rapid demographic transition and a burden of chronic diseases.[9] In 2002, the Brazilian government created a public program, the “Academia da Cidade Program (ACP)” to encourage community individuals to have physical and leisure activity at public parks (www2.recife.pe.gov.br/projetos-e-acoes/projetos/academia-da-cidade., Accessed 22 January 2012).
At present, ACPs are located in Recife in open public spaces in different neighborhoods with approximately 32,000 participants, 15% of whom are elderly. Some studies have evaluated ACP positively.[10,11] Our aim is to assess the QOL according to WHOQOL-BREF and WHOQOL-OLD instruments on elderly participants of ACP in Recife.
Materials and Methods
This cross-sectional study evaluated elderly people attending the ACP between March and December 2013. This study was previously approved by the Research Ethics Committee of IMIP and participants signed an informed consent.
ACP activities are led by physical education teachers and offer free supervised leisure-time physical activity sessions, including stretching, aerobic, and resistance training exercises, walking, dancing classes, and other activities. ACP activities are offered every hour from 5 am to 10 am and 5 pm to 10 pm during weekdays. Each class has around 20 participants.
Participants aged 60 years or more, who have been participating in the program at least twice a week, were selected. Elderly with dementia and other mental health disorders were excluded.
The WHOQOL-OLD and WHOQOL-BREF questionnaires were applied, and for illiterate participants, the questionnaire was filled out by the researchers.
WHOQOL-BREF explores six domains: “environment” (8 items), “physical” (7 items), “psychological” (6 items), “social relationships” (3 items), and “overall QOL” (2 items). Values of domains were transformed into a range between 0 and 100. WHOQOL-OLD accesses elderly-specific facets of QOL covering: Sensory abilities, autonomy, past, present, and future activities, social participation, death and dying, and intimacy. Both Portuguese version of these questionnaires were validated and showed adequate internal consistency; Cronbach's coefficients were ranged from 0.71 to 0.88. These questionnaires were administered by two trained interviewers without knowing the goal of the study. A third questionnaire was used to obtain information about the duration of participation in the ACP, demographic, socioeconomic, and clinical data of the participants.
WHOQOL-OLD and WHOQOL-BREF scores were presented in mean (±standard deviation). Proportions were compared by Chi-square test and the distribution of metric variables among tertiles of WHOQOL scores by Kruskal–Wallis test. Univariate and multivariate analysis, using linear regress models, were performed to identify variables associated with WHOQOL-BREF and WHOQOL-OLD.
Results
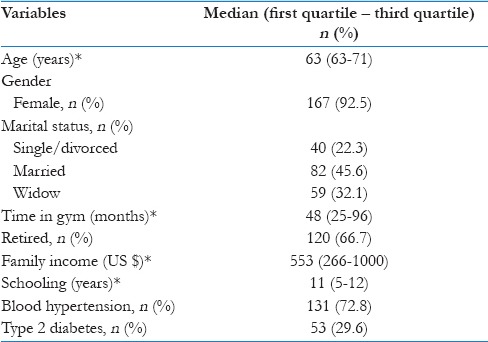
The main characteristics of the 181 individuals are shown in Table 1. Most of them were retired women, had few years of schooling, and had low family income. Blood hypertension and type 2 diabetes were very common.
Table 1.
Main characteristics of the 181 participants
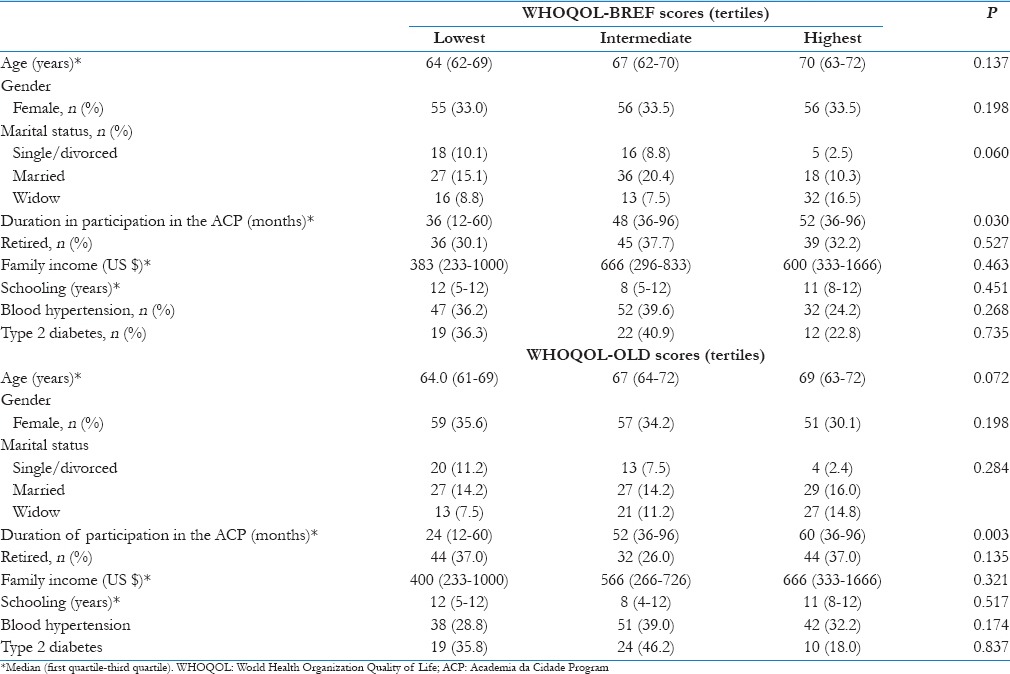
Demographic, socioeconomic, and clinical data according to the WHOQOL-BREF and WHOQOL-OLD scores in tertiles (lowest, intermediate, and highest) are shown in Table 2. According to the WHOQOL-BREF and WHOQOL-OLD scores, only the duration of participation in the APC showed a significant difference of P = 0.030 and P = 0.003, respectively.
Table 2.
Demographic, socioeconomic, and clinical data of participants according to the WHOQOL-BREF and WHOQOL-OLD scores in tertiles (lowest, intermediate, and highest)
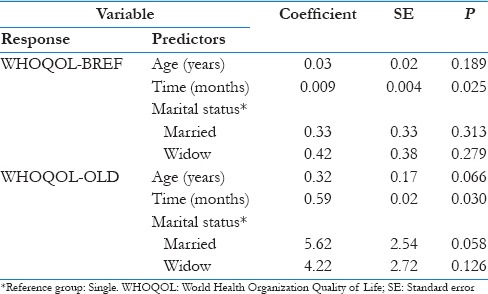
Multivariate analysis linear regression models were adjusted. Predictor variables for WHOQOL-BREF were age, gender, duration of participation in the APC, and marital status and for WHOQOL-OLD they were gender, age, duration of participation in the APC, retired and blood hypertension; all showed P < 0.20 in univariate analysis [Table 2]. After mutual adjustment, only the duration of participation in the APC remained significantly associated with WHOQOL-BREF and WHOQOL-OLD scores (P = 0.023 and P = 0.038), respectively [Table 3].
Table 3.
Adjusted effects of the variables age, time, and marital status on the variables WHOQOL-BREF and WHOQOL-OLD through the adjustment of the linear regression
Discussion
A longer duration of participation in this community-based physical activity program, ACP, was associated with a positive trend in QOL of the participants according to both WHOQOL-BREF and WHOQOL-OLD scores. ACP is a Brazilian government program focusing on physical activity and aims to provide the community of Recife city with the opportunity to engage in regular physical activity by offering free physical exercise classes. This program is offered in public places (parks and squares), the classes are conducted by physical education teachers, and healthy lifestyles are recommended. This ACP results are in agreement with other studies that have shown a positive impact of community-based physical activity program in health.[10,11]
QOL has been positively associated with physical activity.[5] Recently, Sampaio and Ito described in Japan that the highest influence on WHOQOL-BREF was physical activity.[12] The scores of QOL in elderly people have been linked to other factors, such as age, family income, schooling, and positive perceptions about health and depression.[5] In our study, age, income, and schooling did not affect the QOL scores. However, we studied a specific elderly age and all the participants had low income and schooling. This reason could justify the finding of no differences among these variables in our study.
A significant increase in life expectancy and a decrease in the fertility rate in recent decades in Brazil have led to a significant aging population. Aging is associated with the loss of independence and autonomy, which may contribute to a decreased QOL. However, the elderly people studied seem to be already committed and motivated to this specific physical activity program, ACP. This may explain our finding of similar WHOQOL-OLD and WHOQOL-BREF scores among the elderly at different ages.
The duration of participation in ACP may have influenced the variations in response about QOL regarding age on the questionnaire, and we observed a significant increase in the values of the WHOQOL-OLD and WHOQOL-BREF scores according to the time participated in ACP. However, our study had a cross-sectional design, and exposition (ACP) and outcome (QOL) were assessed simultaneously. A cohort study could contribute to a better understanding of this association.
Our participants were almost females. Women in our region have about a 10 years longer lifespan as compared to men. The high number of widows may corroborate this finding. Another explanation is that women, especially in our culture, adhere more to preventive health programs than men. Our WHOQOL-OLD and WHOQOL-BREF scores are similar to elderly women from rural area in Brazil, which are greater as compared to residents in the urban area[11] Our scores are also similar to those found in elderly Brazilian women with good physical and psychosocial health.[13] These comparisons seem to indicate that ACP can compete to a better QOL for those women participants.
The WHOQOL-OLD and WHOQOL-BREF questionnaires are complementary. Possibly because the WHOQOL-BREF emphasizes areas questioning physical aspects and social relations, as well as psychological and environmental aspects that the WHOQOL-BREF questionnaire showed a significant relationship between the higher score and participating time in the ACP program. Our WHOQOL-BREF scores were comparable with normative data from a randomly selected sample of a general Brazilian population.[13] The WHOQOL-OLD questionnaire also surveys the aspect of social participation, but rather in the areas of sensory functioning, autonomy, death and dying, intimacy and past, present, and future activities. A subgroup of elders with a greater degree of dependence and fragility might reveal more consistent differences on the WHOQOL-OLD questionnaire if they were participating in the ACP program. It is a fact, however, that most elderly participants in ACP are independent and autonomous.
Our study design did not allow us to conclude that a longer participation in the program was responsible for an increase in QOL scores despite the association with aging. A cohort design could be better explained in this relation.
Our study has some limitations. The sample may be insufficient for a more faithful indication of QOL and it was drawn from participants who joined the ACP; therefore, it may not be representative. Groups with a similar number of individuals in each period of time in the program (e.g., 1, 2 and 5 years) could specify the relationship between duration of participation in ACP and QOL scores. Finally, we could not exclude response bias from some participants.
Conclusion
ACP seems to be an important strategy for favoring the QOL of the elderly population in Recife.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Tucker KL, Buranapin S. Nutrition and aging in developing countries. J Nutr. 2001;131:2417S–23S. doi: 10.1093/jn/131.9.2417S. [DOI] [PubMed] [Google Scholar]
- 2.De Luca d’Alessandro E, Bonacci S, Giraldi G. Aging populations: The health and quality of life of the elderly. Clin Ter. 2011;162:e13–8. [PubMed] [Google Scholar]
- 3.WHOQOL-OLD/World Health Organization (WHO). Brazilian Version. 2006. [Last cited on 2012 Jan 22]. Available from: http://www.ufrgs.br/psiq/WHOQOL-OLD%20Manual%20POrtugues.pdf .
- 4.Fleck MP, Chachamovich E, Trentini C. Development and validation of the Portuguese version of the WHOQOL-OLD module. Rev Saude Publica. 2006;40:785–91. doi: 10.1590/s0034-89102006000600007. [DOI] [PubMed] [Google Scholar]
- 5.Vagetti GC, Barbosa Filho VC, Moreira NB, Oliveira VD, Mazzardo O, Campos WD. Association between physical activity and quality of life in the elderly: A systematic review, 2000-2012. Rev Bras Psiquiatr. 2014;36:76–88. doi: 10.1590/1516-4446-2012-0895. [DOI] [PubMed] [Google Scholar]
- 6.Coombes JS, Law J, Lancashire B, Fassett RG. “Exercise is Medicine”: Curbing the burden of chronic disease and physical inactivity. Asia Pac J Public Health. 2015;27:600–5. doi: 10.1177/1010539513481492. [DOI] [PubMed] [Google Scholar]
- 7.Martín-Valero R, Cuesta-Vargas AI, Labajos-Manzanares MT. Effectiveness of the physical activity promotion programme on the quality of life and the cardiopulmonary function for inactive people: Randomized controlled trial. BMC Public Health. 2013;13:127. doi: 10.1186/1471-2458-13-127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Murphy SM, Edwards RT, Williams N, Raisanen L, Moore G, Linck P, et al. An evaluation of the effectiveness and cost effectiveness of the National Exercise Referral Scheme in Wales, UK: A randomised controlled trial of a public health policy initiative. J Epidemiol Community Health. 2012;66:745–53. doi: 10.1136/jech-2011-200689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Schmidt MI, Duncan BB, Azevedo e Silva G, Menezes AM, Monteiro CA, Barreto SM, et al. Chronic non-communicable diseases in Brazil: Burden and current challenges. Lancet. 2011;377:1949–61. doi: 10.1016/S0140-6736(11)60135-9. [DOI] [PubMed] [Google Scholar]
- 10.Simoes EJ, Hallal P, Pratt M, Ramos L, Munk M, Damascena W, et al. Effects of a community-based, professionally supervised intervention on physical activity levels among residents of Recife, Brazil. Am J Public Health. 2009;99:68–75. doi: 10.2105/AJPH.2008.141978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hallal PC, Carvalho YM, Tassitano RM, Tenório MC, Warschauer M, Reis RS, et al. Qualitative and quantitative evaluation of the “Programa Academia da Cidade”, Recife (PE): The concept of teachers. Rev Bras Atividade Fí Saúde. 2009;14:9–14. [Google Scholar]
- 12.Sampaio PY, Ito E. Activities with higher influence on quality of life in older adults in Japan. Occup Ther Int. 2013;20:1–10. doi: 10.1002/oti.1333. [DOI] [PubMed] [Google Scholar]
- 13.Cruz LN, Polanczyk CA, Camey SA, Hoffmann JF, Fleck MP. Quality of life in Brazil: Normative values for the WHOQOL-bref in a southern general population sample. Qual Life Res. 2011;20:1123–9. doi: 10.1007/s11136-011-9845-3. [DOI] [PubMed] [Google Scholar]