
Table 1.
Suggested algorithm for a need for CT head in children with TBI, (A) younger than 2 years, and (B) for those aged 2 years and older, with GCS scores of 14–15 [4]*
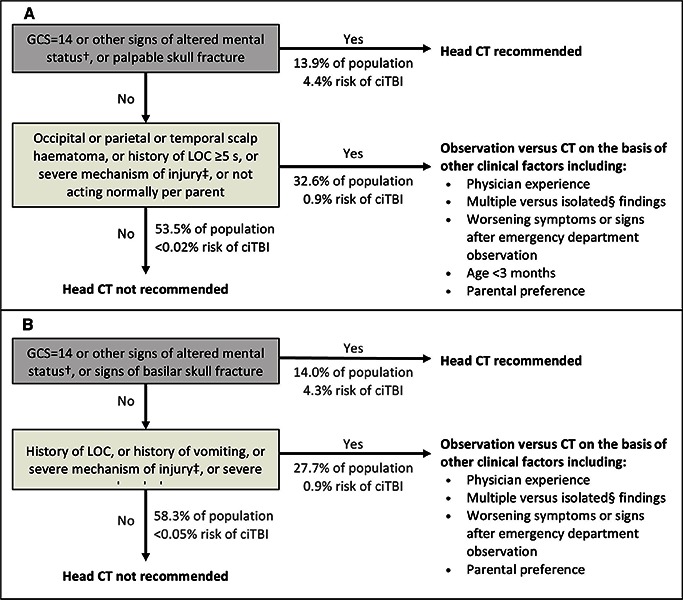 |
ciTBI - clinically-important traumatic brain injury, GCS - Glasgow Coma Scale, LOC - loss of consciousness.
†Other signs of altered mental status: agitation, somnolence, repetitive questioning, or slow response to verbal communication.
‡Severe mechanism of injury: motor vehicle crash with patient ejection, death of another passenger, or rollover; pedestrian or bicyclist without helmet struck by a motorized vehicle; falls of more than 0·9 m (3 feet) (or more than 1·5 m [5 feet] for panel B); or head struck by a high-impact object.
§Patients with certain isolated findings (i.e, with no other findings suggestive of traumatic brain injury), such as isolated LOC, isolated headache, isolated vomiting, and certain types of isolated scalp hematomas in infants older than 3 months, have a risk of ciTBI substantially lower than 1%. Risk of ciTBI exceedingly low, generally lower than risk of CT-induced malignancies. Therefore, CT scans are not indicated for most patients in this group” [4–9].
*Table 1 - Adopted from Kuppermann et al [4].