

Abstract
Background
Chinese herbal medicine (CHM) usage is expected to increase as women suffering from menopausal symptoms are seeking alternative therapy due to concerns from the adverse effects (AEs) associated with hormone therapy (HT). Scientific evidence for their effectiveness and safety is needed.
Objectives
To evaluate the effectiveness and safety of CHM in the treatment of menopausal symptoms.
Search methods
We searched the Gynaecology and Fertility Group's Specialised Register of controlled trials, Cochrane Central Register of Controlled Trials (CENTRAL; 2015, Issue 3), MEDLINE, Embase, CINAHL, AMED, and PsycINFO (from inception to March 2015). Others included Current Control Trials, Citation Indexes, conference abstracts in the ISI Web of Knowledge, LILACS database, PubMed, OpenSIGLE database, and China National Knowledge Infrastructure database (CNKI, 1999 to 2015). Other resources included reference lists of articles as well as direct contact with authors.
Selection criteria
Randomised controlled trials (RCTs) comparing the effectiveness of CHM with placebo, HT, pharmaceutical drugs, acupuncture, or another CHM formula in women over 18 years of age, and suffering from menopausal symptoms.
Data collection and analysis
Two review authors independently assessed 864 studies for eligibility. Data extractions were performed by them with disagreements resolved through group discussion and clarification of data or direct contact with the study authors. Data analyses were performed in accordance with Cochrane Collaboration guidelines.
Main results
We included 22 RCTs (2902 women). Participants were from different ethnic backgrounds with the majority of Chinese origin.
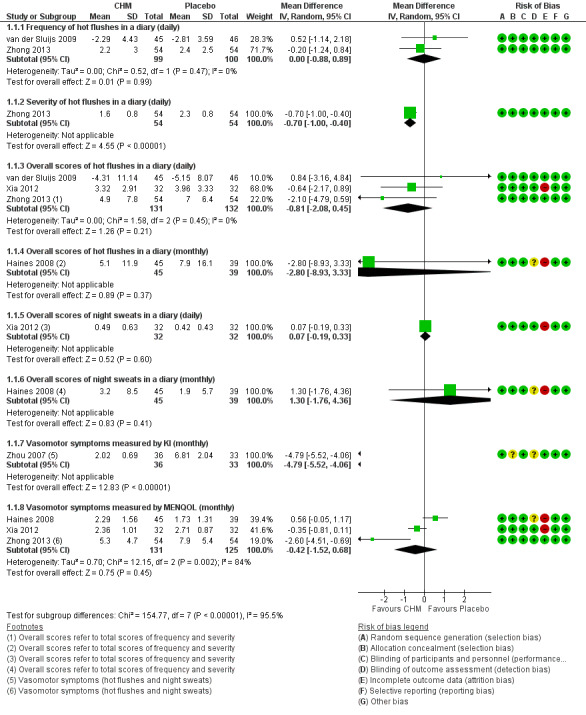
When CHM was compared with placebo (eight RCTs), there was little or no evidence of a difference between the groups for the following pooled outcomes: hot flushes per day (MD 0.00, 95% CI ‐0.88 to 0.89; 2 trials, 199 women; moderate quality evidence); hot flushes per day assessed by an overall hot flush score in which a difference of one point equates to one mild hot flush per day (MD ‐0.81 points, 95% CI ‐2.08 to 0.45; 3 RCTs, 263 women; low quality evidence); and overall vasomotor symptoms per month measured by the Menopause‐Specific Quality of Life questionnaire (MENQOL, scale 0 to 6) (MD ‐0.42 points; 95% CI ‐1.52 to 0.68; 3 RCTs, 256 women; low quality evidence).
In addition, results from individual studies suggested there was no evidence of a difference between the groups for daily hot flushes assessed by severity (MD ‐0.70 points, 95% CI ‐1.00, ‐0.40; 1 RCT, 108 women; moderate quality evidence); or overall monthly hot flushes scores (MD ‐2.80 points, 95% CI ‐8.93 to 3.33; 1 RCT, 84 women; very low quality evidence); or overall daily night sweats scores (MD 0.07 points, 95% CI ‐0.19 to 0.33, 1 RCT, 64 women; low quality evidence); or overall monthly night sweats scores (MD 1.30 points, 95% CI ‐1.76 to 4.36, 1 RCT, 84 women; very low quality evidence). However one study using the Kupperman Index reported that overall monthly vasomotor symptom scores were lower in the CHM group (MD ‐4.79 points, 95% CI ‐5.52 to ‐4.06; 1 RCT, 69 women; low quality evidence).
When CHM was compared with hormone therapy (HT) (10 RCTs), only two RCTs reported monthly vasomotor symptoms using MENQOL. It was uncertain whether CHM reduces vasomotor symptoms (MD 0.47 points, 95% CI ‐0.50 to 1.44; 2 RCTs, 127 women; very low quality evidence).
Adverse effects were not fully reported in the included studies. Adverse events reported by women taking CHM included mild diarrhoea, breast tenderness, gastric discomfort and an unpleasant taste. Effects were inconclusive because of imprecise estimates of effects: CHM versus placebo (RR 1.51; 95% CI 0.69 to 3.33; 7 trials, 705 women; I² = 40%); CHM versus HT (RR 0.96; 95% CI 0.66 to 1.39; 2 RCTs, 864 women; I² = 0%); and CHM versus specific conventional medications (such as Fluoxetine and Estazolam) (RR 0.20; 95% CI 0.03 to 1.17; 2 RCTs, 139 women; I² = 61%).
Authors' conclusions
We found insufficient evidence that Chinese herbal medicines were any more or less effective than placebo or HT for the relief of vasomotor symptoms. Effects on safety were inconclusive. The quality of the evidence ranged from very low to moderate; there is a need for well‐designed randomised controlled studies.
Keywords: Female; Humans; Middle Aged; Drugs, Chinese Herbal; Drugs, Chinese Herbal/adverse effects; Drugs, Chinese Herbal/therapeutic use; Estazolam; Estazolam/therapeutic use; Fluoxetine; Fluoxetine/therapeutic use; Hormone Replacement Therapy; Hot Flashes; Hot Flashes/drug therapy; Menopause; Quality of Life; Randomized Controlled Trials as Topic; Sweating; Sweating/drug effects; Time Factors
Plain language summary
Title: Chinese herbal medicines for menopausal symptoms
Review Question: Are Chinese herbal medicines effective and safe for relieving menopausal symptoms?
Background: Menopause usually takes place when a woman is around 51 years of age. Women can experience symptoms such as hot flushes, sweats, poor sleep, joint pains, anxiousness, dry skin and vagina when the organs which produce female hormones slow down. Usually hormone therapy (HT) is prescribed to reduce the symptoms.
Due to concerns on long term use of HT resulting in adverse effects, women have been looking for alternative treatments to relieve their symptoms. Chinese herbal medicines (CHM) is one of the popular choices. Although CHM has been used for a very long time clinically, its effectiveness and long‐term safety remained unanswered from a scientific perspective.
Study characteristics: This review examined 22 randomised clinical trials where 2902 women took part in the studies; 1499 in the CHM group and 1403 in the control group which might include a placebo (non‐active compound made to look, taste and smell the same as the study compound) or a drug or HT or another CHM formula (different from the one being tested). Most of the studies had a trial period for 12 weeks. The data are current to March 2015.
Key results: We found insufficient evidence that CHM were any more or less effective than placebo or HT for the relief of vasomotor symptoms. Adverse effects were not well reported, some women taking CHM reported mild diarrhoea, breast tenderness, gastric discomfort and an unpleasant taste. Effects on safety were inconclusive.
Quality of the evidence: The quality of the evidence ranged from very low to moderate. The studies did not produce good quality evidence to allow the authors to draw a conclusive statement regarding the effectiveness or safety of CHM.
Summary of findings
Summary of findings for the main comparison. Chinese herbal medicine (CHM) compared with placebo for menopausal symptoms.
| Findings of Effectiveness (Primary outcome) | ||||||
| Population: women with menopausal symptoms Settings: Community Intervention: CHM Comparison: Placebo | ||||||
| Outcomes |
Assumed risk Placebo |
Illustrative comparative risks* (95% CI) CHM compared to placebo |
Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments |
| Vasomotor Symptoms Frequency of hot flushes measured in a diary (daily) | The mean frequency of hot flushes in the control groups ranged across control groups from ‐2.81 to 2.4 points in a diary |
The mean frequency of hot flushes was 0 points flushes per day more in the CHM groups than in placebo group (0.88 to 0.89 points more flushes) in a diary. | _ | 199 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 1 |
A lower score means less bothersome hot flushes |
| Vasomotor Symptoms Severity of hot flushes measured in a diary (daily) | The mean severity of hot flushes in the control groups was 2.3 points in a diary. | The mean severity of hot flushes was 0.70 points lower in the CHM group than in the placebo group (1.00 lower to 0.40 lower) in a diary. | _ | 108 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 |
A lower score means less bothersome hot flushes |
| Vasomotor Symptoms Overall scores of hot flushes in a diary (daily) | The mean overall hot flush scores (frequency and severity) in the control groups ranged across control groups from ‐5.15 to 7.0 scores in a diary |
The mean overall hot flush scores (frequency and severity) in the CHM groups was 0.81 scores lower (2.08 lower to 0.45 higher) in a diary. | _ | 263 (3 RCTs) | ⊕⊕⊝⊝ LOW1 3 | A lower score means less bothersome hot flushes |
| Vasomotor Symptoms Overall scores of hot flushes in a diary (monthly) | The mean overall vasomotor symptoms (hot flushes/night sweats) in the control groups was 7.9 points |
The mean overall vasomotor symptoms (hot flushes/night sweats) was 2.8 points lower in the CHM group than in placebo group (8.93 fewer to 3.33 more) | _ | 84 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 4,5 |
A lower score means less bothersome hot flushes |
| Vasomotor Symptoms Overall night sweats in a diary (daily) | The mean overall daily night sweat score (frequency and severity) in the control groups was 0.42 in a diary |
The mean overall daily night sweat score (frequency and severity) in the CHM group was 0.07 higher (0.19 lower to 0.33 higher) than in placebo in a diary | _ | 64 (1 RCT) | ⊕⊕⊝⊝ LOW 1,6 |
A lower score means less bothersome night sweats |
| Vasomotor Symptoms Overall scores of night sweats in a diary (monthly) | The mean overall monthly night sweats (frequency and severity) in the control groups was 1.9 points |
The mean overall monthly night sweats (frequency and severity) was 1.3 points higher in the CHM group (1.76 fewer to 4.36 more) than in placebo | _ | 84 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 4,5 |
A lower score means less bothersome night sweats |
| Vasomotor Symptoms measured by the Kupperman Index (KI, monthly) | The mean vasomotor symptom scores in the control groups was 6.81 scores on an 11‐item questionnaire |
The mean vasomotor symptom scores was 4.79 points lower in the CHM group (5.52 lower to 4.06 lower) than in placebo, on an 11‐item questionnaire. | _ | 69 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 7 |
KI is a 11‐item questionnaire with scale from 0 to 3. A lower score means fewer symptoms. |
| Vasomotor Symptoms measured by Menopause Specific Quality of Life Questionnaire (MENQOL, monthly) | The mean vasomotor symptom scores in the control groups ranged across control groups from 1.73 to 7.9 points on an 29‐item questionnaire |
The mean vasomotor symptom scores was 0.42 points lower in the CHM group (1.52 lower to 0.68 higher) than in placebo, on an 29‐item questionnaire. | _ | 256 (3 RCTs) | ⊕⊕⊝⊝ LOW1,8 | MENQOL is a 29‐item questionnaire with scale from 0 to 6. A lower score means fewer symptoms. |
| Adverse Effects | 31 per 1000 | 47 per 1000 (22 to 104) | RR 1.51 (0.69 to 3.33) | 705 (7 studies) | ⊕⊝⊝⊝ VERY LOW 8 9 10 |
|
| *The basis for the assumed risk is the median control group risk across studies. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1Downgraded one level due to serious imprecision (small sample size; confidence interval suggests both benefit and harm).
2Downgraded one level due to serious imprecision (small sample size).
3Downgraded one level due to serious risk of bias (high drop‐off and ITT was not or was not properly implemented in one of the three studies, Xia 2012).
4Downgraded one level due to serious risk of bias (blinding of outcome assessors unclear and high likelihood of attrition bias).
5Downgraded two levels due to very serious imprecision (small sample size; very wide confidence interval, suggesting appreciable benefit and harm).
6Downgraded one level due to serious risk of bias (high likelihood of attrition bias).
7Downgraded one level due to serious risk of bias (allocation concealment and blinding of outcome assessors unclear).
8Downgraded one level because of serious inconsistency (the directions of effects were inconsistent).
9Downgraded one level due to serious risk of bias (allocation concealment and blinding of outcome assessors unclear, high likelihood of attrition bias).
10Downgraded one level due to very serious imprecision (very wide confidence interval).
Summary of findings 2. CHM compared with HT for menopausal symptoms.
| Findings of Effectiveness (Primary Outcome) | ||||||
| Patient or population: Women with menopausal symptoms Settings: Outpatients Intervention: CHM Comparison: HT | ||||||
| Outcomesa | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
|
Assumed risk scores/values |
Corresponding scores/values |
|||||
| HT | CHM | |||||
| Vasomotor Symptoms measured by Menopause Specific Quality of Life Questionnaire (MENQOL, monthly) | The mean vasomotor symptoms in the control groups ranged across control groups from 0.36 to 0.45 points, on an 0‐29 questionnaire scale |
The mean vasomotor symptoms was 0.47 points higher in the CHM group than in HT (0.5 lower to 1.44 higher), on an 0‐29 questionnaire scale. | 127 (2 studies) | ⊕⊝⊝⊝ VERY LOW 1 2 | MD 0.47 (‐0.50 to 1.44) MENQOL a 29‐item questionnaire with scale from 0 to 6. A lower score means fewer symptoms. |
|
| Adverse Effects | 60 per 1000 | 57 per 1000 (40 to 83) | RR 0.96 (0.66 to 1.39) | 864 (6 RCTs) | ⊕⊝⊝⊝ VERY LOW 2 3 | Symptoms reported included mild diarrhoea, breast tenderness, gastric discomfort and an unpleasant taste |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
a None of the included studies in this comparison assessed the following primary outcomes: frequency of daily hot flushes; frequency of daily night sweats; severity of daily hot flushes; severity of daily night sweats; overall scores of daily hot flushes; overall scores of daily night sweats measured in a diary.
1Downgraded one level due to serious imprecision (small sample size; confidence interval suggests both benefit and harm).
2 Downgraded two levels due to very serious risk of bias (sequence generation, allocation concealment and blinding of outcome assessors unclear; study participants and personnel not blinded; outcome data incomplete).
3Downgraded one level due to serious imprecision (very wide confidence interval).
Background
Description of the condition
Menopause is defined as the permanent cessation of menses, usually signalling the end of a woman’s reproductive years (Greendale 1999). It is said to have occurred after 12 months of amenorrhoea (the absence of menstrual periods), therefore the time of the final menses can only be determined retrospectively. Menopause may occur naturally as the result of ageing or as a consequence of the following: surgical removal of ovaries, or as a result of radiation, or chemotherapy (Dodin 2013). The mean age of natural menopause is 51 years (Gold 2001; Greendale 1999; Nelson 2008) with most women experiencing menopause with a range of 40 and 58 years of age (NIH 2005). Age at menopause may be affected by various factors such as smoking, socioeconomic status, age at menarche (first menstrual period), parity, previous oral contraceptive use, body‐mass index (BMI), ethnic origin, and family history (Nelson 2008).
Women experience menopause differently; vasomotor complaints such as hot flushes and perspiration being the most commonly reported in the USA and UK, whereas joint pain is a complaint prevalent amongst Asian women (Castel‐Branco 2005; Chim 2002; Dennerstein 2004; Singh 2002). Other common symptoms include loss of libido, dryness and thinning of the skin and vaginal wall, mood swings and depression, osteoporosis, and insomnia. Variations in these clinical symptoms may occur across ethnic groups (Avis 2001; Geller 2006; Haines 2005; Nelson 2008). Symptoms also tend to fluctuate and their severity varies greatly between individuals, ranging from a mere discomfort to severe distress with substantial reduction in the quality of life (Marjoribanks 2012). The average duration of menopausal symptoms is three and a half years (McKinlay 2006), however it can range from five months to 10 years (Leach 2012).
Natural menopause occurs when the ovaries no longer produce eggs (ovulation), and therefore the amounts of the hormones progesterone and oestrogen present in the body decrease significantly.
Description of the intervention
In many countries, women are actively seeking alternative approaches to reduce their menopausal symptoms (Bair 2008; Biddle 2003; Chen 2010; Michelle 2002; Newton 2002). These include vitamins and minerals, plant‐derived dietary supplements, meditation, and traditional Chinese medicine (TCM). TCM is one of the most popular alternative and complementary therapies (Tindle 2005; Xue 2007), with a history of practice exceeding 2000 years. It offers a clear and systematic approach to the management of menopausal symptoms (Scheid 2007). Its therapies, including the use of Chinese herbal medicine (CHM), acupuncture, and specific diets and exercises, are commonly used to relieve menopausal symptoms in Eastern countries (Chen 2010). Recently, the practice of TCM has significantly permeated a broad cross‐section of western communities (Kwee 2007; Zhu 2009).
The forms of CHM preparations are varied; from traditional raw herbs made into a decoction, pills, liniments, plasters and ointments to concentrated powder and liquid extracts prepared by modern pharmaceutical procedures. The routes of administration also differ, either oral, topical, intravenous or injections into specific acupuncture points. Practitioners may choose to select a single herb or a complex formula consisting of several herbal ingredients.
A formula may be used un‐tailored to individual needs and remain unchanged throughout the whole period of clinical intervention; this is known as the standard approach. Conversely, an individualised approach requires prescription of different formulae customised specifically for different individuals or modification of a basic formula during different stages of clinical intervention to respond to clinical changes if present. This is one of the underpinning theoretical constructs of TCM and a number of complementary therapies.
TCM operates under a different theoretical paradigm to the dominant paradigm of Western biomedical science (Zhu 2009). In the case of menopausal symptoms, biomedical science has viewed menopause as the presence of organic conditions (the deficiency of ovaries due to ageing process or various medical interventions), with illness manifesting as changes in structure (e.g. dryness and thinning of skin and vaginal wall, and osteoporosis) and function of the body (such as hot flushes, poor memory, mood swings), observed at the anatomical and physiological levels, and increasingly reliant on laboratory findings for detection (i.e. increased follicle stimulating hormone (FSH) levels, decreased oestrogen and progestogen levels).
In comparison, TCM regards illness as a syndrome or pattern (Zheng), manifesting as a disparate but mutually related set of signs and symptoms occurring throughout the whole body, and may arise from disharmony of the body (Deng 1983). The syndromes or diagnostic categories of TCM describe clinical patterns of both objective signs and subjective symptoms. Although the term 'menopause' does not appear in historical TCM literature, the clinical manifestations were recognised and considered to be related to hypo‐functions of the kidney. Contemporary Chinese medicine gynaecological textbooks such as Gynaecology in TCM (Zhong Yi Fu Ke Xue ) (Luo 1986) also continue to attribute menopause to kidney function: that is, around the cessation of menstruation, the Kidney Qi gradually declines. The fundamental theories and approaches of TCM, reflecting upon the practice of CHM, determine contemporary scientific research and clinical practice in managing menopausal symptoms.
Another key requirement of traditional treatment with CHM is that the treatment has to be tailored to the individual at the outset as well as modified at different stages of the patient's recovery or illness, since the clinical patterns may change during different stages. Hence, a second and distinct diagnostic process is required, as illness labelling (and therefore the treatment process) differs from conventional medical approaches (Zhu 2009). For example, a menopausal woman at onset of transition, a diagnostic pattern “Deficiency of Kidney Yin Resulting in Empty Heat” may be made in accordance with her clinical manifestations, whilst a pattern of “Deficiency of Kidney Yin and Kidney Yang” may be labelled later on when the postmenopausal stage is attained.
These fundamental theories and approaches of TCM, reflecting on the practice of CHM, determines contemporary scientific research in the field of menopausal symptoms. Therefore, it was our intention to rigorously follow the scientific approaches whilst to fully respect the traditional philosophies and practice of Chinese medicine while conducting this systematic review.
How the intervention might work
Chinese herbal medicine is currently used in public hospitals in China for the treatment of menopause. In the last few decades, much research has investigated the efficacy, possible risks, and adverse effects of CHM for the management of menopausal symptoms. A review of the literature of 485 clinical studies (Liu 2008) in 2008 reported that 185 herbs were used to treat menopausal symptoms. Dang Gui (Radix Angelicae sinensis), a commonly used Chinese herb, was most frequently cited. This herb has traditionally been used to treat dysmenorrhoea, irregular menstruation and as a supportive herb for menopausal complaints (Geller 2006; Luo 1986). Dang Gui is reported to act by enhancing oestrogen production (Amato 2002). Ren Shen (Radix Panax ginseng), another commonly used herb (Kronenberg 2002), has also been reported in several publications (Ososki 2003) to have oestrogen‐like effects on vaginal mucosa. Its extract has also been found to compete with estradiol (E2) for oestrogen‐ and progesterone‐binding sites in human myometrial cytosol (Punnonen 1980). This may be due to triterpene saponin, which is a subtype of isoflavone (a type of phyto‐oestrogen) (McBane 2008).
Recommendations for treating menopausal symptoms in the TCM literature are dominated by formulations which usually contain about a dozen herbs with different functions within the TCM framework. The most commonly selected herbal formula is Liu Wei Di Huang Wan, which has been used for more than one thousand years. It is also the most widely used CHM formula for the tonification of the Kidney Yin, as a basic formula for treatment in either pattern of deficiency of Kidney Yin or Kidney Yang (Scheid 2007). Traditional applications listed in the Chinese Pharmacopoeia include hot flushes, night sweating, dizziness, tinnitus, weakness and soreness of limbs and lower back, and fertility dysfunctions (NJUTCM 2006).
In Liu’s review (Liu 2008), the Liu Wei Di Huang Wan formula was the most frequently cited amongst the 73 classic formulae reported in 485 studies. A randomised controlled trial (RCT) conducted by a Dutch research team (Kwee 2007) used Zhi Bai Di Huang Wan (a variation of Liu Wei Di Huang Wan) versus hormone therapy (HT) and placebo to treat menopausal symptoms. The authors concluded that the formula could produce a reduction in frequency of vasomotor symptoms and that overall quality of life was also improved. However, no oestrogen was detected in the herbal formula and the mechanism of the formulation remained uncertain.
Why it is important to do this review
Many questions about menopausal transition and its symptoms have not yet been adequately answered (Nelson 2008). Hormone therapy (HT, oestrogen alone or combined oestrogen with progestogen) is widely used to treat menopausal symptoms (Marjoribanks 2012). However, there are considerable concerns regarding the adverse effects associated with conventional therapies, especially with long‐term use. The major concern is the adverse effects resulting in an increased risk of cardiovascular disease and breast cancer as reported in the Women’s Health Initiative study (Rossouw 2002), as well as other studies (Colditz 2005; Persson 2000; Störk 2004). As outlined in several Cochrane reviews, HT has been associated with an increased incidence of venous thromboembolic events, pulmonary embolus, stroke (Boardman 2015), and gallbladder disease (Marjoribanks 2012). The publication of these results and lack of confidence in pharmacological interventions have resulted in a reduction in the use of HT and an increase in complementary and alternative therapies which may include CHM (Bair 2008; Dodin 2013; Geller 2006; Leach 2012).
Public interest in the use of CHM, as one of the most popular alternatives, for the improvement of menopausal symptoms is likely to increase. Although CHM is generally safe when used properly by qualified practitioners, many herbs and formulae have contraindications, and some can be toxic. Most importantly, the effectiveness and safety of long‐term use of CHM to treat menopausal symptoms is yet to be well developed within the scientific research framework.
Given that the evidence of the safety and effectiveness of Chinese herbs for the treatment of menopausal symptoms is important, there is an urgent need for a systematic review of the available literature so that the unique needs of menopausal women can be addressed and quality of life improved.
Objectives
To evaluate the effectiveness and safety of Chinese herbal medicine (CHM) in the treatment of menopausal symptoms.
Methods
Criteria for considering studies for this review
Types of studies
Only randomised controlled trials (RCTs) considering the effectiveness of CHM in menopause were eligible for inclusion. The status of RCTs was verified and confirmed through contacting the authors of primary studies.
We planned to include cross‐over trials in the review, providing data from the first phase of the trial prior to the cross‐over phase were available, however no cross‐over trials were identified.
Types of participants
Participants were limited to women 18 years of age or older with either spontaneous menopause or induced menopause through surgery or chemotherapy and/or radiotherapy who were experiencing climacteric symptoms.
All women, regardless of any prior or existing morbidity (e.g. cardiovascular disease, fracture, and osteoporosis).
Types of interventions
The interventions included, but were not limited to, the following.
Any CHM versus placebo for menopausal symptoms (this included similar variations of the comparisons, for example one formula with different doses).
Any CHM versus no treatment for menopausal symptoms.
Any CHM versus conventional therapy (e.g. HT) for menopausal symptoms (CHM compared with HT and other types of medication separately; similar variations of the comparisons were also included).
One type of CHM (e.g. oral administration) versus another type of CHM (e.g. topical use) for menopausal symptoms.
Any CHM versus acupuncture for menopausal symptoms.
Note:
Detailed interventions included, but were not limited to, single Chinese herb and Chinese herbal formulae such as fixed/standardised formula and tailored formula.
The route of administration of interventions included, but was not limited to, oral and external use. However, intravenous injection was excluded.
The forms of administration included, but were not limited to, herbal decoctions, herbal extract including powders, liquid, pills/tablets/capsules, and plasters.
Co‐interventions included HT, acupuncture or other traditional Chinese medicine (TCM) therapies.
Types of outcome measures
Primary outcomes
1. Improvement in frequency or severity of vasomotor symptoms (i.e. hot flushes, night sweats); evaluated either subjectively by participants, usually in daily diaries, or by any validated objective scoring system such as the Kupperman Index (Kupperman 1959).
Methods used for evaluation
A diary may be used to capture one or more of these three types of symptoms, hot flushes, night sweats or combination of hot flushes with night sweats. Either frequency or intensity of these symptoms may be measured. For frequency, the daily number of episodes is recorded as one point. As for severity, the total number of hot flush points is calculated by assigning a number to the severity of the hot flush (mild = I, moderate = 2, severe = 3, very severe = 4), and multiplied by the daily number of hot flushes experienced at that severity level. The resulting points may be summed to give a total daily score, and each daily score is averaged over 14 days, before consultation at baseline, after treatment, and at follow‐up (Sloan 2001).
Kupperman Index (KI), also called Kupperman Index Score (KIS), is a questionnaire containing 11 menopausal‐related symptoms. Each symptom is rated from 0 ‐ 3 according to severity and symptoms (where 0 = no symptoms, and 3 = most severe), weighted, and the total sum is calculated with a possible maximum score of 51; higher scores indicate more severe symptoms.
Secondary outcomes
1. Improvement in other menopausal symptoms derived from overall numerical results by using different measurements e.g. Kupperman Index (KI) (Kupperman 1959); Menopause‐Specific Quality of Life Questionnaire (MENQOL) (Hilditch 1996); Greene Climateric Scale (GCS) (Greene 1976); Women's Health Questionnaire (WHQ) (Hunter 1992); Menopause Rating Scale (MRS) (Hauser 1994; Heinemann 2003; Potthoff 2000); and Hot Flash Related Daily Interference Scale (HFRDI) (Carpenter 2001). Chinese studies tended to use different measurements; measuring a successful rate for menopausal symptoms (Ministry of Health of PRC 1995).
Rating scales
The Menopause‐Specific Quality of Life Questionnaire (MENQOL) is interchangable with Menopause Specific Quality of Life (MSQOL). It is a condition‐specific validated measure of Health‐Related Quality of Life (HRQoL). It is a 29‐item questionnaire covering domains of physical, emotional and social aspects which defines if a therapeutic intervention affects an individual’s quality of life specific to menopause symptoms. Participants are asked about their symptoms in the previous month and rate problems on a seven‐point Likert Scale (0 = no bother and 6 = extremely bothered). Systematic scoring for each domain is identical. Each domain is scored by averaging the manipulated values.
Means are computed for each subscale by dividing the sum of the domain’s items by the number of items within that domain. Non‐endorsement of an item is scored a '1' and endorsement a '2' plus the number of the particular rating, so that the possible score on any item ranges from 0 to 8.
The Greene Climateric Scale (GCS) is a 21‐item questionnaire assessing menopausal symptoms in three domains including psychological, physical and vasomotor with four ratings (0 = not at all, 1 = a little, 2 = quite a bit, and 3 = extremely). Lower points indicate better health‐related quality of life rated from 0 to 63.
The Women's Health Questionnaire (WHQ) is a 37‐item questionnaire evaluating nine domains including physical and emotional areas with four‐point scale, with more points indicating more normal disturbance, and less points indicating less normal disturbance.
The Menopause Rating Scale (MRS) is an 11‐item questionnaire covering three dimensions, psychological, somatic and urogenital, with participants marking each question according to severity of symptoms on a scale of 0 to 4. Lower points indicate a better quality of life.
The Hot Flash Related Daily Interference Scale (HFRDI) is used to measure the impact of hot flushes on overall quality of life (item 10) as well as on nine specific activities (items 1 to 9: work, social activities, leisure activities, sleep, mood, concentration, relations with others, sexuality, enjoyment of life). It consists of a series of 0‐ to‐10 point numeric rating scales. Hot flushes are rated based on how much they have interfered with each item during the previous week using a 0 (do not interfere) to 10 (completely interfere) point scale. A total score is computed by summing items. Higher scores indicate higher interference resulted from hot flushes.
Improvement in menopausal symptoms: this method was reported in some of the included Chinese studies. According to the authority standards, outcomes of treatment are generally defined as 'curing' (the major menopausal symptoms have completely disappeared), 'improving' (the symptoms have improved in severity or/and frequency), and 'not responding' (there has been no improvement at all). A successful/unsuccessful rate is usually calculated as the total number of women being cured, or improved, or with no improvement divided by the total number of participants expressed as a percentage. Some studies also considered Chinese medicine diagnostic patterns, which is a unique approach in the practice of TCM when successful or unsuccessful rate is applied. The data (rate) were therefore treated as dichotomous data.
2. Adverse effects, measured as a self‐report of incidence and/or liver and renal function tests.
3. Quality of life measured by a validated scale (e.g. SF‐36, MENQOL (Hilditch 1996).
4. Satisfaction of treatment as reported by women, measured as the proportion of women who reported improvements or satisfaction, or both, with their treatment.
The primary outcome in our protocol was defined as 'improvement in frequency or intensity of vasomotor symptoms (i.e. hot flushes and night sweats) evaluated subjectively by participants, usually in daily diaries or by any validated objective scoring system such as Kupperman Index; however it was noted that the definition failed to provide wider scopes to the research topic, for example, when either hot flushes or night sweats were measured based on overall scores rather than frequency and intensity, and in a few studies, vasomotor symptoms were also measured based on overall scores without distinguishing hot flushes and night sweats. Hence, more relevant outcomes in the review were considered and evaluated accordingly with only KI and MENQOL, which are the most commonly used measurements.
We also modified the secondary outcomes; only overall scores were analysed, subsets of questionnaires were not included.
The relevant outcomes of each comparison are reported as below.
The primary outcome was modified to changes of vasomotor symptoms including:
changes in frequency of hot flushes/night sweats;
changes in intensity of hot flushes/night sweats;
changes in overall scores of hot flushes/night sweats;
changes in overall scores of vasomotor symptoms.
The secondary outcomes are reported accordingly as below:
menopausal symptoms;
adverse effects;
quality of life (QoL);
satisfaction of treatment.
All these changes are notified in the Differences between protocol and review.
Search methods for identification of studies
Electronic searches
The Cochrane Gynaecology and Fertility Group's search strategy was adopted in consultation with the Trial Search Co‐ordinator. Reports which described (or might have described) RCTs of CHM in the treatment of menopause were obtained using the following search strategy.
The Gynaecology and Fertility Group's Specialised Register of Controlled Trials was searched for any trials within the scope in the title, abstract or keyword sections.
The following electronic databases were searched from their inception to March 2015:
Cochrane Central Register of Controlled Trials (CENTRAL 2015, Issue 3), MEDLINE, Embase, CINAHL, AMED, and PsycINFO.
The MEDLINE search was combined with the Cochrane highly sensitive search strategy for identifying randomised trials, which appeared in the searching chapter of The Cochrane Handbook of Systematic Reviews of Interventions (Higgins 2011).
The Embase search was combined with trial filters developed by the Scottish Intercollegiate Guidelines Network (SIGN) (http://www.sign.ac.uk/methodology/filters.html#random)
Other electronic sources of trials included were:‐
Trial registers for ongoing and registered trials ‐ 'Current Controlled Trials' (http://www.controlled‐trials.com/), 'ClinicalTrials.gov' a service of the US National Institutes of Health (http://clinicaltrials.gov/ct2/home) and 'The World Health Organization International Trials Registry Platform search portal' (http://www.who.int/trialsearch/Default.aspx)
Citation indexes (http://scientific.thomson.com/products/sci/)
Conference abstracts in the Web of Knowledge (http://wokinfo.com/)
LILACS database, as a source of trials from the Portuguese and Spanish speaking world (http://bases.bireme.br/cgibin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis&base=LILACS&lang=i&form=F)
PubMed (http://www.ncbi.nlm.nih.gov/pubmed/), the random control filter for PubMed was taken from the chapter on searching in the Cochrane Handbook of Systematic Reviews of Interventions
OpenSIGLE database (http://opensigle.inist.fr/) and Google for grey literature.
We searched one of the commonly used electronic Chinese databases namely The China National Knowledge Infrastructure (CNKI, 1999 to 2015) as recommended by the Gynaecology and Fertility Group.
See appendices for the specific search string used Appendix 1; Appendix 2; Appendix 3; Appendix 4; Appendix 5; Appendix 6; Appendix 7; Appendix 8.
Searching other resources
We handsearched the reference lists of articles retrieved by the search and contacted experts in the field and the manufacturers of CHM in order to obtain additional relevant data.
We handsearched any relevant journals and conference abstracts that were not covered in the Gynaecology and Fertility Group's register, in liaison with the Trial Search Co‐ordinator.
Data collection and analysis
Data collection and analysis were conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Selection of studies
The study selection was undertaken by two review authors (XZ and ZL). The titles and abstracts of articles found by the search were screened by XZ, who discarded studies that were clearly ineligible but aimed to be inclusive rather than risk losing relevant studies. XZ obtained copies of the full‐text articles and made copies for ZL in which details of the authors and institutions had been struck out and the results section removed. Both review authors independently assessed whether the studies met the inclusion criteria, and disagreements were resolved by discussion. Further information was sought from the authors where papers contain insufficient information to enable assessment for eligibility.
Data extraction and management
All assessments on the quality of trials and data extraction were performed independently by the two review authors (XZ and ZL). Data were extracted onto a pre‐developed data extraction sheet to assess study characteristics including the location of the study, methods of the study (as per quality assessment checklist), the participants (age range, eligibility criteria), the nature of the interventions, and data relating to the outcomes specified above. Any discrepancies were resolved by a third review author (YL).
Additional information on the trial methodology or actual original trial data were sought from the principal author of those trials that appeared to meet the eligibility criteria, when aspects of methodology were unclear, or where the data were in a form unsuitable for meta‐analysis.
Assessment of risk of bias in included studies
The included studies were assessed for risk of bias using the Cochrane 'Risk of bias' assessment tool to assess the following domains: sequence generation; allocation concealment; blinding of participants, providers and outcome assessors; completeness of outcome data; selective outcome reporting; and other potential sources of bias. Two review authors (XZ and ZL) assessed these six domains, with any disagreements resolved by consensus or by discussion with the third review author (YL). All judgments were fully described and presented in the ‘Risk of bias' tables in accordance with the standards as below.
Sequence generation
Low risk of bias: the method used was considered either adequate (e.g. computer‐generated random numbers, table of random numbers) or unlikely to introduce confounding.
Uncertain risk of bias: there was insufficient information to assess whether the method used was likely to introduce confounding.
Allocation concealment
Low risk of bias: the method used (e.g. central allocation) was unlikely to induce bias on the final observed effect.
Uncertain risk of bias: there was insufficient information to assess whether the method used was likely to induce bias on the estimate of effect.
High risk of bias: the method used (e.g. open random allocation schedule) was likely to induce bias on the final observed effect.
Blinding
Low risk of bias: the trial was described as blinded, the parties that were blinded, and the method of blinding was described, so that knowledge of allocation was adequately prevented during the trial.
Uncertain risk of bias: the trial was described as blinded, but the method of blinding was not described, so that knowledge of allocation was possible during the trial.
High risk of bias, the trial was not blinded, so that the allocation was known during the trial.
Incomplete outcome data
Low risk of bias: the numbers and reasons for dropouts and withdrawals in all intervention groups were described, or if it was specified that there were no dropouts or withdrawals.
Uncertain risk of bias: the report gave the impression that there had been no dropouts or withdrawals, but this was not specifically stated.
High risk of bias: the number or reasons for dropouts and withdrawals were not described or dropout rates were high.
Selective outcome reporting
Low risk of bias: predefined, or clinically relevant and reasonably expected outcomes were reported.
Uncertain risk of bias: not all predefined, or clinically relevant and reasonably expected outcomes were reported, or were not reported fully, or it was unclear whether data on these outcomes were recorded or not.
High risk of bias: one or more clinically relevant and reasonably expected outcomes were not reported; data on these outcomes were likely to have been recorded.
Other bias
In addition to the above‐mentioned biases, industry, academic, or other bias that could be detected were also considered.
Low risk of other bias: the trial appeared to be free of any risk of bias.
Uncertain risk of bias: the trial may or may not have been free of any risk of bias.
High risk of other bias: there were other factors in the trial that could lead a risk of bias; for example, unequal groups as baseline.
Measures of treatment effect
Statistical analyses were performed in accordance with the guidelines described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
For continuous outcome data, results from each study were expressed as a difference in means with 95% confidence intervals and combined for meta‐analysis using the mean difference (MD) if all studies reported exactly the same outcomes. Where different scales were used to report the same outcomes (e.g. hot flushes); we planned to use the standardised mean difference (SMD).
Ordinal data (e.g. quality of life (QoL) scores) were treated as continuous data and 95% confidence intervals were presented for all outcomes. A random‐effects approach was used to calculate summary effect measures, as a priori it was expected that analyses would have heterogeneous results.
For binary outcomes, results for each study were expressed as risk ratios (RR) with 95% confidence intervals and combined for meta‐analysis using the Peto method.
Confidence intervals (95%) were presented for all outcomes and comparisons.
Unit of analysis issues
Dichotomous outcomes were analysed as per woman randomised (e.g. number of women with an adverse effect/total number of women randomised). When data were presented in continuous form, the data were treated so participants from individual trials were included only once in each comparison.
Dealing with missing data
We contacted the primary authors of studies by email to obtain any missing participant data and we recorded the rate of contact. When we were unable to obtain missing data, analyses were based on populations in which outcomes were reported. Discrepancies between the number of participants enrolled and number for whom outcomes were reported were noted in the Characteristics of included studies table. Data were analysed on an intention‐to‐treat basis when available.
Assessment of heterogeneity
We considered heterogeneity when clinical and methodological characteristics of included studies were suitable for a meta‐analysis. Statistical analyses were performed in accordance with the guidelines for statistical analysis described in Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Heterogeneity was identified by visual inspection of the forest plots with a standard Chi2. Heterogeneity (variation) between the results of different studies was specifically examined by using the I2 statistic (a quantity that describes approximately the proportion of variation in point estimates that is due to heterogeneity rather than sampling error), which can be interpreted when I2 was identified at the following ranges.
0% to 40%: might not be important.
30% to 60%: represents moderate heterogeneity.
50% to 90%: represents substantial heterogeneity.
75% to 100%: represents considerable heterogeneity (Higgins 2011).
If an I2 was between 50% and 85%, we used a random‐effects model for analysis. If an I2 was greater than 85%, meta‐analysis was not performed. Pre‐determined subgroup analyses according to standard formulation and individualised formulation (data were not available) were preformed in order to explore the cause(s) of heterogeneity.
Assessment of reporting biases
In view of the difficulty in detecting and correcting for publication bias and other reporting biases, we aimed to minimise their potential impact by ensuring a comprehensive search for eligible studies and by being alert for duplication of data. We planned to prepare a funnel plot if there were 10 or more studies in one analysis, however, too few studies were identified for a funnel plot construction.
Data synthesis
The data from primary studies were combined in the following comparisons:
CHM versus placebo;
CHM versus active medications (including HT);
CHM versus another CHM (including comparisons between different doses).
No study reported on CHM versus no treatment.
An increase or decrease in the odds of a particular outcome, which may be beneficial or detrimental, were displayed graphically in the meta‐analyses. An increase in the odds of an outcome was displayed to the right of the centre line while a decrease in the odds of an outcome was displayed to the left of the centre line.
When meta‐analyses were conducted, either random‐effects model or fixed‐effect model might be used. When there was no significant or substantial heterogeneity (an I2 less than 50%), only results from the fixed‐effect model were presented. When heterogeneity was over 85%, meta‐analysis was not performed, since the effect estimate did not reflect the 'true' value, hence a narrative, qualitative summary was provided instead.
In the event of high clinical, methodological or statistical heterogeneity, we did not combine study results by means of meta‐analysis, but instead, summarised them in narrative form.
Subgroup analysis and investigation of heterogeneity
The protocol stated that where data were available, subgroup analyses would be conducted to determine the evidence of different types of Chinese herbal formulation, that is, standard formulation and individualised formulation, in order to investigate heterogeneous results. Since the data were unavailable, subgroup analysis was not undertaken.
Sensitivity analysis
We undertook a sensitivity analysis for the primary outcomes to determine whether review conclusions would have differed if eligibility were restricted to studies deemed at low risk of bias.
The following aspects of quality were considered for this sensitivity analysis: inadequate blinding, non‐comparable groups (because they had different baseline characteristics), and no intention‐to‐treat analysis.
Overall quality of the body of evidence: Summary of findings tables
We prepared two Summary of findings tables using GRADEPRO, see Table 1; Table 2. These tables evaluate the overall quality of the body of evidence for the main review outcomes: vasomotor symptoms were assessed by different aspects, including frequency of hot flushes, severity of hot flushes, overall hot flushes, and overall night sweats. Vasomotor symptoms were also assessed by validated questionnaires, including the modified Kupperman Index Scale (KIS), the Menstrual‐Specific Quality of Life (MENQOL), the Green Climacteric Scale (GCS) and the Menopause Rating Scale (MRS). The GRADE criteria including study limitations (i.e. risk of bias), consistency of effect, imprecision, indirectness and publication bias were adopted. Judgements about evidence quality (high, moderate or low) were justified, documented, and incorporated into reporting of results for each outcome in relation to the primary outcome.
Reliable synthesis was not possible in our other comparisons (CHM versus conventional therapy (fluoxetine & estazol) and CHM versus another CHM) where small studies reported only one secondary outcome. Because of insufficient data we did not present a summary of findings table for these comparisons.
Results
Description of studies
Results of the search
The search retrieved 864 articles. Twenty‐eight studies were potentially eligible and we retrieved the full‐text articles. Twenty‐two studies met our inclusion criteria. Six studies were excluded. For detailed information, see study tables: Characteristics of included studies and Characteristics of excluded studies. We prepared a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta‐Analyses) flow diagram to describe the publications found through our searches (Figure 1).
1.
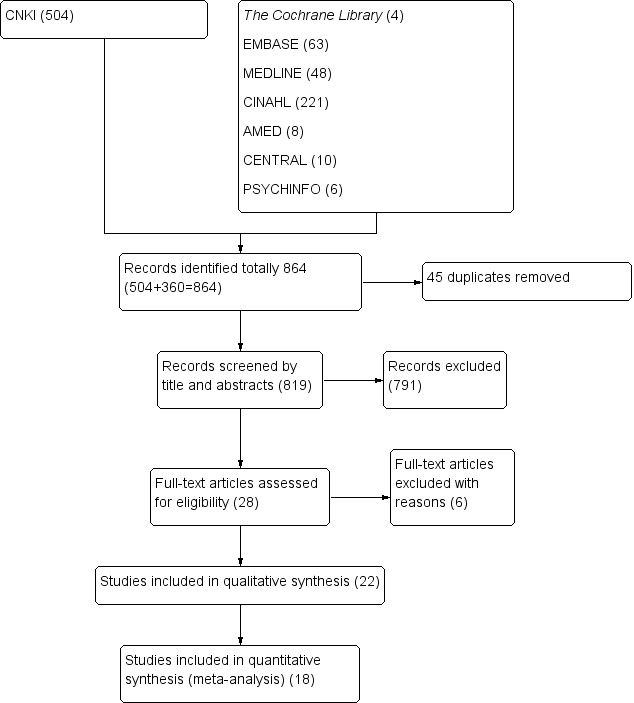
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta‐Analyses) flow‐chart of study selection.
Included studies
Study design and setting
Twenty‐two parallel‐design randomised controlled trials (RCTs) were included in the review (Azizi 2011; Deng 2011; Gong 2008; Guo 2009; Haines 2008; Jing 2002; Kwee 2007; Li 2009; Liang 2003; Lou 2009; Plotnikoff 2011; Qu 2009; Tao 2009; van der Sluijs 2009; Wu 2013; Xia 2012; Xue 2011; Zhang 2009; Zhang 2012; Zhong 2013; Zhou 2007; Zhou 2009). All were single‐centre studies with three studies conducted in outpatient clinics in Australia (van der Sluijs 2009), The Netherlands (Kwee 2007) and the USA (Plotnikoff 2011). The majority of studies, (19) were conducted in China, including two in Hong Kong (Haines 2008; Zhong 2013).
Participants The studies included 2902 women with a total of 1499 participants in the intervention groups and 1403 in the control groups. Women were diagnosed with menopause by one or more of the following assessment items including gynaecological examination, serum hormone levels (follicle stimulating hormone (FSH) > ranged from 4 to 40 IU/L, luteinizing hormone (LH) > 12.6 IU/L, and E2 < ranged from 20 to 361 pg/mL), and menstrual scores. Nine out of the 22 studies also considered a specific Chinese medicine diagnostic pattern as one of the key inclusion criteria (Azizi 2011; Deng 2011; Guo 2009; Kwee 2007; Li 2009; Plotnikoff 2011; Tao 2009; Xue 2011; Zhang 2012).
Menopause symptoms
The menopausal symptoms reported in the studies varied widely. In terms of descriptive symptoms, there were hot flushes, night sweats, combination of these two symptoms, symptoms of hot flushes and night sweats with emotional disturbance and sleep problems. The tools for measuring these symptoms also varied across the studies, for example, hot flushes might be measured alone as intensity, or frequency; or might be assessed as part of overall symptoms.
Interventions and controls
No study compared Chinese herbal medicine (CHM) versus no treatment.
8/22 studies compared CHM versus placebo (including one study that compared CHM plus placebo versus placebo).
10/22 studies compared CHM versus conventional therapy, specifically hormone therapy (HT), (including one study that compared CHM plus placebo versus HT plus placebo.
2/22 studies compared CHM versus conventional therapy (other than HT).
2/22 studies compared CHM versus another formula of CHM.
No study compared CHM versus acupuncture.
Formulae and Ingredients: There was huge variation in formulations: 21 formulae with 91 herbal ingredients were tested. However there was a tendency to use certain herbs in menopause research, for example, the following 11 herbs were identified as the most frequently tested. The list below reports how often and which herbs were used in the relevant included studies in detail.
Herbs tested
Bai Shao Yao Radix Paeoniae Alba (eight studies) (Azizi 2011; Jing 2002; Plotnikoff 2011; Wu 2013; Xue 2011; Zhang 2012; Zhou 2007; Zhou 2009).
Dang Gui Radix Angelicae Sinensis (seven studies) (Azizi 2011; Haines 2008; Jing 2002; Wu 2013; Zhang 2009; Zhong 2013; Zhou 2007).
Di Huang Radix Rehmanniae Preparata (seven studies) (Azizi 2011; Kwee 2007; Liang 2003; Wu 2013; Zhang 2009; Zhang 2012; Zhou 2009).
Fu Ling Poria (seven studies) (Kwee 2007; Li 2009; Liang 2003; Plotnikoff 2011; Wu 2013; Zhang 2009; Zhou 2009).
Zhi Mu Rhizoma Anemarrhenand (six studies) (Azizi 2011; Jing 2002; Kwee 2007; van der Sluijs 2009; Zhang 2009; Zhong 2013).
Shan Yao Rhizoma Dioscoreae Oppositae (six studies) (Deng 2011; Kwee 2007; Li 2009; Liang 2003; Qu 2009; Wu 2013).
Suan Zao Ren Semen Z spinosae (five studies) (Azizi 2011; Jing 2002; Qu 2009; van der Sluijs 2009; Zhang 2009).
Shan Zhu Yu/ShanYu Rou Fructus Corni (five studies) (Kwee 2007; Liang 2003; Wu 2013; Zhang 2009; Zhang 2012).
Mu Dan Pi Cortex Moutan Radicis (five studies) (Deng 2011; Jing 2002; Kwee 2007; Liang 2003; Plotnikoff 2011).
Yin Yang Huo Herba Epimedii (four studies) (Deng 2011; Li 2009; Lou 2009; van der Sluijs 2009).
Dan Shen Radix Salviae Miltiorrhizae (four studies) (Liang 2003; Wu 2013; Xia 2012; Zhang 2009).
Huang Bai Cortex Phellodendri (three studies) (Jing 2002; Kwee 2007; van der Sluijs 2009).
Styles of formulation : 20/22 studies investigated a standard formula throughout the trial period. Only one study (Guo 2009), looked into a few tailored formulae for women diagnosed with different traditional Chinese medicine (TCM) diagnostic patterns, but used throughout the course of the intervention without modification; one study (Kwee 2007), adapted an approach with a standard formula adding limited modifications in herb compositions. Interestingly, no study assessed the use of just a single herb or a complete individualised approach (i.e. each patient is given as many different formulae as possible based on individual clinical presentation, and a formula may be changed during the course of intervention, which is the typical TCM diagnostic approach).
Forms of herbs: The most popular form of CHM was herbal extract in the form of granules which was used in 17/22 studies (Azizi 2011; Deng 2011; Gong 2008; Haines 2008; Jing 2002; Kwee 2007; Li 2009; Liang 2003; Lou 2009; Plotnikoff 2011; Tao 2009; van der Sluijs 2009; Xia 2012; Xue 2011; Zhong 2013; Zhou 2007; Zhou 2009); only five studies used a traditional form as a decoction (Guo 2009; Qu 2009; Wu 2013; Zhang 2009; Zhang 2012. All herbs were administered internally.
Reporting involved herbs and dosages: 14/22 studies reported full compositions of the herbal formulae (Azizi 2011; Guo 2009; Haines 2008; Liang 2003; Plotnikoff 2011; Qu 2009; Tao 2009; van der Sluijs 2009; Wu 2013; Xia 2012; Zhang 2009; Zhang 2012; Zhong 2013; Zhou 2007). By contrast, eight studies did not report full ingredients used in their studies (Deng 2011; Gong 2008; Jing 2002; Kwee 2007; Li 2009; Lou 2009; Xue 2011; Zhou 2009). Eleven studies mentioned the full dosages of the involved ingredients (Guo 2009; Liang 2003; Qu 2009; Tao 2009; van der Sluijs 2009; Wu 2013; Xia 2012; Zhang 2009; Zhang 2012; Zhong 2013; Zhou 2007); information on full dosages of the studied ingredients was missing in the remaining 11 studies (Azizi 2011; Deng 2011; Gong 2008; Haines 2008; Jing 2002; Kwee 2007; Li 2009; Lou 2009; Plotnikoff 2011; Xue 2011; Zhou 2009).
Length of intervention: the lengths of trial period varied from a period of four weeks to 106 weeks, however a substantial number of the included studies (9/22) were for 12 weeks (Jing 2002; Kwee 2007; Liang 2003; Plotnikoff 2011; Qu 2009; Wu 2013; Xia 2012; Zhong 2013; Zhou 2007). A period of four weeks as intervention period was used in four studies (Guo 2009; Xue 2011; Zhang 2009; Zhang 2012); eight weeks in three studies (Azizi 2011; Lou 2009; Tao 2009); only one study had a 16‐week intervention (van der Sluijs 2009) and one study a 106‐week intervention, which was extremely long (Li 2009); two studies had a period as long as 24 weeks (Deng 2011; Haines 2008) and 52 weeks (Gong 2008; Zhou 2009).
Length of lead‐in and follow‐up periods: Only three studies had a lead‐in period from one week (Plotnikoff 2011), to two weeks (Zhong 2013), and four weeks (van der Sluijs 2009). Three studies had a follow‐up with either a period of four weeks (Kwee 2007),eight weeks (van der Sluijs 2009), or 12 weeks (Zhong 2013).
Outcomes
6/22 studies reported vasomotor symptoms (Haines 2008; Haines 2008; van der Sluijs 2009; Xia 2012; Zhong 2013; Zhou 2009).
12/22 reported menopausal symptoms (Azizi 2011; Deng 2011; Wu 2013; Li 2009; Guo 2009Lou 2009; van der Sluijs 2009; Zhou 2007; Zhou 2009; Zhong 2013; Xia 2012; Haines 2008).
2/22 reported quality of life in general (Kwee 2007; Zhou 2009).
16/22 reported adverse effects (Azizi 2011; Deng 2011; Gong 2008; Haines 2008; Li 2009; Lou 2009; Plotnikoff 2011; Qu 2009; van der Sluijs 2009; Xia 2012; Xue 2011; Zhang 2009; Zhang 2012; Zhong 2013; Zhou 2007; Zhou 2009).
No study reported the outcome of satisfaction of treatment.
13/22 reported levels of hormone changes (Azizi 2011; Deng 2011; Gong 2008; Jing 2002; Li 2009; Liang 2003; Lou 2009; Qu 2009; Tao 2009; Wu 2013; Xue 2011; Zhong 2013; Zhou 2007), however these were not outcomes of interest in the review.
The way of reporting the primary outcome in the review was slightly modified for clarity.
Changes of vasomotor symptoms were measured by the following methods.
Frequency of hot flushes/night sweats
Severity of hot flushes/night sweats
Overall scores of hot flushes/night sweats (frequency and severity)
Overall scores of vasomotor symptoms (hot flushes and night sweats)
The secondary outcomes were assessed according to the following order.
Menopausal symptoms
Adverse effects
Quality of life (QoL)
Satisfaction of treatment
See Differences between protocol and review for the modifications made and the rationale.
Excluded studies
Six studies were excluded from the review, for the following reasons.
One study was not true RCT
One study reported with data not retrievable (when the corresponding author of this study was contacted on several occasions, it was reported that there was no original data available for any clarification, this study was therefore excluded due to concerns regarding the quality of study)
Three studies reported primary outcomes that were not of interest for this review such as hypotension, eye conditions and psychological disorders
One study investigated different dosages in one formula
Risk of bias in included studies
Allocation
Sequence generation
All 22 studies were at low risk of selection bias in relation to sequence generation, either computer‐generated randomisation or a random numbers table was used.
Allocation concealment
Sixteen studies did not report how allocation concealment was carried out (Deng 2011; Gong 2008; Guo 2009; Jing 2002; Kwee 2007; Li 2009; Liang 2003; Lou 2009; Qu 2009; Tao 2009; Wu 2013; Xue 2011; Zhang 2009; Zhang 2012; Zhou 2007; Zhou 2009). Only five studies reported that allocation concealment was implemented, therefore was considered to have at low risk of selection bias (Haines 2008; Plotnikoff 2011; van der Sluijs 2009; Xia 2012; Zhong 2013). One study did not carry out allocation concealment, resulting in a high risk of bias (Azizi 2011). Detailed information is shown in Figure 2 and Figure 3.
2.
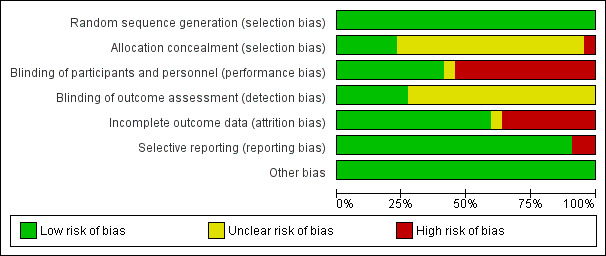
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
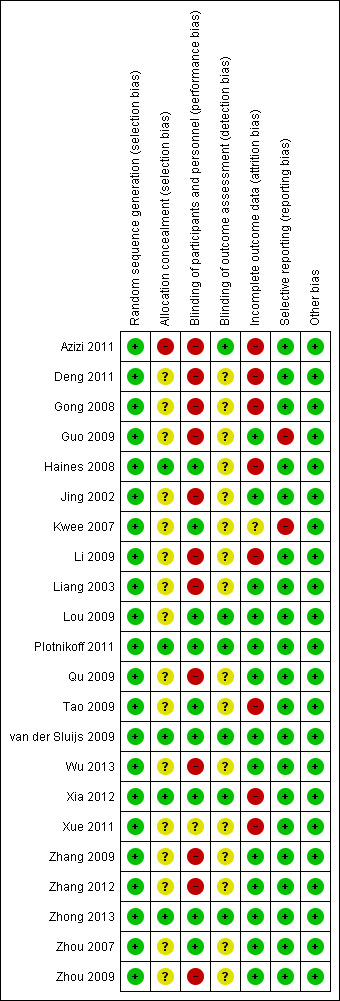
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Blinding
In nine studies participants and personnel were blinded (Haines 2008; Kwee 2007; Lou 2009; Plotnikoff 2011; Tao 2009; van der Sluijs 2009; Xia 2012; Zhong 2013; Zhou 2007), but 12/22 participants and personnel were not blinded (Azizi 2011; Deng 2011; Gong 2008; Guo 2009; Jing 2002; Li 2009; Liang 2003; Qu 2009; Wu 2013; Zhang 2012;Zhang 2009Zhou 2009); in the remaining study it was unclear if blinding was undertaken (Xue 2011). Given that more than fifty per cent of included studies did not introduce appropriate blinding methods, performance bias and detection bias existed, which partially influenced the primary outcome. However, non blinding occurred mainly in the studies in which CHM was compared against HT, and we did not consider that blinding was likely to influence findings for the objective secondary outcomes such as changes in levels of the hormones and lipids; adverse effects were also unlikely to be affected.
Eight included studies compared CHM with placebo (Haines 2008; Kwee 2007; Lou 2009; Plotnikoff 2011; van der Sluijs 2009; Xia 2012; Zhong 2013; Zhou 2007); all of these studies described the use of a placebo identical to the intervention and were thus deemed to be at low risk of performance bias.
In regards to blinding of outcome assessors, six included studies described blinding of outcome assessors, which appeared to be at low risk of detection bias (Azizi 2011; Lou 2009; Plotnikoff 2011; van der Sluijs 2009; Xia 2012; Zhong 2013). However, the remaining 16 studies did not report if outcome assessors including data entry personnel and statisticians were blinded (Deng 2011; Gong 2008; Guo 2009; Haines 2008; Jing 2002; Kwee 2007; Li 2009; Liang 2003; Qu 2009; Tao 2009; Wu 2013; Xue 2011; Zhang 2009; Zhang 2012; Zhou 2007; Zhou 2009).
Incomplete outcome data
We judged 13 studies with 1240 women randomised and analysed to be at low risk of bias (Guo 2009; Jing 2002; Liang 2003; Lou 2009; Plotnikoff 2011; Qu 2009; van der Sluijs 2009; Wu 2013; Zhang 2009; Zhang 2012; Zhong 2013; Zhou 2007; Zhou 2009).
Eight studies with 1640 women were considered to be at high risk of attrition bias with either intention‐to‐treat (ITT) being not mentioned or not implemented (Azizi 2011; Deng 2011; Gong 2008; Haines 2008; Kwee 2007; Tao 2009; Xia 2012; Xue 2011).
One study was rated as unclear (Kwee 2007).
Selective reporting
All expected aspects were reported in 20/22 included studies (Azizi 2011; Deng 2011; Gong 2008; Haines 2008; Jing 2002; Li 2009; Liang 2003; Lou 2009; Plotnikoff 2011; Qu 2009; Tao 2009; van der Sluijs 2009; Wu 2013; Xia 2012; Xue 2011; Zhang 2009; Zhang 2012; Zhong 2013; Zhou 2007; Zhou 2009), which we judged to be at low risk of bias. Two studies did not report expected outcomes (Kwee 2007), or had no pre‐specified outcomes (Guo 2009) and both were deemed to be at high risk of bias.
Other potential sources of bias
We found no potential sources of within‐study bias in the 22 studies. Detailed information is shown in Figure 2 and Figure 3.
Effects of interventions
In terms of comparisons, results in this review are reported according to the following sequence.
CHM versus placebo
-
CHM versus no treatment
including CHM + placebo versus placebo
CHM + conventional therapy (drug as short term) versus placebo + conventional therapy (drug)
-
CHM versus conventional therapy (HT)
including CHM + placebo versus conventional therapy (HT) + placebo
CHM versus conventional therapy (drug)
CHM versus another CHM (different formulations)
CHM versus acupuncture
See Differences between protocol and review for minor changes and rationale.
The relevant outcomes of each comparison are reported as below.
The primary outcome was modified for clarity as changes of vasomotor symptoms including:
frequency of hot flushes/night sweats;
severity of hot flushes/night sweats;
overall scores of hot flushes/night sweats (i.e. combination of frequency and severity);
overall scores of vasomotor symptoms (i.e. combination of hot flushes and night sweats).
The secondary outcomes are reported accordingly as below:
menopausal symptoms measured by different instruments;
adverse effects;
quality of life (QoL);
satisfaction of treatment.
Note: see 'Difference between protocol and review' for the modifications and rationale.
1. Comparison of CHM versus placebo
Seven studies compared CHM against placebo (Haines 2008; Lou 2009; Plotnikoff 2011; van der Sluijs 2009; Xia 2012; Zhong 2013; Zhou 2007); one study compared CHM plus placebo against placebo (Kwee 2007).
Primary outcomes
1.1 Vasomotor symptoms (hot flushes/night sweats)
1.1.1 Frequency of hot flushes in a diary (daily)
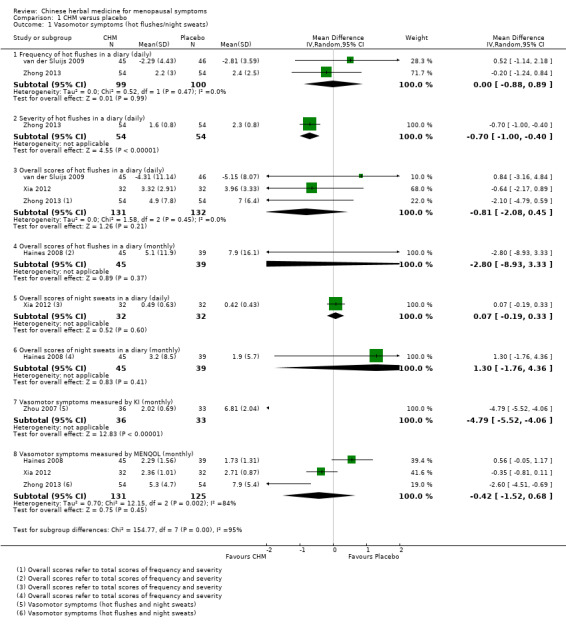
This reports daily hot flushes that were measured by frequency in a diary. Two studies (van der Sluijs 2009; Zhong 2013) reported this outcome. There was no evidence of a difference between the CHM group and the placebo group (mean difference (MD) 0.00 points, 95% confidence interval (CI) ‐0.88 to 0.89; 2 RCTs, 199 women). Heterogeneity was presented as Chi² = 0.52, df = 1 (P = 0.47); I² = 0% (Analysis 1.1; Figure 4). This evidence was rated as low quality using GRADE criteria. See Table 1.
1.1. Analysis.
Comparison 1 CHM versus placebo, Outcome 1 Vasomotor symptoms (hot flushes/night sweats).
4.
Forest plot of comparison: 1 CHM versus Placebo, outcome: 1.1 Vasomotor symptoms (hot flushes/night sweats).
1.1.2 Frequency of night sweats in a diary (daily)
No data available.
1.1.3 Severity of hot flushes in a diary (daily)
This reports daily hot flushes that were measured by severity in a diary. Only one study reported this outcome (Zhong 2013), with a difference between the CHM group and the placebo, in favour of the CHM group (MD ‐0.70 points, 95% CI‐1.00 to ‐0.40; 1 RCT, 108 women (Analysis 1.1; Figure 4). This evidence was rated as high quality using GRADE criteria. See Table 1.
1.1.4 Severity of night sweats in a diary (daily)
No data available.
1.1.5 Overall scores of hot flushes in a diary (daily)
This reports overall scores of hot flushes (including frequency and severity), which were measured in a diary as daily data. Data from three studies (van der Sluijs 2009; Xia 2012; Zhong 2013) were suitable for meta‐analysis; they reported hot flushes with overall scores in diary. The difference in the mean overall hot flushes measured by daily record between CHM groups and the placebo groups was not significant (MD ‐0.81 points, 95% CI ‐2.08 to 0.45; 3 RCTs, 263 women), with no heterogeneity (I² = 0%) (Analysis 1.1; Figure 4). This evidence was rated as low quality using GRADE criteria. See Table 1.
There was no evidence of a difference between the groups in a sensitivity analysis removing the study at other than low risk of bias (Xia 2012) (MD ‐1.02 points, 95% CI ‐3.80 to 1.76; 2 RCTs, 199 women).
1.1.6 Overall scores of hot flushes in a diary (monthly)
This reports overall scores of hot flushes (including frequency and severity), which were measured monthly in a diary. One study (Haines 2008) reported a set of monthly data which was analysed accordingly, there was no difference between the two groups (MD ‐2.80 points, 95% CI ‐ 8.93 to 3.33; 1 RCT, 84 women) Analysis 1.1, Figure 4. This evidence was rated as moderate using GRADE criteria. See Table 1.
1.1.7 Overall scores of night sweats in a diary (daily)
This reports overall night sweats (including frequency and severity), which were measured using daily recorded data. One study (Xia 2012) reported overall night sweats (measured daily). There was no evidence of a difference between the groups (MD 0.07 points, 95% CI ‐0.19 to 0.33; 1 RCT, 64 women) (Analysis 1.1; Figure 4). This evidence was rated as moderate quality using GRADE criteria. See Table 1.
1.1.8 Overall scores of night sweats in a diary (monthly)
This reports overall night sweats (including frequency and severity), which were measured in a diary as monthly data. One study (Haines 2008) reported overall night sweats (measured monthly). There was no evidence of a difference between the groups (MD 1.30 points, 95% CI ‐1.76 to 4.36; 1 RCT, 84 women) (Analysis 1.1; Figure 4). This evidence was rated as moderate quality using GRADE criteria. See Table 1.
1.1.9 Vasomotor symptoms measured by the Kupperman Index (KI) (monthly)
When vasomotor symptoms (including hot flushes and night sweats) were measured monthly, different questionnaires were used. Four studies assessed overall vasomotor symptoms with the following outcome measures, including the KI (Zhou 2007) and the Menopausal Specific Quality of Life (MENQOL) (Haines 2008; Xia 2012; Zhong 2013). Data from the four studies were not suitable for meta‐analysis due to high heterogeneity when the MD was calculated (I2 = 96%). Outcomes measured by KI and MENQOL were analysed separately.
Individually, the study (Zhou 2007) using the KI reported that overall vasomotor symptom scores were lower in the CHM group (MD ‐4.79 points, 95% CI ‐5.52 to ‐4.06; 1 RCT, 69 women). This evidence was rated as low quality using GRADE criteria. See Table 1.
Vasomotor symptoms were also measured by MENQOL in three studies (Haines 2008; Xia 2012; Zhong 2013) and there was no evidence of a difference between the groups (MD ‐0.42 points, 95% CI ‐1.52 to 0.68; 3 RCTs, 256 women); the heterogeneity was high (P = 0.002; I² = 84%) (Analysis 1.1; Figure 4). This evidence was rated as low quality using GRADE criteria. See Table 1.
There was evidence of a difference between the groups in a sensitivity analysis removing the studies at other than low risk of bias (Haines 2008; Xia 2012) (MD ‐2.60 points, 95% CI ‐4.51 to ‐0.69; 1 RCT, 108 women).
Secondary outcomes
1.2 Menopausal symptoms measured monthly
Six studies reported monthly data, however only overall data were analysed from four studies, subset data measuring physical, psychosocial, sexual aspects from other two studies were not considered for analysis. The four studies used three different tools to measure the menopausal symptoms, the heterogeneity was very high (I2 = 98%), hence, results were unpooled, instead, subtotal analysis was chosen, given that different measurements were adopted (Analysis 1.2).
1.2. Analysis.
Comparison 1 CHM versus placebo, Outcome 2 Menopausal symptoms measured monthly.
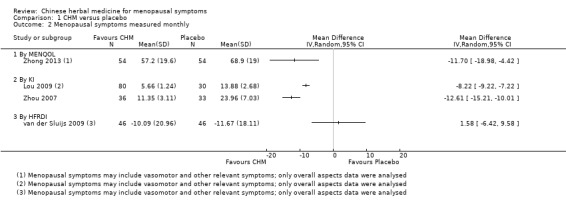
One study (Zhong 2013) assessing the overall scores measured by Menopausal Specific Quality of Life Questionnaire (MENQOL, scale 0 to 6) demonstrated a difference between the comparison groups (MD ‐11.70 points, 95% CI ‐18.98 to ‐4.42; 108 women) (Analysis 1.2). This study also used the Menopause Rating Scale(MRS) to measure overall menopausal symptoms, but this was not included in our analysis to avoid over counting.
Data from the studies using the Kupperman Index (KI, overall scores, scale 0 to 3) were not suitable for meta‐analysis due to high heterogeneity (Chi² = 9.52, df = 1 (P < 0.002), I² = 89%). Individually, Lou and colleagues (Lou 2009) and Zhou and colleagues (Zhou 2007) reported that CHM was better than placebo in improving the monthly overall menopausal symptom scores (MD ‐8.22 points, 95% CI ‐9.22 to ‐7.22; 1 RCT, 110 women and MD ‐12.61 points, 95% CI ‐15.21 to ‐10.01; 1 RCT, 99 women, respectively).
One study (van der Sluijs 2009) did not find any evidence of a difference between the two groups when overall menopausal symptoms were measured by the Hot Flash‐Related Daily Interference Scale (HFRDI, scale 0 to 10) (MD 1.58 points, 95% CI ‐6.42 to 9.58; 1 RCT, 92 women) (Analysis 1.2).
In summary, measures of overall menopausal symptoms were unsuitable for pooling due to high heterogeneity, and findings were inconsistent. When menopausal symptoms were compared by using the KI and MENQOL, there was some suggestion of improvement in the three studies, however there was little evidence of a difference between the groups in the fourth study, which used the HFDRI.
1.3 Improvement in menopausal symptoms
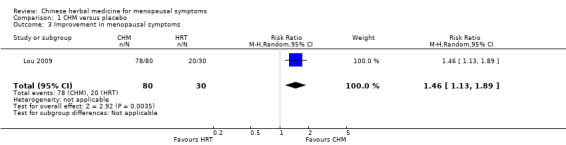
Improvement in menopausal symptoms: this was reported in one Chinese study and was treated as dichotomous data (Lou 2009), the study showed a difference between CHM and placebo, favouring CHM (risk ratio (RR) 1.46; 95% CI 1.13 to 1.89; 1 RCT, 110 women) (Analysis 1.3).
1.3. Analysis.
Comparison 1 CHM versus placebo, Outcome 3 Improvement in menopausal symptoms.
1.4 Adverse effects
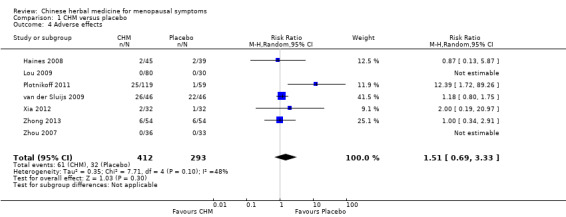
All seven studies (705 women) reported adverse effects as one of the study outcomes. A total of 61 adverse events were reported in 412 women assigned to CHM and 32 adverse events in 293 women assigned to placebo. Two studies claimed no adverse events occurred which was not estimable in analysis (Lou 2009; Zhou 2007). There was no evidence of a difference between the groups (RR 1.51; 95% CI 0.69 to 3.33; 7 RCTs, 705 women, I² = 48%). (Analysis 1.4).
1.4. Analysis.
Comparison 1 CHM versus placebo, Outcome 4 Adverse effects.
1.5 Quality of life (QoL)
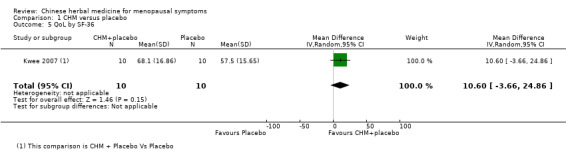
No study reported the QoL specifically in the comparison of CHM versus placebo. One study (Kwee 2007), explored a model of a trial with a double‐dummy design; the data were split into two comparisons, CHM plus placebo versus placebo, and CHM plus placebo versus HT plus placebo.
Quality of life was assessed by SF‐36 (0 to 100 scale). Data in the published report were not available, but were successfully retrieved when the author was contacted. There was no evidence of a difference between the two groups (MD 10.60 points, 95% CI ‐3.66 to 24.86; 1 RCT, 20 women) (Analysis 1.5).
1.5. Analysis.
Comparison 1 CHM versus placebo, Outcome 5 QoL by SF‐36.
1.6 Satisfaction with treatment
No study reported this outcome.
2. Comparison of CHM versus no treatment
No study was found for inclusion in the review.
3. Comparison of CHM plus drug versus placebo plus drug
Only one study used this comparison model (Tao 2009), but no data were available on primary and secondary outcomes.
4. Comparison of CHM versus conventional therapy (HT)
Nine studies compared CHM against HT as an active comparison (Azizi 2011; Deng 2011; Gong 2008; Jing 2002; Li 2009; Liang 2003; Qu 2009; Wu 2013; Zhou 2007); one study compared CHM plus placebo against HT plus placebo (Kwee 2007).
Primary outcomes
4.1 Vasomotor symptoms
No data were available for these primary outcomes: frequency of daily hot flushes; frequency of daily night sweats; severity of daily hot flushes; severity of daily night sweats; overall scores of daily hot flushes; overall scores of daily night sweats measured in a diary.
4.1.1 Vasomotor symptoms measured by the MENQOL (monthly)
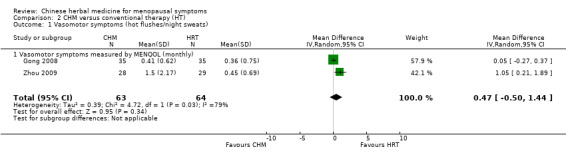
Data from two studies (Gong 2008; Zhou 2009) which measured monthly vasomotor symptoms by MENQoL were suitable for meta‐analysis. However, pooling their data showed no evidence of a difference between the groups in the monthly overall vasomotor symptom scores (MD 0.47 points; 95% CI ‐0.50 to 1.44; 2 RCTs, 127 women). Heterogeneity was presented as Chi² = 4.72, df = 1 (P = 0.03); I² = 79% ,which means the heterogeneity across two included studies was moderately high (Analysis 2.1; Figure 5). This evidence was rated as very low quality: see Table 2.
2.1. Analysis.
Comparison 2 CHM versus conventional therapy (HT), Outcome 1 Vasomotor symptoms (hot flushes/night sweats).
5.
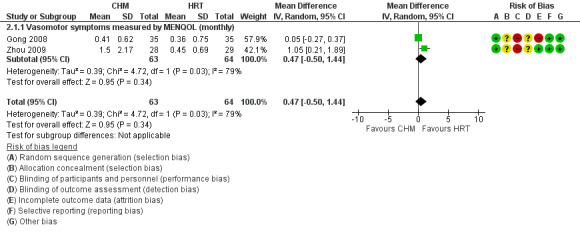
Forest plot of comparison: 2 CHM versus Conventional Therapy (HT), outcome: 2.1 Vasomotor symptoms (hot flushes/night sweats).
We planned a sensitivity analysis based on study quality but did not perform this as both studies in this analysis were at high risk of bias in at least one identified domain.
Secondary outcomes
4.2 Menopausal symptoms measured monthly
Five studies assessed the monthly menopausal symptoms by using different scoring systems. Three studies used the KI scale (Azizi 2011; Deng 2011; Wu 2013) and two studies used the MENQOL (Li 2009; Zhou 2009). Two studies also assessed menopausal symptoms based on individual aspects including the psychosocial component, sexual and physical functions by the MENQOL (Gong 2008; Zhou 2009), however this was not considered in analysis to avoid double counting.
The data from these five studies were considered unsuitable for meta‐analysis using the standardised mean difference (SMD), due to high heterogeneity (I² = 86%). When the data for studies using the KI were pooled, heterogeneity remained high (Chi² = 10.79, df = 2 (P = 0.005); I² = 81%) and there was no evidence of a difference between the groups (MD ‐1.24 points; 95% CI ‐3.99 to 1.52; 3 RCTs, 642 women). When the studies using the MENQOL were pooled, heterogeneity was moderate (Chi² = 2.17, df = 1 (P = 0.14); I² = 54%), there was also no evidence of a difference between the groups (MD ‐1.83 points, 95% CI ‐7.00 to 3.34; 2 RCTs, 285 women) (Analysis 2.2).
2.2. Analysis.
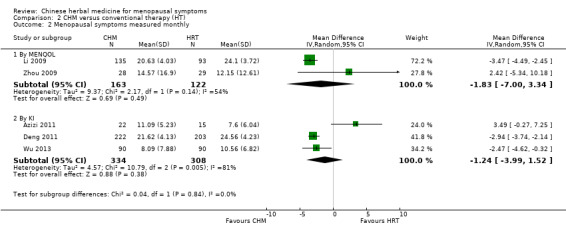
Comparison 2 CHM versus conventional therapy (HT), Outcome 2 Menopausal symptoms measured monthly.
4.3 Improvement in menopausal symptoms
For assessing the dichotomous data from improvement in menopausal symptoms concerning the overall menopausal symptoms in the three Chinese studies (Deng 2011; Li 2009; Wu 2013), a pooled result suggested there was a difference between CHM and HT, in favour of CHM (RR 1.17; 95% CI 1.04 to 1.32; 3 RCTs, 833 women). Heterogeneity across these three studies was acceptable: Chi² = 5.59, df = 2 (P = 0.06), I² = 64% (Analysis 2.3).
2.3. Analysis.
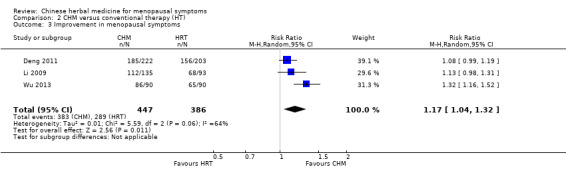
Comparison 2 CHM versus conventional therapy (HT), Outcome 3 Improvement in menopausal symptoms.
4.4 Adverse effects
Six studies (864 women) out of nine studies reported adverse effects. A total of 23 adverse events were reported in the 463 women assigned to CHM and 24 adverse events in the 401 women assigned to HT. Four studies claimed no adverse events, which was not estimable in analysis (Azizi 2011; Deng 2011; Li 2009; Qu 2009). Our findings are compatible with a higher risk of adverse events in either arm, or with no difference between the groups, so no conclusions can be drawn (RR 0.96; 95% CI 0.66 to 1.39; 6 RCTs, 864 women). Heterogeneity was presented as Chi² = 0.22, df = 1 (P = 0.64, I² = 0%), which means that there was no heterogeneity; however the confidence interval was wide, hence, we failed to draw an absolute conclusion on the safety of CHM (Analysis 2.4). Three studies did not mention adverse effects (Jing 2002; Liang 2003; Wu 2013).
2.4. Analysis.
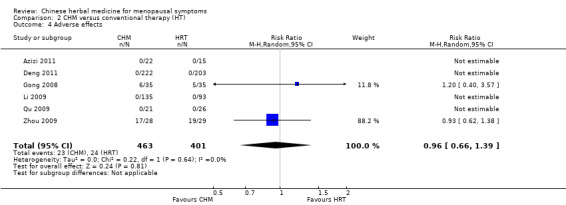
Comparison 2 CHM versus conventional therapy (HT), Outcome 4 Adverse effects.
4.5 Quality of life
Only one study (Zhou 2009) assessed the quality of life by using the MENQOL; the data showed no evidence of a difference between the two groups (MD 2.42 points; 95% CI ‐5.34 to 10.18, 1 RCT, 57 women) (Analysis 2.5).
2.5. Analysis.
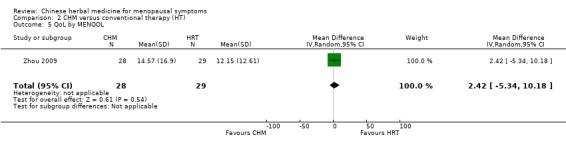
Comparison 2 CHM versus conventional therapy (HT), Outcome 5 QoL by MENQOL.
A comparison of CHM plus placebo versus HT plus placebo was set up in one study (Kwee 2007) and assessed QoL by using the Short Form (36) Health Survey (SF‐36, 0 to 100 scale), it showed no evidence of a difference between the groups (MD ‐0.10 points, 95% CI ‐12.95 to 12.75; 1 RCT, 21 women) (Analysis 2.6).
2.6. Analysis.
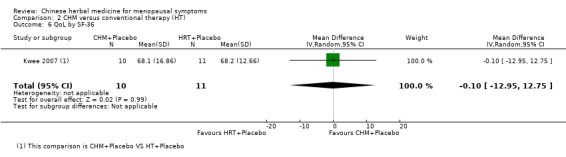
Comparison 2 CHM versus conventional therapy (HT), Outcome 6 QoL by SF‐36.
4.5 Satisfaction of treatment
No study reported this outcome.
5. Comparison of CHM versus conventional therapy (fluoxetine & estazolam)
This compares drugs other than HT, and was reported in the two included studies (Zhang 2009; Zhang 2012). These two studies compared CHM against either fluoxetine (Zhang 2009) or estazolam (Zhang 2012).
Primary outcomes
5.1 Vasomotor symptoms
Data not available.
Secondary outcomes
5.2 Menopausal symptoms
Data not available.
5.3 Adverse effects
Two studies were suitable for pooling (Zhang 2009; Zhang 2012), however the heterogeneity across these studies was still moderately high (Chi² = 2.56, df = 1 (P = 0.11); I² = 61%). There was no evidence of a difference in adverse effects between CHM and conventional medications (RR 0.20; 95% CI 0.03 to 1.17; 2 RCTs, 139 women) (Analysis 3.1).
3.1. Analysis.
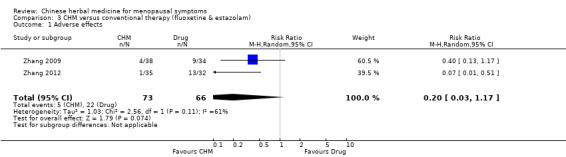
Comparison 3 CHM versus conventional therapy (fluoxetine & estazolam), Outcome 1 Adverse effects.
5.4 Quality of life
Data not available.
5.5 Satisfaction with treatment
Data not available.
6. Comparison of CHM versus another CHM (different formulations)
Two studies (Guo 2009; Xue 2011) that assessed different CHM formulations were included and analysed. One study (Guo 2009) investigated whether a self‐designed experimental formula called Shen Qi Wu Wei Zi decoction was more effective than a control formula, which was either Zuo Gui Yin or You Gui Yin. Both are classical formulations, depending on a TCM diagnosis labelled as Yin‐deficiency pattern or Yang‐deficiency pattern.
The other study (Xue 2011) assessed Geng Mei Ning, a self‐designed formulation, against an over‐the‐counter product, Geng Nian Ning.
Primary outcomes
6.1 Vasomotor symptoms
Data not available.
Secondary outcomes
6.2 Improvement in menopausal symptoms
Two studies (Guo 2009; Xue 2011) reported the data in dichotomous style assessing improvement in menopausal symptoms; in addition, one study (Xue 2011) assessed the improvement in menopausal symptoms in relation to TCM diagnostic pattern scores.
Pooling would be inappropriate for head‐to‐head comparisons using different herbal formulations (Chi² = 38.99, df = 1 (P <0.00001); I² = 97%) (Analysis 4.1).
4.1. Analysis.
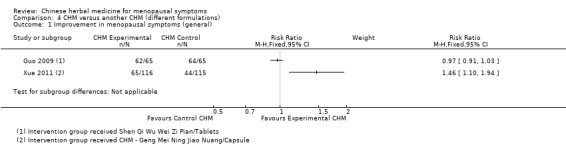
Comparison 4 CHM versus another CHM (different formulations), Outcome 1 Improvement in menopausal symptoms (general).
Individually, one study (Guo 2009) did not demonstrate any evidence of a difference in overall success rate between the two different CHM formulations (RR 0.97; 95% CI 0.91 to 1.03; 1 RCT, 130 women). One of the two studies (Xue 2011), reported the experimented CHM, Geng Mei Ning, was superior to the control CHM, Geng Nian Ning (RR 1.46; 95% CI 1.10 to 1.94; 1 RCT, 231 women) (Analysis 4.1). Xue and colleagues (Xue 2011) also used another assessment tool, TCM diagnostic pattern score to assess changes in menopausal symptoms. It showed evidence of a difference between comparisons with different CHM formulations in favour of the experimental formula, Geng Mei Ning (RR 1.52; 95% CI 1.16 to 2.00; 1 RCT, 231 women) (Analysis 4.2).
4.2. Analysis.
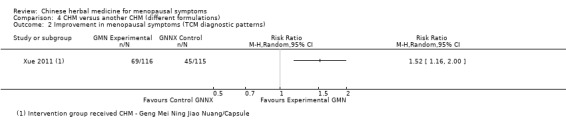
Comparison 4 CHM versus another CHM (different formulations), Outcome 2 Improvement in menopausal symptoms (TCM diagnostic patterns).
Formula compositions in detail are provided in the Characteristics of included studies tables.
6.3 Adverse effects
Only one study (Xue 2011) mentioned there were no adverse events observed in either comparison group.
6.4 Quality of life
Data not available.
6.5 Satisfaction of treatment
Data not available.
7. Comparison of CHM versus acupuncture
No data available.
Subgroup analysis
We did not perform subgroup analyses because there were not enough studies to estimate effects in subgroups in any comparison.
Funnel plots
Due to the small number of studies in any comparison, we did not perform funnel plots.
Discussion
Summary of main results
Data were assessed and findings were reported in line with the rigorous scientific research ideologies and consideration of the fundamental philosophies employed in traditional Chinese medicine (TCM).
Summary of findings
This systematic review of Chinese herbal medicine (CHM) for menopausal symptoms was based on 22 RCTs. There were 2902 perimenopausal and postmenopausal women from different ethnic backgrounds with 90% from a Chinese background. Diagnosis was based on assessment of menopausal scores across the 22 included studies, while nine of the studies also utilised an additional Chinese medicine diagnostic tool.
Except for two studies that evaluated one Chinese herbal formula, 20 trials studied different formulations which consisted of different ingredients with a total of 91 experimented herbs. Amongst them there were 11 of the most commonly used herbs which are very consistent with the clinical literature resources and contemporary clinical practice. Placebo, hormone therapy (HT) and other types of conventional drugs as well as another herbal formula were used as comparisons, however, the majority of the studies used placebo (8/22 studies) and HT (10/22 studies) as a control, this includes one study that used both placebo and HT as controls.
It was noted that when a style of herbal intervention was considered in these included studies, neither a single herb, nor a complete tailored approach (which is the most standard TCM practice) was used. The majority of studies used a standard formula throughout the trial, which is a reflection of the reconciliation between the rigorous scientific methodology and the fundamental TCM philosophies as an effort of integration in contemporary Chinese medicine research.
The most popular length of intervention was 12 weeks, with a few trials having one to four weeks lead‐in period and four to 12 weeks follow‐up. The majority of the interventions used CHM extract in the form of granules.
Although the quality of study design was relatively good as far as many similar CHM clinical trials other than in the area of hot flushes were concerned, there were still serious flaws in the study designs. A large proportion of the included studies (16/22) did not report how allocation concealment was carried out; less than 50% of studies (10/22) were double‐blind trials which influenced partially the primary outcome with less impact on some of secondary outcomes such as changes in the levels of hormones and lipids. Placebo seemed to be used appropriately in terms of its identical appearance and taste to CHM. Intention‐to‐treat (ITT) was not implemented appropriately, only 13/22 studies considered missing and incomplete data. Nevertheless, reporting bias was relatively low, since the majority of studies reported expected outcomes. Many studies did not report full compositions, or full dosages of the investigated formulations, or both. No other potential bias was detected across the included studies.
Several different common menopausal symptoms scores were used. This included numerical results from an individual or a combination of menopausal symptoms and dichotomous data from a combination of menopausal symptoms. A few studies used the same outcome measure such as the Kupperman Index (KI), Menopause‐Specific Quality of Life (MENQOL), Greene Climacteric Scale (GCS) and Menopause Rating Scale (MRS). However for statistical analysis, data were entered and analysed separately, in order to best address the heterogeneity caused by the diversity in terms of assessment tools.
Findings of the CHM effects on menopausal symptoms were summarised in the following aspects.
Vasomotor symptoms: Meta‐analysis of the pooled data found CHM was no better than placebo for vasomotor symptoms measured by frequency and severity of daily hot flushes, and overall scores of vasomotor symptoms by a specific questionnaire. The evidence was rated from low to moderate grade.
With HT as control intervention, pooled continuous data did not show any difference in the overall vasomotor symptoms between the CHM and HT with no data available on the other defined aspects of vasomotor symptoms. The evidence was rated as very low grade.
The rest of defined comparisons reported no data on the primary outcome, i.e. vasomotor symptoms.
Menopausal symptoms: Meta‐analysis of the pooled monthly menopausal symptom scores showed no difference between CHM and HT in continuous data; however the pooled monthly menopausal symptoms scores in dichotomous data set suggested a difference between CHM and HT, in favour of CHM. No pooled data were available from other comparisons on menopausal symptoms.
Adverse effects: The majority of the studies (17 out of 22) evaluated adverse effects; overall, the Chinese herbal formulae were well‐tolerated based on the clinical adverse effects events and the relevant laboratory examinations (haematological and biochemical). Most adverse effects reported were mild to moderate including diarrhoea, tenderness of the breasts, gastric discomfort, and the unfavourable taste of the CHM. The adverse effects symptoms were resolved once the CHM was terminated. Meta‐analysis of the pooled adverse effects in the dichotomous data set showed no difference between CHM and placebo or in the comparisons between CHM and HT or drugs. In summary, it is reasonable to conclude that CHM did not present any higher risk of adverse effects compared with HT, placebo and some pharmaceutical drugs.
Quality of life: Only two studies evaluated this outcome measure by using either the MENQOL or SF‐36. There was no difference between CHM plus placebo and placebo groups.
Satisfaction of treatment: no study assessed this outcome.
Other outcomes: There was a tendency that studies conducted in China were more likely to assess the hormone levels including serum FSH, LH, E2 and/or progesterone for exploring any possible mechanisms of effectiveness. However these were not outcomes of interest to this review and we have not reported them.
Overall completeness and applicability of evidence
The objective of this review was to evaluate the effectiveness and safety of CHM in perimenopausal and postmenopausal women using the same research methods across the included studies. The participants were perimenopausal and postmenopausal women; various formulae with 11 of the most commonly used herbs investigated with a standard approach. The range of intervention periods varied widely from four weeks to 106 weeks, with the most common duration being 12 weeks. The most commonly used form of herbs is herbal extract as granules for practical purposes. Outcome measures assessed included frequency and intensity of daily hot flushes and night sweats, monthly menopausal symptoms scores, adverse effects, quality of life which were consistent with current practice in menopause research.
However, incomplete reports on formula compositions and dosages, paucity of data on the number of women experiencing adverse events, substantial heterogeneity for primary and secondary outcome measures, flaws in design leading to high risk of bias in allocation, blinding, incomplete outcome data and selective reporting issues made the results inconclusive. Thus, the completeness and applicability of the evidence is limited.
Furthermore, the formulations and herbs varied; there were 21 formulae with 91 herbal ingredients. This limits the applicability of findings in general practice of Chinese herbal medicine, since there are many more formulae and herbs that were not tested in the included studies but are commonly used in day‐to‐day practice. Assessment of an individual's constitution which is often interpreted as Chinese medicine diagnostic patterns also influences applicability of the evidence in this review. For the consumer, it is very important to seek professional advice from a qualified Chinese medicine practitioner.
In addition, the majority of participants were of Chinese background, so results should be interpreted with caution when applied to other ethnic groups.
Quality of the evidence
The quality of the evidence for CHM for menopausal symptoms was affected by inadequate reporting of study methods. Figure 2 and Figure 3 indicate the methodological quality of the trials included in this review based on the review authors' judgements. Many studies did not report full compositions or full dosages of the investigated formulations. Therefore, the quality of the evidence was impacted potentially by the presence of selection bias, performance bias, attrition bias and reporting bias. The quality of the evidence was also influenced by the unexplained high level of heterogeneity between studies, types of herbs experimented and the paucity of data on the number of women experiencing adverse events. Using GRADE criteria, the quality of the body of evidence for comparison of CHM versus placebo was rated from moderate to very low for effectiveness. See Table 1. The quality of the evidence for the comparison of CHM versus HT was rated very low for effectiveness outcomes. See Table 2. The quality of the evidence for adverse effects from above comparisons was graded very low.
Potential biases in the review process
It is notable that there were a few limitations to this review. Although the search strategy was comprehensive, it is possible that some unpublished reports or studies published in languages other than English and Chinese could have been unintentionally missed. Therefore language and publication bias cannot be excluded entirely. Furthermore, the heterogeneity of measures used and study materials tested in the included studies made it difficult to compare across the included studies. The expanded defined outcomes in the review stage may introduce bias in reporting the results.
Agreements and disagreements with other studies or reviews
The main findings of this review do not completely echo the results from previous reviews (Peng 2014; Taylor‐Swanson 2014; Xie 2005; Xu 2012). Whilst this review is likely the most comprehensive systematic review with meta‐analysis, it found little evidence that CHM was any more or less efficacious for the management of menopausal symptoms compared to placebo or HT.
Authors' conclusions
Implications for practice.
Based on the findings, this review was unable to draw firm conclusions about the effectiveness and safety of CHM for menopausal symptoms due to inadequate quality of the research evidence.
Implications for research.
In view of the heterogeneity across the included studies, inadequate reporting of study methods, blinding of relevant personnel, and the wide range of outcome measurements, there is a need for conducting further research on CHM for menopausal symptoms. Recommendations for further research include the improvement of the quality of study designs including allocation concealment, randomisation and participants' withdrawals. Consideration of measuring relevant symptoms as the whole‐person when designing trials of CHM should also be given. The fundamental tradition philosophies should be also considered when rigorous scientific research design is implemented in order to reflect the true clinical practice as well as long‐term positive empirical clinical response.
Herb extracts are more practical for a CHM trial than herbs in a raw form. Furthermore, a standardised formulation should only be tested in consideration of relevant Chinese medicine diagnostic pattern(s) for its validity. In addition, greater consistency in outcome measures is warranted.
It would be interesting to look into the potential mechanisms of CHM on menopausal symptoms, given that many studies reported the relevant data. As a safety guidance, it is important to understand if CHM may influence the hormone profiles in a similar manner as HT does, or whether it is different from the HT pathways. Further studies on CHM pharmacological mechanisms are warranted as this will provide comfort on the use of CHM as an alternative in comparison with the known adverse effects of HT.
What's new
| Date | Event | Description |
|---|---|---|
| 9 May 2016 | Amended | Adding source of support: National Center for Complementary and Alternative Medicine Grant Number R24 AT001293 |
Acknowledgements
The review authors would like to acknowledge Helen Nagels, Marian Showell and the team of the Gynaecology and Fertility Group for their guidance and assistance with the preparation of the review, and to Jane Clarke and Michelle Proctor for their involvement in the development of the protocol. We also acknowledge Yunjiao Zhang, a Masters student of Beijing University of Chinese Medicine, for assistance with the data entry from the studies published in Chinese.
This work was partially funded by Grant Number R24 AT001293 from the National Center for Complementary and Alternative Medicine (NCCAM). The contents of this systematic review are solely the responsibility of the authors and do not necessarily represent the official views of the NCCAM or the National Institutes of Health.
Appendices
Appendix 1. Search Strings
MDSG search strings 03.03.10
Keywords CONTAINS "menopausal"or "menopausal symptoms" or "*Menopause" or"perimenopausal"or"climacteric "or"vasomotor"or"hot flashes"or"hot flushes"or"night sweats"or"night time awakenings" or "vaginal atrophy"or"vaginal dryness"or"sleep disturbances " or Title CONTAINS "menopausal"or "menopausal symptoms" or "*Menopause"or"perimenopausal"or"climacteric "or"vasomotor"or"hot flashes"or"hot flushes"or"night sweats"or"night time awakenings" or "vaginal atrophy"or"vaginal dryness"or"sleep disturbances "
AND
Keywords CONTAINS "Chinese"or "Chinese drugs" or "Chinese herbal medicine" or "Chinese herbal preparations" or "Chinese herbal remedy" or "Chinese traditional medicine" or "traditional" or "traditional Chinese medicine" or "traditional medicine" or "herbal remedy" or "herbal preparations" or "TCM" or Title CONTAINS "Chinese"or "Chinese drugs" or "Chinese herbal medicine" or "Chinese herbal preparations" or "Chinese herbal remedy" or "Chinese traditional medicine" or "traditional" or "traditional Chinese medicine" or "traditional medicine" or "herbal remedy" or "herbal preparations"
Appendix 2. CENTRAL
1 exp menopause/ or exp perimenopause/ or exp postmenopause/ (5295) 2 perimenopaus$.tw. (358) 3 postmenopaus$.tw. (8298) 4 menopaus$.tw. (3938) 5 exp Climacteric/ (5514) 6 exp Hot Flashes/ (457) 7 (hot flush$ or hot flash$).tw. (1014) 8 climacteric.tw. (625) 9 (vagina$ adj3 atroph$).tw. (111) 10 (vagina$ adj3 dry$).tw. (136) 11 night sweat$.tw. (107) 12 sleep hyperhydrosis.tw. (1) 13 vasomotor.tw. (899) 14 or/1‐13 (12732) 15 exp Drugs, Chinese Herbal/ (2110) 16 exp medicine, east asian traditional/ or exp medicine, chinese traditional/ or exp medicine, kampo/ or exp medicine, korean traditional/ or exp medicine, tibetan traditional/ or exp medicine, mongolian traditional/ or exp shamanism/ (709) 17 Chinese herb$.tw. (711) 18 chinese medicine$.tw. (1499) 19 (TCM or CHM).tw. (755) 20 herbal remed$.tw. (79) 21 traditional chinese.tw. (1496) 22 herb$ medic$.tw. (631) 23 or/15‐22 (4862) 24 14 and 23 (107) 25 limit 24 to yr="2013 ‐Current" (4)
Appendix 3. MEDLINE
1 exp menopause/ or exp perimenopause/ or exp postmenopause/ (45349) 2 perimenopaus$.tw. (3160) 3 postmenopaus$.tw. (41190) 4 menopaus$.tw. (35550) 5 exp Climacteric/ (48778) 6 exp Hot Flashes/ (2271) 7 (hot flush$ or hot flash$).tw. (3523) 8 climacteric.tw. (3758) 9 (vagina$ adj3 atroph$).tw. (437) 10 (vagina$ adj3 dry$).tw. (718) 11 night sweat$.tw. (1474) 12 sleep hyperhydrosis.tw. (10) 13 vasomotor.tw. (10513) 14 or/1‐13 (94257) 15 exp Drugs, Chinese Herbal/ (27932) 16 exp medicine, east asian traditional/ or exp medicine, chinese traditional/ or exp medicine, kampo/ or exp medicine, korean traditional/ or exp medicine, tibetan traditional/ or exp medicine, mongolian traditional/ or exp shamanism/ (14208) 17 Chinese herb$.tw. (5912) 18 chinese medicine$.tw. (11455) 19 (TCM or CHM).tw. (5590) 20 herbal remed$.tw. (1735) 21 traditional chinese.tw. (11941) 22 herb$ medic$.tw. (8166) 23 or/15‐22 (53195) 24 randomized controlled trial.pt. (370712) 25 controlled clinical trial.pt. (88159) 26 randomized.ab. (290599) 27 placebo.tw. (157119) 28 clinical trials as topic.sh. (169353) 29 randomly.ab. (210726) 30 trial.ti. (124919) 31 (crossover or cross‐over or cross over).tw. (60271) 32 or/24‐31 (916037) 33 (animals not (humans and animals)).sh. (3832165) 34 32 not 33 (844035) 35 14 and 23 and 34 (141) 36 (2013$ or 2014$).ed. (1223461) 37 (2013$ or 2014$).dp. (1269887) 38 36 or 37 (1703263) 39 35 and 38 (22)
Appendix 4. EMBASE
1 exp menopausal syndrome/ or exp "menopause and climacterium"/ or menopause related disorder/ (87566) 2 postmenopaus$.tw. (51909) 3 perimenopaus$.tw. (4048) 4 menopaus$.tw. (47536) 5 (hot flush$ or hot flash$).tw. (4725) 6 climacteric.tw. (4194) 7 (vagina$ adj3 atroph$).tw. (680) 8 (vagina$ adj3 dry$).tw. (1094) 9 night sweat$.tw. (2591) 10 sleep hyperhydrosis.tw. (18) 11 vasomotor.tw. (11751) 12 exp herbal medicine/ or exp Chinese herb/ or exp Chinese medicine/ or exp Chinese drug/ (42962) 13 exp traditional medicine/ (57094) 14 Chinese herb$.tw. (7684) 15 (chinese adj2 medicine$).tw. (20385) 16 (TCM or CHM).tw. (7541) 17 herbal remed$.tw. (2478) 18 traditional chinese.tw. (16578) 19 herb$ medic$.tw. (11831) 20 or/12‐19 (81691) 21 Clinical Trial/ (829834) 22 Randomized Controlled Trial/ (339246) 23 exp randomization/ (61637) 24 Single Blind Procedure/ (18063) 25 Double Blind Procedure/ (112516) 26 Crossover Procedure/ (38388) 27 Placebo/ (236843) 28 Randomi?ed controlled trial$.tw. (96261) 29 Rct.tw. (13470) 30 random allocation.tw. (1289) 31 randomly allocated.tw. (19842) 32 allocated randomly.tw. (1898) 33 (allocated adj2 random).tw. (707) 34 Single blind$.tw. (13987) 35 Double blind$.tw. (138429) 36 ((treble or triple) adj blind$).tw. (353) 37 placebo$.tw. (194048) 38 prospective study/ (245966) 39 or/21‐38 (1341843) 40 case study/ (25274) 41 case report.tw. (254843) 42 abstract report/ or letter/ (884458) 43 or/40‐42 (1159072) 44 39 not 43 (1304562) 45 or/1‐11 (128369) 46 20 and 44 and 45 (332) 47 (2013$ or 2014$).em. (2049870) 48 (2013$ or 2014$).dp. (238178) 49 47 or 48 (2050589) 50 46 and 49 (35)
Appendix 5. AMED
1 exp climacteric/ or exp menopause/ or exp postmenopause/ (527) 2 perimenopaus$.tw. (36) 3 postmenopaus$.tw. (398) 4 menopaus$.tw. (683) 5 (hot flush$ or hot flash$).tw. (79) 6 climacteric.tw. (50) 7 (vagina$ adj3 atroph$).tw. (3) 8 (vagina$ adj3 dry$).tw. (11) 9 night sweat$.tw. (19) 10 sleep hyperhydrosis.tw. (0) 11 vasomotor.tw. (87) 12 or/1‐11 (1005) 13 exp Traditional medicine chinese/ or exp Drugs chinese herbal/ (6308) 14 Chinese herb$.tw. (2074) 15 chinese medicine$.tw. (1618) 16 (TCM or CHM).tw. (798) 17 herbal remed$.tw. (289) 18 traditional chinese.tw. (1417) 19 herb$ medic$.tw. (1228) 20 or/13‐19 (8128) 21 12 and 20 (98) 22 limit 21 to yr="2013 ‐Current" (3)
Appendix 6. PSYCINFO
1 exp menopause/ (2878) 2 postmenopause.tw. (115) 3 perimenopaus$.tw. (489) 4 menopaus$.tw. (3676) 5 Climacteric.tw. (410) 6 Hot Flash$.tw. (294) 7 hot flush$.tw. (171) 8 (vagina$ adj3 atroph$).tw. (35) 9 (vagina$ adj3 dry$).tw. (115) 10 night sweat$.tw. (115) 11 sleep hyperhydrosis.tw. (4) 12 vasomotor.tw. (1159) 13 or/1‐12 (5726) 14 exp "Medicinal Herbs and Plants"/ or exp Alternative Medicine/ (7267) 15 Chinese herb$.tw. (156) 16 chinese medicine$.tw. (485) 17 (TCM or CHM).tw. (267) 18 herbal remed$.tw. (185) 19 traditional chinese.tw. (867) 20 herb$ medic$.tw. (437) 21 or/14‐20 (8242) 22 13 and 21 (83) 23 limit 22 to yr="2013 ‐Current" (4)
Appendix 7. CINAHL
| # | Query | Results |
| S37 | S35 AND S36 | 34 |
| S36 | EM 2014* or EM 2015* | 416,204 |
| S35 | S20 AND S34 | 323 |
| S34 | S21 OR S22 or S23 or S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 | 947,067 |
| S33 | TX allocat* random* | 4,203 |
| S32 | (MH "Quantitative Studies") | 13,178 |
| S31 | (MH "Placebos") | 9,129 |
| S30 | TX placebo* | 33,418 |
| S29 | TX random* allocat* | 4,203 |
| S28 | (MH "Random Assignment") | 38,874 |
| S27 | TX randomi* control* trial* | 84,708 |
| S26 | TX ( (singl* n1 blind*) or (singl* n1 mask*) ) or TX ( (doubl* n1 blind*) or (doubl* n1 mask*) ) or TX ( (tripl* n1 blind*) or (tripl* n1 mask*) ) or TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) | 757,569 |
| S25 | TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) | 111 |
| S24 | TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) | 0 |
| S23 | TX clinic* n1 trial* | 170,178 |
| S22 | PT Clinical trial | 77,532 |
| S21 | (MH "Clinical Trials+") | 185,045 |
| S20 | S12 AND S19 | 801 |
| S19 | S13 OR S14 OR S15 OR S16 OR S17 OR S18 | 32,165 |
| S18 | TX herb* medic* | 12,475 |
| S17 | TX herbal remed* | 785 |
| S16 | TX (TCM or CHM) | 1,702 |
| S15 | TX chinese medicine* | 12,045 |
| S14 | TX Chinese herb* | 4,431 |
| S13 | (MM "Medicine, Chinese Traditional+") OR (MM "Drugs, Chinese Herbal") OR (MM "Medicine, Herbal+") OR (MM "Medicine, Oriental Traditional+") | 19,925 |
| S12 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 | 23,407 |
| S11 | TX vasomotor | 1,089 |
| S10 | TX night* sweat* | 351 |
| S9 | TX (vagina* N3 dry*) | 229 |
| S8 | TX (vagina* N3 atroph*) | 133 |
| S7 | TX (hot flush* or hot flash*) | 2,294 |
| S6 | (MH "Climacteric+") | 15,293 |
| S5 | TX menopaus* | 11,724 |
| S4 | TX postmenopaus* | 11,774 |
| S3 | TX perimenopaus* | 3,138 |
| S2 | (MM "Perimenopause") OR (MM "Perimenopausal Symptoms+") OR (MM "Hot Flashes") | 2,569 |
| S1 | (MM "Menopause+") OR (MM "Postmenopause") | 7,094 |
Appendix 8. CNKI
1. (title=climacteric or title =menopause or title =perimenopause ) or (key word=climacteric or key word =menopause or key word =perimenopause ) or (subject=climacteric or subject =menopause or subject =perimenopause ) and text word=random (exact match) (2608)
2. title= climacteric or title=menopause or title=perimenopause and title=Chinese herbal medicine or title=herbal medicine or title=Chinese medicine and title= Chinese herbal medicine or title=herbal medicine or title=Chinese medicine and title=Chinese herbal medicine or title=herbal medicine or title=Chinese medicine ) or ( key word= climacteric or key word =menopause or key word =perimenopause or key word = Chinese herbal medicine or key word=herbal medicine or key word=Chinese medicine and key word= Chinese herbal medicine or key word= Chinese herbal medicine or key word=herbal medicine or key word=Chinese medicine or key word= Chinese herbal medicine or key word=herbal medicine or key word=Chinese medicine) or (subject=climacteric or subject =menopause or subject =perimenopause or subject=Chinese herbal medicine or subject=herbal medicine or subject =Chinese medicine or subject=Chinese herbal medicine or subject=herbal medicine or subject =Chinese medicine or subject=Chinese herbal medicine or subject=herbal medicine or subject =Chinese medicine ) and text word=random (exact match) (407)
Data and analyses
Comparison 1. CHM versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Vasomotor symptoms (hot flushes/night sweats) | 5 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Frequency of hot flushes in a diary (daily) | 2 | 199 | Mean Difference (IV, Random, 95% CI) | 0.00 [‐0.88, 0.89] |
| 1.2 Severity of hot flushes in a diary (daily) | 1 | 108 | Mean Difference (IV, Random, 95% CI) | ‐0.70 [‐1.00, ‐0.40] |
| 1.3 Overall scores of hot flushes in a diary (daily) | 3 | 263 | Mean Difference (IV, Random, 95% CI) | ‐0.81 [‐2.08, 0.45] |
| 1.4 Overall scores of hot flushes in a diary (monthly) | 1 | 84 | Mean Difference (IV, Random, 95% CI) | ‐2.80 [‐8.93, 3.33] |
| 1.5 Overall scores of night sweats in a diary (daily) | 1 | 64 | Mean Difference (IV, Random, 95% CI) | 0.07 [‐0.19, 0.33] |
| 1.6 Overall scores of night sweats in a diary (monthly) | 1 | 84 | Mean Difference (IV, Random, 95% CI) | 1.30 [‐1.76, 4.36] |
| 1.7 Vasomotor symptoms measured by KI (monthly) | 1 | 69 | Mean Difference (IV, Random, 95% CI) | ‐4.79 [‐5.52, ‐4.06] |
| 1.8 Vasomotor symptoms measured by MENQOL (monthly) | 3 | 256 | Mean Difference (IV, Random, 95% CI) | ‐0.42 [‐1.52, 0.68] |
| 2 Menopausal symptoms measured monthly | 4 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 By MENQOL | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 By KI | 2 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 By HFRDI | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Improvement in menopausal symptoms | 1 | 110 | Risk Ratio (M‐H, Random, 95% CI) | 1.46 [1.13, 1.89] |
| 4 Adverse effects | 7 | 705 | Risk Ratio (M‐H, Random, 95% CI) | 1.51 [0.69, 3.33] |
| 5 QoL by SF‐36 | 1 | 20 | Mean Difference (IV, Random, 95% CI) | 10.60 [‐3.66, 24.86] |
Comparison 2. CHM versus conventional therapy (HT).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Vasomotor symptoms (hot flushes/night sweats) | 2 | 127 | Mean Difference (IV, Random, 95% CI) | 0.47 [‐0.50, 1.44] |
| 1.1 Vasomotor symptoms measured by MENQOL (monthly) | 2 | 127 | Mean Difference (IV, Random, 95% CI) | 0.47 [‐0.50, 1.44] |
| 2 Menopausal symptoms measured monthly | 5 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 By MENQOL | 2 | 285 | Mean Difference (IV, Random, 95% CI) | ‐1.83 [‐7.00, 3.34] |
| 2.2 By KI | 3 | 642 | Mean Difference (IV, Random, 95% CI) | ‐1.24 [‐3.99, 1.52] |
| 3 Improvement in menopausal symptoms | 3 | 833 | Risk Ratio (M‐H, Random, 95% CI) | 1.17 [1.04, 1.32] |
| 4 Adverse effects | 6 | 864 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.66, 1.39] |
| 5 QoL by MENQOL | 1 | 57 | Mean Difference (IV, Random, 95% CI) | 2.42 [‐5.34, 10.18] |
| 6 QoL by SF‐36 | 1 | 21 | Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐12.95, 12.75] |
Comparison 3. CHM versus conventional therapy (fluoxetine & estazolam).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Adverse effects | 2 | 139 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.03, 1.17] |
Comparison 4. CHM versus another CHM (different formulations).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Improvement in menopausal symptoms (general) | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2 Improvement in menopausal symptoms (TCM diagnostic patterns) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Azizi 2011.
| Methods | Trial design: Single‐blinded RCT Year of trial: June 2008 to July 2009 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced at baseline with statistical analysis Sample size calculation: yes (60 as proposed) Intention‐to‐treat: not performed Drop‐off: 8.3% in the CHM group; 16.7% in the CHM plus acupuncture group; 37.5 % in the HT group Compliance: compliance rates were not reported, but author reported that "they attempted to measure the participants' compliance by calling them regularly" Duration of study including follow‐up: 2 months (8 weeks) with no follow‐up period |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: a gynaecology clinic at Dong Zhi Men Hospital in Beijing Setting: 97 women recruited with 72 randomised into three groups [24 (CHM) vs 24 (CHM + acupuncture) vs 24 (HT)] Included: women with perimenopausal or postmenopausal status aged from 40 to 59 years with > 3 of the 11 Kupperman Index symptoms; perimenopausal women with irregular cycles or with a rise of follicle stimulating hormone (FSH) concentration >10 IU/L: showing a pattern of kidney and liver deficiency accompanied by Liver Yang hyperactivity, women who have taken but ceased taking systemic HT or selective serotonin reuptake inhibitors (SSRI) for 8 weeks or ceased topical estradiol (E2) preparations for 4 weeks. Excluded: currently taking systemic HT, SSRI or topical estradiol (E2) preparations; organic diseases of reproductive system; currently under treatment or suffering from breast cancer, serious cardiac, renal, metabolic, endocrine or hepatic disease Chinese medicine diagnosis: performed with all participants diagnosed as pattern, deficiency of Kidney and Liver Yin accompanied with Liver Yang hyperactivity by one designated CM doctor |
|
| Interventions | Experimental groups: Group A, CHM only; Group B, CHM plus acupuncture Group A (CHM only)
Group B (CHM plus acupuncture)
2. Control group (HT):
Note: Only Group A (CHM) in the experimental group was assessed against the control group (HT) |
|
| Outcomes | Primary outcome was measured as change in reporting of:
Secondary outcomes were measured as change in reporting of:
Outcome measured: at baseline and the end of 8 weeks of intervention |
|
| Notes | Langauage: English Country/region of study: Beijing, China Type of publication: Journal article Funding source: Iran's Ministry of Health and Medical Education; Beijing University of Chinese Medicine |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation chart was used |
| Allocation concealment (selection bias) | High risk | Assignments were placed on a table visible to be assigned |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as it was impossible in the methodology of the trial |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessor was blinded and results analyst was blinded to study groups |
| Incomplete outcome data (attrition bias) All outcomes | High risk | ITT was not performed. |
| Selective reporting (reporting bias) | Low risk | Protocol not available, but most expected outcomes were reported |
| Other bias | Low risk | No other potential bias detected |
Deng 2011.
| Methods | Trial design: RCT Year of trial: June 2006 to December 2009 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics in both groups was balanced at baseline with statistical analysis Sample size calculation: not reported Intention‐to‐treat: nor performed Drop‐off: 26.98% in both groups (22.11% in the experimental group; 31.65% in the control group) Compliance: not reported Duration of study including follow‐up: 6 months (24 weeks) of intervention with no follow‐up period |
|
| Participants | Ethnics: Chinese Number of study centres: 2 Source: out patients from General Hospital of Guang Zhou Military Region and Yue Xiu District Women's and Childen Clinic, Guang Zhou Setting: 582 women randomised into two groups [285 (CHM ‐ Bu Shen Zhuang Gu Chong Ji/Granules) vs 297 (HT ‐ Premarin and Medroxyprogesterone acetate)] Included: 582 women aged 46 to 60 years with amenorrhoea for more than one year with symptoms of hot flushes, sweating, palpitations, depression, insomnia, irritability, fluctuations of blood pressure, increased systolic blood pressure, abnormal skin sensation and so on; alleviated levels of FSH, LH and E2 declined; secondary sexual characteristics may be degenerated in different degrees; reproductive organs may be atrophied in different degrees; Chinese medicine pattern diagnosis of the deficiency of the spleen and kidney in accordance with the defined criteria with the main symptom of hot flushes and sweats, accompanied by three of the following signs, including dizziness and tinnitus, fatigue and lack of strength, chest tightness and shortness of breath, loss of appetite and libido, lower back pain, pale tongue and little coating, deep and weak pulse Excluded: women who had history of breast fibroids, breast hyperplasia, breast cancer, cervical cancer and other malignancies; diabetes and other endocrine diseases; taken steroids, contraceptives, lipid‐lowering drugs or anticoagulants; severe hypertension and venous thrombosis; coronary artery disease by EGC; angiography for suspicious coronary Chinese medicine diagnosis: performed with one defined pattern (deficiency of the spleen and kidney) |
|
| Interventions | Experimental group (CHM‐ Bu Shen Zhuang Gu Chong Ji/Granules):
Control group [HT ‐ Premain (conjugated oestrogens tablets) and Medroxyprogesterone acetate]
|
|
| Outcomes | Primary outcome None Secondary outcome measured as changes in:
Outcome endpoint: at baseline and the end of 6 months (24 weeks) of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Guan Dong, China Type of publication: Journal article Funding source: State Administration of Traditional Chinese Medicine Foundation Guang Dong Province (No. 2060124, No. 102151); Science and Technology Project Guang Dong Province (No. 2008B040200019) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | Not in detail |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as one group took granules while the other group took tablets. Personnel blinding not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 26.98% drop‐off in both groups; ITT was not reported |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | No other potential bias detected |
Gong 2008.
| Methods | Trial design: RCT Year of trial: June 2005 to April 2006 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics in both groups were balanced with statistical analysis Sample size calculation: not reported Intention‐to‐treat: not performed Drop‐off: 34.61% in both groups (32.7% in experimental group; 36.53% in comparison group) Compliance: not reported Duration of study including follow‐up: one year (52 weeks) with assessment every three months with no follow‐up period. |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: out patients of Affliated Gynecology and Obstetrics Hospital, Fu Dan University Setting: 104 women randomised into two groups [52 (CHM ‐ Kun Tai Wan/Capsules) vs 52 (HT ‐ Premarin) or with Medroxyprogesterone acetate)] Included: women aged 42 to 57 years with no symptoms contradictory to use of HT; cession of menstruation naturally for more than three months but less than three years or induced by hysterectomy; symptoms of hot flushes and night sweats and other associated conditions; E2< 30 pg/mL and FSH > 40 IU/mL Excluded: not reported Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM ‐ Kun Tai Wan/capsule )
Comparison group: [HT ‐ Premain (conjugated oestrogens tablets) and plus Medroxyprogesterone acetate if uterus remained]
|
|
| Outcomes | Primary outcome was measured as vasomotor symptoms change in reporting of:
Secondary outcome measured as changes in:
Outcome endpoint: baseline and the end of each three months of intervention for a period of one year. |
|
| Notes | Langauage: Chinese Country/region of study: Shang Hai, China Type of publication: Journal article Funding source: National 15th Scientific and Technological Grant (No. 2004BA720A08) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | Not in detail |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as one group took oral liquid plus drops while the other group only took drops. Personnel blinding was not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Drop‐off were not considered in analysis |
| Selective reporting (reporting bias) | Low risk | All expected aspects were reported |
| Other bias | Low risk | No other potential bias detected |
Guo 2009.
| Methods | Trial design: RCT Year of trial: April to December 2008 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics were balanced in both groups with statistical analysis Sample size calculation: not reported Intention‐to‐treat: unclear, there seemed to be no drop‐off Drop‐off: 0% in both groups Compliance: not reported Duration of study including follow‐up: 4 weeks with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 2 Source: out patients from two defined hospitals Setting: 130 women randomised into two groups [65 (CHM ‐ Shen Qi Wu Wei Zi Pian/Tablets) vs 65 (CHM ‐ tailored formula)] Included: women aged 41 to 60 years FSH >10u/L; signed an informed consent form Excluded: women with hypertension; coronary heart disease, hyperthyroid functions, depression, anxiety, brain or mental disorders |
|
| Interventions | Experimental group (CHM ‐ Shen Qi Wu Wei Zi Pian/tablets)
Control group (CHM ‐ two tailored formulae)
|
|
| Outcomes | Primary outcome
Secondary outcome measured as changes in:
Outcome endpoint: was not reported |
|
| Notes | Langauage: Chinese Country/region of study: China Type of publication: Journal article Funding source: not applicable |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | No in detail |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment. Personnel blinding was not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There seemed to be no drop‐off |
| Selective reporting (reporting bias) | High risk | No protocol no pre‐specified aspects |
| Other bias | Low risk | No other potential bias detected |
Haines 2008.
| Methods | Trial design: RCT, double‐blind, placebo‐controlled study Year of trial: unclear Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced at baseline with statistical analysis Sample size calculation: reported to be 41 in each group Intention‐to‐treat: not reported Drop‐off: 9% in the experimental group, 22% in the control group Compliance: not reported Duration of study including follow‐up: 6 months (24 weeks) with no follow‐up period |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: a menopause clinic in a public hospital Setting: 84 of 100 randomised women [45 (CHM) vs 39 (placebo)] Included: women with symptoms of menopausal of any age, confirmed with a follicle stimulating hormone concentration (FSH) >18 IU/L, luteinizing hormone concentration (LH) >12.6 IU/L and estradiol (E2) <361 pmol/L, and being amenorrhoeic for at least 12 months. Excluded: had used any form of any Chinese medicine or any hormone therapy with 8 weeks of recruitment of if they had any serious underling medical disorders or undiagnosed vaginal bleeding. Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM ‐ Dang Gui Bu Xue Tang/decoction)
Control group (Placebo)
|
|
| Outcomes | Primary outcome measured as change in reporting of:
Secondary outcome measured the changes in reporting of:
Outcome endpoint: baseline (week1, day 0), week 12 and week 24 |
|
| Notes | Langauage: English Country/region of study: Hong Kong Type of publication: Journal article Funding source: Area of Excellence Grant of the University Grants Committe in Hong Kong |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A computer‐generated randomisation code list in blocks of 10 was in use. |
| Allocation concealment (selection bias) | Low risk | No staff having contact with the participants were aware of the treatment allocation and the code was not broken for any participants during the study, however details of the method were not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | As above. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Although it was reported that staff having contact with the participants were not aware of the treatment allocation, it was not stated if staff processing data were blinded to the code. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 22% drop‐off in the control group, ITT was not implemented. |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but it is clear that the published reports included all expected outcomes, including those that were pre‐specified. |
| Other bias | Low risk | No other potential bias detected |
Jing 2002.
| Methods | Trial design: RCT Year of trial: February 2000 to March 2001 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics were balanced in both groups with statistical analysis Sample size calculation: not reported Intention‐to‐treat: not reported Drop‐off: not reported but appeared not to have drop‐off Compliance: not reported Duration of study including follow‐up: 3 months (12 weeks) with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: outpatient department of Obstetrics and Gynecology Hospital, Fu Dan University in Shang Hai Setting: 56 women randomised into two groups [32 (CHM ‐ Geng Nian Qin Jiao Nang/capsule vs 24 (HT ‐ Premarin and Medroxyprogesterone acetate Tablets)] Included: 56 women aged 44 to 54 years with memory deficiency as a main complaint with no specific treatment in the past two months, no history of exposure to radiation or ovariectomy Excluded: not reported Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM ‐ Geng Nian Qin Jiao Nang/capsule)
Control group (HT ‐ Premarin and Medroxyprogesterone acetate tablets)
|
|
| Outcomes | Primary outcome
Secondary outcome measured as changes in:
Outcome endpoint: at baseline and the end of 12 weeks of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Shanghai, China Type of publication: Journal article Funding source: Shanghai Key Disciplines in the Leading Field of Integrative Gynecology (No.96001) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as one group took capsules while the other group took tablets Personnel blinding not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There seemed to be no drop‐off |
| Selective reporting (reporting bias) | Low risk | Pre‐specified aspects were reported |
| Other bias | Low risk | No other potential bias detected |
Kwee 2007.
| Methods | Trial design: RCT, double‐blind, double‐dummy, placebo‐controlled study Year of trial: February to June 2002 and June to October 2004 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced at baseline for demographic and physical health except for poorer mental health in placebo group Sample size calculation: reported Intention‐to‐treat: performed Drop‐off: 10% in the Chinese herbal experimental group, 0% in the HT or control group Compliance: not reported Duration of study including follow‐up: 16 weeks (12 weeks intervention plus 4 weeks follow‐up) |
|
| Participants | Ethnics: Dutch Number of study centres: 1 Source: recruitment of women living in two Dutch cities via newspaper advertisement in 2002 and again in 2004 Setting: 31 women randomised into 3 groups [10 (CHM + placebo) vs 11 (HT + placebo) vs 10 (Placebo)] Included: women aged 45 to 65 years with > 20 hot flushes or night sweats per week, FSH > 30 IU/L, at least in perimenopausal stage with irregular cycles and climacteric symptoms, no other complaints except those of menopause, and ability to understand the context of the trial. Excluded: taking hormones or medications which could affect the vasomotor symptoms, serious diseases such as cancer, autoimmune disorder, thrombosis and thrombophlebitis, BP >160/90 mmHg, endocrine diseases, liver scores > 1.5 of normal value, obesity with body weight > 30% normal values, hormonal intake between first consultation and commencement of trial, refusal to take hormone medication Promelle%, lactating and suffering from porphyria. Chinese medicine diagnosis: performed, Kidney‐yin‐deficiency was the main CM diagnostic pattern with additional patterns such as Kidney‐yang‐deficiency, hyperactivity of Liver‐yang resulting from Liver‐yin‐deficiency, Heart‐blood‐emptiness, weakness of Spleen and Stomach and Phlegm stagnation. The criteria for patten of diagnosis were reported |
|
| Interventions | Experimental group (CHM + placebo):
Control groups with two arms (Group B HT + placebo and Group C placebo): Group B (HT + placebo)
Group C (Placebo)
|
|
| Outcomes | Primary outcome was measured as the changes in the reporting of vasomotor symptoms (the flush reduction percentage compared to the maximum number encountered). Seconday outcomes were measured as the changes in reporting of:
Outcomes measured: at baseline and end of 12 weeks of intervention. |
|
| Notes | Langauage: English Country/region of study: The Netherlands Type of publication: Journal Funding source The Dutch Phytotherapy Association and Dong Xi Foundation |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by coin flip |
| Allocation concealment (selection bias) | Unclear risk | Randomisation carried out by an independent third party with no detail as how allocation concealment was conducted |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Both participants and doctors were blinded to treatment assignment |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It was not clear if outcome assessment was done by personnel who were blinded to the study. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | One CHM participant's data were excluded due to having strong corticosteroids medications for the treatment of asthma during the trial, but unrelated to the trial medications. ITT did not seem to be carried out. |
| Selective reporting (reporting bias) | High risk | The study report failed to include results for a key outcome that would be expected to have been reported for such a study. |
| Other bias | Low risk | No other potential bias detected |
Li 2009.
| Methods | Trial design: RCT Year of trial: March 2002 to March 2006 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics balanced with statistical analysis Sample size calculation: not reported Intention‐to‐treat: no performed Drop‐off: 39.5% in both groups (28% in the experimental group; 50% in the control group) Compliance: not reported Duration of study including follow‐up: 2 years (104 weeks) with assessment every three months but no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: out patients from General Hospital of Guang Zhou Military Region and Yue Xiu District Women's and Childen Clinic, Guang Zhou Setting: 327 women randomised into two groups [188 (Bu Shen Zhuang Gu Chong Ji/Granules) vs 189 (HT ‐ Premarin and Medroxyprogesterone acetate)] Included: aged 45 to 58 years with irregular menstruation or amenorrhoea, hot flushes, sweating, palpitations, depression, insomnia, irritability, fluctuations of blood pressure, increased systolic blood pressure (SBP), abnormal skin sensation and so on; alleviated levels of FSH, LH and decreased E2 levels; secondary sexual characteristics may be degenerated in different degrees; reproductive organs may be atrophied in different degrees; Chinese medicine pattern diagnosis of the deficiency of the Spleen and Kidney with Stagnation of Blood in accordance with the defined criteria with the main symptom of hot flushes and sweats, accompanying with three of the following signs, including dizziness and tinnitus, fatigue and lack of strength, chest tightness and shortness of breath, loss of appetite and libido, lower back pain, pale tongue and little coating, deep and weak pulse. Excluded: women who had history of breast fibroids, breast hyperplasia, breast cancer, cervical cancer and other malignancies; diabetes and other endocrine diseases; taken steroids, contraceptives, lipid‐lowering drugs or anticoagulants; severe hypertension and venous thrombosis; coronary artery disease by EGC; angiography for suspicious coronary Chinese medicine diagnosis: performed with one defined pattern (deficiency of the Spleen and Kidney with Stagnation of Blood) |
|
| Interventions | Experimental group (CHM‐ Bu Shen Zhuang Gu Chong Ji/Granules)
Control group [HT ‐ Premain (conjugated oestrogens tablets) and Medroxyprogesterone acetate]
|
|
| Outcomes | Primary outcome None Secondary outcome measured as changes in:
Outcome endpoint: baseline and the end of the first and second year of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Guang Zhou, China Type of publication: Journal article Funding source: State Administration of Traditional Chinese Medicine Foundation Guang Dong Province (No. 2060124, No102151) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | No in detail |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as one group took oral liquid plus drops while the other group only took drops. Personnel blinding not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Drop‐off was not considered in analysis |
| Selective reporting (reporting bias) | Low risk | All expected outcomes have been reported |
| Other bias | Low risk | No other potential bias detected |
Liang 2003.
| Methods | Trial design: RCT Year of trial: 1999 to 2000 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics were balanced in both groups with statistical analysis Sample size calculation: not reported Intention‐to‐treat: not performed Drop‐off: not reported Compliance: not reported Duration of study including follow‐up: three months (12 weeks) with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 or 2 Source: unclear Setting: 73 women randomised into two groups [46 (CHM ‐ Dan Di Pian/tablet) vs 27 (HT ‐ Wei Ni An)] Included: women aged 40 to 65 years with FSH more than 40 IU/L and BMI less than 30; no abnormality detected in the breast and gynaecological examinations, the liver and kidney function tests, no history of diabetes, malignancy, taking lipid‐lowering drugs, dyslipidaemia, hypertension and severe vein thrombosis Excluded: not reported (it seems to be mixed in report with the inclusion criteria) Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM ‐ Dan Di Pian/tablet)
Control group (HT ‐ Nylestriol containing quinestrol 2.5 mg/tablet)
|
|
| Outcomes | Primary outcome None Secondary outcome measured as changes in:
Outcome endpoint: at baseline and the end of 12 weeks of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Jiang Xi, China Type of publication: Journal article Funding source: Key Research Project of Jiang Xi Province Science and Technology Committee (No. 379370021) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Drawing |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants did not seem to be blinded, no report on personnel neither |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There seemed to be no drop‐off |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | No other potential bias detected |
Lou 2009.
| Methods | Trial design: RCT double‐blind placebo‐controlled Year of trial: June 2006 to May 2008 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced at baseline for demographic characteristics in both groups Sample size calculation: not reported Intention‐to‐treat: yes Drop‐off: 13.75% in the experimental group, 10% in the control group Compliance: not reported Duration of study including follow‐up: 8 weeks with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: study carried out at the Shao Yi Fu Hospital, Zhe Jiang University; recruitment details not reported. Setting: 110 women randomised into two groups [80 (CHM) vs 30 (placebo)] Included: women 45‐60 years old; experiencing menopausal symptoms including hot flushes and night sweats in addition to irregular menstruation. May also experience other symptoms such as irritability, palpitation, insomnia, poor memory, lower back pain, disturbed emotion and so on; and E2 decreased significantly, FSH and LH increased significantly. Excluded: women who had hypertension, mental illness, cardiovascular diseases, endocrine diseases, haematopoietic system diseases, hysterectomy, and double oophorectomy. Chinese medicine diagnosis: not performed. |
|
| Interventions | Experimental group (CHM)
Control group (Placebo)
|
|
| Outcomes | Primary outcome measured the change in reporting of clinical symptom score Secondary outcomes were changes in:
Outcome endpoint: baseline and the end of 8 weeks of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Zhe Jiang, China Type of publication: Journal article Funding source: Zhe Jiang Province TCM Science and Technology Project (491030‐W50703) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | Not in detail |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants, doctors and research staff were blinded to group assignments |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Statisiticians were blinded, although it was not clear if person for data entry was blinded as well |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 12.73% drop‐off in both groups, ITT was implemented |
| Selective reporting (reporting bias) | Low risk | the published reports include all expected outcome were reported |
| Other bias | Low risk | No other potential bias detected |
Plotnikoff 2011.
| Methods | Trial design: RCT, double‐blind, placebo‐controlled study Year of trial: unclear Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced at baseline with statistical analysis Sample size calculation: Yes Intention‐to‐treat: Yes Drop‐off: 22.8% in high dose and 17.7% in low dose experimental groups, 1.7% in the control group Compliance: compliance checks carried out using weekly pill count, rate of compliance was not reported Duration of study including follow‐up: 12 weeks with one week placebo lead‐in period with no follow‐up period |
|
| Participants | Ethnics: American Number of study centres: 1 Source: recruitment from Minneapolis, St Paul metropolitan area Setting: 178 women randomised into three groups [57 (CHM 7.5 g/d) vs 62 (CHM 12.5 g/d) vs 59 (placebo)] Included: women aged 45 to 58 years, with history of amenorrhoea for 12 consecutive months, or hysterectomy without oophorectomy and with a follicle stimulating hormone concentration (FSH) > 40 mIU/m/L, and estradiol (E2) < 20 pg/mL, or two months post hysterectomy plus oophorectomy. Participants must also suffer from vasomotor symptoms with a Mayo hot flush score > 28 per week, willing to take herbal formula, not on any hormonal therapy for prior 8 weeks, smoker < 10 cigarettes per day, BMI < 36, Beck Depression Inventry of < 11 and not on antidepressant medications Excluded: history of breast or uterine cancer. Sufferers of other cancers with < 5 years cancer clearance Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental groups (CHM)
Control group:
|
|
| Outcomes | Primary outcomes were measured as the change in reporting of:
Secondary outcomes were measured via blood tests
Outcome measured: at baseline, one, two and three months after enrolment |
|
| Notes | Langauage: English Country/region of study: Minnesota, USA Type of publication: Journal Funding source Tsumura & Co and National Institutes of Health grant |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation in blocks using pseudo‐random number |
| Allocation concealment (selection bias) | Low risk | Research pharmacy prepared containers for administration to study participants |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants, all investigators and research staff were blinded to group assignment |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Invesigators and assessors were blinded to treatment assignment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Missing data were considered |
| Selective reporting (reporting bias) | Low risk | Protocol followed and outcomes have been reported |
| Other bias | Low risk | No other potential bias detected |
Qu 2009.
| Methods | Trial design: open RCT Year of trial: September 2004 to April 2008 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced at baseline for demographic characteristics in both groups Sample size calculation: not reported Intention‐to‐treat: not applied Drop‐off: 0% in both groups Compliance: not reported Duration of study including follow‐up: 12 weeks with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: study carried out at the Women's Hospital, Zhe Jiang University; recruitment details not reported. Setting: 47 women randomised into 2 groups [21 (CHM) vs 26 (HT)] Included: women aged 45 to 60 years, randomised into with > 6 months of amenorrhoea; serum estradiol < 20 pg/mL; FSH > 40 mIU/L; at least one month of low mood; total score of > 20 in the 24‐item HAMD; absence of organic reproductive system diseases following gynaecological examination and blood tests. No history of depression and willingness to complete the study. Excluded: taking hormones or medications within previous 3 months; medical conditions where oestrogen therapy is contraindicated; structural CNS diseases; cognitive impairment; treatment for depression in previous 3 months; alcohol or drug abuse or drug dependence during the previous 6 months; serious medical problems with high risk of death within a year; schizophrenia; bipolar disorder, or early‐onset dysthymic disorder; surgical menopause, pathological conditions; chemotherapy; or behaviours such as extreme exercise or anorexia nervosa and somatic or neurological illnesses impairing psychiatric evaluation. Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM)
Control group (HT)
|
|
| Outcomes | Primary outcome was measured as the change in reporting of: not applicable Seconday outcome were measured as the change in reporting of:
Outcomes measured: at baseline and the end of intervention at 12 weeks |
|
| Notes | Langauage: English Country/region of study: Hang Zhou, China Type of publication: Journal Funding source: National Natural Science Foundation of China (No. 30800390), China Postdoctoral Science Foundation (No. 20070421188), Outstanding Young Medicall Scientist Foundation of Zhe Jiang Province (No. 2008QN022) and Zhe Jiang TCM Foundation (No. 2008YB010) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation using a randomisation chart |
| Allocation concealment (selection bias) | Unclear risk | Randomisation method was not clear in report |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | participants were not blinded to treatment as one group took herbal liquid while the other group took tablets. However, gynaecologist and psychologist and researcher for assigning randomisation were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No report of blinding of outcome assessors but outcome data was analysed by independent university statistician |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ITT was not required because of zero drop‐off |
| Selective reporting (reporting bias) | Low risk | Not present |
| Other bias | Low risk | No other potential bias detected |
Tao 2009.
| Methods | Trial design: RCT Year of trial: September 2006 to January 2008 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: baseline for demographic characteristics in both groups were balanced with statistical analysis Sample size calculation: not reported Intention‐to‐treat: not reported Drop‐off: 2% drop off in both groups Compliance: not reported Duration of study including follow‐up: 8 weeks with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: out patients at Xi Yuan Hopsital in Bei Jing Setting: 87 women randomised into two groups [44 (CHM + Drug) vs 43 (Drug + Placebo)] Included: at stage I to II of primary hypertension diagnosed by the relevant hypertension criteria; menopausal women aged from 40‐60 as diagnosed in Chinese medicine, pattern of deficiency of Yin and hyperactivity of Yang Excluded: secondary hypertension; systolic pressure > 180 mmHg or diastolic pressure > 110 mmHg; with liver, brain, heart and renal diseases; being involved in other clinical trials; could not tolerate or allergic to the study materials Chinese medicine diagnosis: yes |
|
| Interventions | Experimental group (CHM + Drug) CHM information
Drug information
Control group (Drug + Placebo) Drug information ‐ as above Placebo information
|
|
| Outcomes | Primary outcome
Secondary outcome measured as changes in:
Outcome endpoint: at baseline and every 2 weeks throughout the 8 weeks of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Bei Jing China Type of publication: Journal article Funding source: not applicable |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | No details |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants were blinded, no report on if personnel were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | ITT was not performed |
| Selective reporting (reporting bias) | Low risk | Expected aspects were reported |
| Other bias | Low risk | No other potential bias detected |
van der Sluijs 2009.
| Methods | Trial design: RCT double‐blind, placebo‐controlled Year of trial: September 2004 to October 2005 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced baseline characteristics with statistical analysis Sample size calculation: calculated to be 31 participants in each group Intention‐to‐treat: reported and used for data analysis Drop‐off: 13% for herbal group and 21.8% for placebo group Compliance: 84.73% in herbal group, and 89.07% in placebo group. It was checked by monthly counting of remaining tablets on return of bottles and daily entries in the hot flushes diary Duration of study including follow‐up: 28 weeks (consisted of a 4‐week baseline period, a 16‐week intervention period, and a 8‐week follow‐up after cessation of treatment) |
|
| Participants | Ethnics: Australian Number of study centres: 1 Source: Recruitment through newspaper, magazine articles, television and radio interviews, and through referrals from Liverpool Health service and Royal North Shore Hospitals Setting: 93 women randomised into 2 groups [46 (CHM) vs 46 (placebo)] including one no‐recorded measurements Included: women aged 45 to 65 years with > 12 months of amenorrhoea; with average 5 vasomotor symptoms daily regardless of severity (35 per week); FSH >40 mIU/mL; Estradiol < 80 pg/mL; normal FBC, LFT and renal function within past 6 months: BMI < 30 kg/m2 ; no HT or CAM for treatment of menopausal symptoms in previous 2 months Excluded: undiagnosed vaginal bleeding; history of cancer especially breast or oestrogen‐dependent cancers: using corticosteroids or anticoagulants; uncontrolled and/or undiagnosed medical conditions that are likely to impact on study treatment e.g., diabetes, renal or hepatic dysfunction; uncontrolled or untreated hypertension: uncontrolled psychiatric disorders; other conditions that may make the woman unsuitable for or unable to complete the study. Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM)
Placebo group
|
|
| Outcomes | Primary outcome was measured as the change in reporting of:
Seconday outcomes were measured as the change in reporting of:
Outcome measured: at baseline and the end of intervention |
|
| Notes | Langauage: English Country/region of study: Sydney, Australia Type of publication: Journal article Funding source: Global Therapeutics |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation |
| Allocation concealment (selection bias) | Low risk | Independent data manager performed allocation using a computer randomisation |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants and personnel were blinded to treatment allocation which was revealed after completion of the study |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Data analyst was blinded to treatment allocation, unclear if statistician was blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ITT was undertaken |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | No other potential bias detected |
Wu 2013.
| Methods | Trial design: RCT Year of trial: February 2010 to February 2013 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics were balanced statistically in both groups Sample size calculation: not reported Intention‐to‐treat: no need to perform because of zero drop‐off rate Drop‐off: seemed to be no drop‐off Compliance: not reported Duration of study including follow‐up: 2 months (12 weeks) treatment without follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: from clinic in a traditional Chinese medicine hospital in Qin Huangdao, China Setting: 180 women randomised into two groups [90(CHM ‐ herbal paste) vs 90 (Nilestriol tablets)] Included: women aged 40 to 60 years; falling into the menopause diagnostic criteria used in biomedicine, with the following chief complaints such as hot flushes, insomnia, irritability, fatigue and so on; Kupperman score more than 10 points; FSH > 10IU/L; compliance with Chinese medicine syndrome differentiation standard however it is no clear if pattern diagnosis was considered Excluded: women who do not fall into the diagnosis of menopausal syndrome; suffering from coexisting diseases such as hypertension, hyperthyroidism, genital cancer, coronary heart disease and so on; who do not want to comply with the treatment protocol; previously had received hormone or other medication therapy almost 3months prior to participate the study. |
|
| Interventions | Experimental group (CHM ‐ herbal paste)
Control group (HT ‐ Nilestriol tablets)
|
|
| Outcomes | Primary outcome
Secondary outcome measured as changes in:
Outcome endpoint: at baseline and the end of 2 months of intervention |
|
| Notes | Langauage: Chinese Country/region of study: China Type of publication: Journal article Funding source: 'Twleve Five' Key Specialisation Fostering Projects awarded by the State Administration of Traditional Chinese Medicine (National Chinese Medicine Pracitioner Regulation & Development [2012] 2) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | No detail |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as one group took the tablets, the other group only took herbal paste. Personnel blinding was not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There seemed to be no drop‐off |
| Selective reporting (reporting bias) | Low risk | All expected areas were reported |
| Other bias | Low risk | No other potential bias detected |
Xia 2012.
| Methods | Trial design: RCT double‐blind, placebo‐controlled Year of trial: May to September 2010 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced baseline characteristics with statistical analysis Sample size calculation: not reported Intention‐to‐treat: not performed appropriately Drop‐off: 11.1% for herbal group and 13.9% for placebo group Compliance: compliance rate not reported but authors reported that all remaining study materials count was carried out at end of trial Duration of study including follow‐up: 12 weeks with 4 weeks follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: Recruitment through community‐based media, and referrals from the clinic of the second Afiliated Hospital of Tianjin University of Traditional Chinese Medicine Setting: 72 women randomised into 2 groups [36 (CHM) vs 36 (placebo)] Included: perimenopausal women aged 45 to 55 years with irregular cycles or amenorrhoea for 3 to 11 months and > 14 hot flushes per week. Excluded: severe mammary hyperplasia, endometrial hyperplasia, uterine polyps, and abnormal uterine bleeding; surgical menopause; known hypersensitivity to investigational drugs or their ingredients; previous or existing malignant tumour, hyperthyroidism, hypothyroidism, pheochromocytoma, uncontrolled diabetes, obesity where BMI >30 kg/m2 , neurasthenia, psychiatric disorders, migraine headache, fungal or bacterial vaginal infections, cardio‐cerebral vascular diseases, insufficiently controlled hypertension and hypotension, thromboembolic diseases, GIT diseases affecting drug absorption, haematopoietic system diseases, or auto‐immune system diseases; abnormal LFTor abnormal renal function; smoking presently or previously and alcohol abuse; treatment of climacteric complaints using TCM in previous 4 weeks, vaginal percutaneous or oral oestrogen or oestrogen/progesterone drugs in past 8 weeks, taking progesterone implants and a separate injection of oestrogen therapy in the previous 3 months, and taking oestrogen pills or progesterone injections in the previous 6 months. Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM)
Placebo group
|
|
| Outcomes | Primary outcome was measured as the changes in reporting of:
Seconday outcomes were measured as the changes in reporting of:
Outcome measured: at baseline, week 4, week 8 and week 12. However it was mentioned in the Abstract that follow‐up was performed 4 weeks after cessation of intervention without details in the main texts. |
|
| Notes | Language: English Country/region of study: Tian Jin, China Type of publication: Journal article Funding source: National Science & Technology Pillar Program (No.2009ZX09311‐002; 2008ZX09312‐001), International Cooperative Project of the Science and Technology Ministry and Program (No. 2008DFB30070) for Chang Jiang Scholars and Innovative Research Team in Tian Jin |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation |
| Allocation concealment (selection bias) | Low risk | Allocation preparation performed by an independent data manager and study medicine in numbered containers were distributed by blinded research university pharmacist |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Randomisation concealed from participants and investigative personnel |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Statiscial analyst blinded to treatment allocation until after the final report was produced |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Similar attrition and reasons for dropouts in both active and control group, it was reported as 'modified ITT', which is not true ITT. |
| Selective reporting (reporting bias) | Low risk | Protocol unavailable, but report had covered all expected outcomes |
| Other bias | Low risk | No other potential bias detected |
Xue 2011.
| Methods | Trial design: RCT Year of trial: not clear Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics were balanced in both groups with statistical analysis Sample size calculation: not reported Intention‐to‐treat: not performed Drop‐off: 9% in both groups Compliance: not reported Duration of study including follow‐up: 4 weeks of intervention with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 4 Source: out patients from Xi Yuan Hospital, Guang An Men Hospital, Dong Zhi Men Hospital and The First Affliated Hospital of Guan Xi College of Chinese Medicine Setting: 235 women randomised into two groups [118 (CHM ‐ Geng Mei Ning Jiao Nuang/capsule) vs 117 (CHM ‐ Geng Nian Ning Xin Jiao Nuang/capsule)] Included: in accordance with the diagnosis of menopause in Western medicine with ammonirrhoea within five years with FSH > 40; in accordance with Chinese medicine diagnosis as the pattern of deficiency of the Liver‐Yin and Kidney‐Yin, accompanying with hyperactivity of Heart‐fire and Liver‐fire; aged from 45 to 55 years; HT not in use or cession of HT for more than three months, or not in use of cession of relevant Chinese herbal medicine for more than two months; signed consent form Excluded: history of the following conditions including primary hypertension, or primary hypotension or chronic anaemia, ovariectomy, hysterectomy, or other gynaecological organic disorders; aged below 45 or over 55; allergic constitution; combining with cardiovascular diseases, severe liver and kidney diseases and mental disorders; involved in other clinical trials Chinese medicine diagnosis: yes with one pattern, that is the pattern of the deficiency of the Liver‐Yin and Kidney‐Yin, accompanying with hyperactivity of Heart‐fire and Liver‐fire |
|
| Interventions | Experimental group (CHM ‐ Geng Mei Ning Jiao Nuang/Capsule)
2. Comparison group (CHM ‐ Geng Nian Ning Xin Jiao Nuang/Capusle)
|
|
| Outcomes | Primary outcome
Secondary outcome measured as changes in:
Outcome endpoint: at baseline and the end of 4 weeks of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Bei Jing and Guang Xi China Type of publication: Journal article Funding source: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | No details |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Participants might not be blinded to treatment. Personnel blinding was not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | ITT was not undertaken |
| Selective reporting (reporting bias) | Low risk | All expected outcomes have been reported |
| Other bias | Low risk | No other potential bias detected |
Zhang 2009.
| Methods | Trial design: RCT Year of trial: January 2006 to December 2008 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics were balanced in both groups with statistical analysis Sample size calculation: not reported Intention‐to‐treat: unclear but there was no drop off Drop‐off: no drop‐off Compliance: not reported Duration of study including follow‐up: 4 weeks with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 2 Source: out patients from two local clinics in Bei Jing; Setting: 72 women randomised into two groups [38(CHM ‐ Zhao Ren Bu Xue Tang/decoction) vs 34 (Drug ‐ Prozac Fluoxetine Hydrochloride capsules)] Included: menopausal women aged 45 to 56 years depression for two weeks Excluded: had a history of depression, psychotic disorders prior to menopause, coma, loss of speech, dementia, vision impairment, severe heart, liver and kidney diseases, epilepsy and women using anti‐depressants Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM ‐ Zhao Ren Bu Xue Tang/decoction)
Comparison group [Drug ‐ Prozac (Fluoxetine Hydrochloride Capsules)]
|
|
| Outcomes | Primary outcome None Secondary outcome measured as changes in:
Outcome endpoint: at baseline and the end of 4 weeks of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Bei Jing, China Type of publication: Journal article Funding source: not applicable |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as one group took oral liquid while the other group only took tablet. Personnel blinding was not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There seemed to be no drop‐off |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | No other potential bias detected |
Zhang 2012.
| Methods | Trial design: RCT Year of trial: September to December 2011 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics were balanced in both groups with statistical analysis Sample size calculation: not reported Intention‐to‐treat: not reported but there was no drop‐off Drop‐off: no drop‐off Compliance: not reported Duration of study including follow‐up: 4 weeks with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: out patients from Yue Yang Integrative Medicine Hospital, Shang Hai Setting: 67 women randomised into two groups [35(CHM ‐ Wu Wei Shen Ping Tang/decoction) vs 32 (drug ‐ estazolam)] Included: women with insomnia diagnosed according to the China Mental Disorders Classifications and Diagnostic Criteria; menopause symptoms; aged from 45‐55 in addition to irregular menstruation, hot flushes and sweats, other accompanying symptoms including restless, palpitation, stiffness in the chest, headache, poor memory, unstable blood pressure and lower back pain; a pattern of the deficiency of the liver and kidney in accordance with the relevant criteria Excluded: women who had severe insomnia; a history of primary hypertension, or primary hypotension or chronic anaemia; ovariectomy, hysterectomy, or other gynaecological organic disorders; allergic constitution; combining with cardiovascular diseases, severe liver and kidney diseases and mental disorders; bad compliance or incomplete data Chinese medicine diagnosis: yes with one pattern, that is the pattern of the deficiency of the liver and kidney |
|
| Interventions | Experimental group (CHM ‐ Wu Wei Shen Ping Tang/decoction)
Comparison group (drug ‐ estazolam)
|
|
| Outcomes | Primary outcome
Secondary outcome measured as changes in:
Outcome endpoint: at baseline and the end of 4 weeks of intervention |
|
| Notes | Langauage: Chinese Country/region of study: Shang Hai, China Type of publication: Journal article Funding source: Shang Hai Key Projects (S30303) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | Unclear |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as one group took oral liquid while the other group only took tablets. Personnel blinding was not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There seemed to be no drop‐off |
| Selective reporting (reporting bias) | Low risk | All expected aspects were reported |
| Other bias | Low risk | No other potential bias detected |
Zhong 2013.
| Methods | Trial design: RCT Year of trial: April 2009 to January 2011 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: demographic characteristics were balanced statistically in both groups Sample size calculation: reported Intention‐to‐treat: yes Drop‐off: 5.9% in placebo group and 8% in treatment group Compliance: 91% of participants took at least 80% of scheduled doses Duration of study including follow‐up: 2 weeks baseline, 12 weeks treatment with follow‐up 3 months later |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: women answering local newspapers advertisements Setting: 108 women randomised into two groups [54(CHM ‐ Er‐Xian decoction) vs 54 (placebo)] Included: women aged 45 to 55 years; experiencing > 3 months of irregular cycles; or amenorrhoea for > 3 months within previous 12 months; experiencing hot flushes and having a Menopause Rating Scale (MRS) totaling > 28; for at least 3 months prior to study; and willingness to sign off an informed consent form Excluded: women have not used hormonal or Chinese medicines who are taking hormones or medications that could affect vasomotor symptoms; any medications or therapies for management of menopausal symptoms within the last 3 months or during the study; suffering from chronic illnesses such as GIT disease, renal disease, liver disease, diabetes requiring medications and uncontrolled hypertension; suffering from serious disease such as cancer, autoimmune system disease, thrombosis and thrombophlebitis; having diagnosis of major depressive disorder with symptoms of anxiety, insomnia, poor concentration and poor memory; having used alcohol, psychiatric drugs or psychotherapeutic drugs within 3 months of baseline; having used anticoagulant medication within the 3 months before baseline. Chinese medicine diagnosis: not performed, presumed all patterns were both Kidney‐Yin and Kidney‐Yang deficiency |
|
| Interventions | Experimental group (CHM ‐ Er‐Xian decoction)
Control group (Placebo)
|
|
| Outcomes | Primary outcome
Secondary outcome measured as changes in:
Outcome endpoint: at baseline and the end of 12 weeks of intervention |
|
| Notes | Language: English Country/region of study: Hong Kong Type of publication: Journal article Funding source: Liu Hao Tsing Foundation and Hong Kong University Small Project Funding |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation |
| Allocation concealment (selection bias) | Low risk | Randomisation remained concealed until end of study, code kept at separate location by one research assistant |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | All participants and research personnel were blinded to treatment allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessor was also blinded to treatment allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 5.9% drop out in placebo group, and 8% in treatment group. ITT was used for data analysis |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | No other potential bias detected |
Zhou 2007.
| Methods | Trial design: RCT, double‐blind, placebo‐controlled study Year of trial: May 2003 to June 2006 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced at baseline with statistical analysis Sample size calculation: not reported Intention‐to‐treat: no need to perform because of zero drop‐off rate Drop‐off: 0% in the experimental group, 0% in the control group Compliance: It was reported 'compliance in the study for both groups was excellent > 90%', in this case 100% Duration of study including follow‐up: 12 weeks with no follow‐up |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: University affiliated hospital Setting: 69 women randomised into two groups [36 (CHM) vs 33 (placebo)] Included: 69 ovariectomised women age between 38 and 49 years, with at least 2 years history of menopausal symptoms but not on hormonal or cardiovascular medications. Excluded: under medical treatment for metabolic, renal or endocrine disease. Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM):
Control group (Placebo):
|
|
| Outcomes | Primary outcome was measured as the change in reporting of vasomotor symptoms by modified Kupperman Index Scale (KIS) Secondary outcome was measured as changes
Outcome measured: it was only reported clearly that KIS were measured on the one day before the intervention and the end of the intervention. No details are given on other outcome measurements although it is mentioned that two sets of data were collected before and after the intervention. |
|
| Notes | Langauage: English Country/region of study: Republic of China Type of publication: Journal article Funding source: Innovation Research Foundation for Doctor of Philosphy Grant |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A computer‐generated randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | No details of concealment in report |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants were blinded but no details if staff personnel were blinded although the abstract claims it is doubled‐blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessors although implied in the abstract |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No drop‐off |
| Selective reporting (reporting bias) | Low risk | Analysis by independent Universlty statistician |
| Other bias | Low risk | No other potential bias detected |
Zhou 2009.
| Methods | Trial design: RCT Year of trial: September 2005 to October 2006 Judgement of the quality of study: see 'Risk of bias' table Groups comparable at baseline: balanced at baseline for demographic characteristics in both groups Sample size calculation: not reported Intention‐to‐treat: performed Drop‐off: 35.71% in experimental group; 13.80% in comparison group Compliance: compliance rate was not reported, however remaining study materials were counted by designated personnel Duration of study including follow‐up: intervention was one year (52 weeks) with assessment every three months (12 weeks) with no follow‐up. |
|
| Participants | Ethnics: Chinese Number of study centres: 1 Source: out patients from Hua Xi Second Hospital, Si Chuan University Setting: 57 women randomised into two groups [28 (CHM ‐ Kun Tai Wan/pills) vs 29 (HT ‐ Premarin)] Included: women aged 40 to 57 years with no symptoms contradict to use of HT cession of mensuration naturally or induced by hysterectomy for more than three months but less than three years; symptoms of hot flushes and night sweats and other associated conditions; E2< 30pg/mL and FSH > 40 IU/mL; signed off the consent to participate. Excluded: women who had uterine fibroids > 3 cm or identified diabetes, hypertension endometriosis with obvious symptoms; history of thromboembolic disease and thrombophilia; epilepsy, asthma, hyperprolactinaemia; and family history of breast cancer; serious physical diseases or unstable physical statues; substance (alcohol or drug) abuse or dependence during past three months; taken oestrogen preparations or health drugs for menopausal symptoms during the past one month; single‐layer endometrial thickness measured > 0.5 cm with abnormalities in cervical pap smears (except inflammation); unexplained vaginal bleeding after menopause; allergic history to the experimental materials and participated in other clinical trials in the past month. Chinese medicine diagnosis: not performed |
|
| Interventions | Experimental group (CHM)
Control group [HT ‐ Premain (conjugated oestrogens tablets) and/or Medroxyprogesterone acetate]
|
|
| Outcomes | Primary outcome None Secondary outcome measured as changes in:
Outcome endpoint: baseline and the end of each three months of intervention for a period of one year of intervention. |
|
| Notes | Langauage: Chinese Country/region of study: Sichuan, China Type of publication: Journal article Funding source: National 15th Scientific and Technological Grant (No. 2004BA720A08); Leadership Grant in Academic and Technology, Department of Human Resource, Si Chuan Province (No. 06SXS‐06) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer block randomisation |
| Allocation concealment (selection bias) | Unclear risk | No details of concealment in report |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to treatment as one group took capsules while the other group took tablets. Personnel blinding not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details regarding blinding of outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ITT was performed |
| Selective reporting (reporting bias) | Low risk | All pre‐specified aspects were reported |
| Other bias | Low risk | No other potential bias detected |
BMI: body mass index BP: blood pressure CHM: Chinese herbal medicine CAM: complementary and alternative medicine CNS: central nervous system E2: estradiol FBC: full blood count FSH: follicle stimulating hormone GIT: gastrointestinal HAMD: Hamilton Depression Scale HDL‐C: high‐density lipoprotein cholesterol HFRDI: Hot Flash Related Daily Interference Scale HT: hormone therapy ITT: intention‐to‐treat IU: international unit KIS: Kupperman Index Scale LDL‐C: low‐density lipoprotein cholesterol LFT: lung function test LH: luteinizing hormone MENQOL: Menopause‐Specific Quality of Life questionnaire MMSE: Mini Mental State Examination MRS: Menopause Rating Scale MSQL: Menopause Specific Quality of Life QoL: quality of life RCT: randomised controlled trial SBP: systolic blood pressure SSRI: selective serotonin reuptake inhibitors TC: total cholesterol TG: triglycerides TCM: traditional Chinese medicine vs: versus
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Davis 2001 | No data could be analysed, we therefore contacted the corresponding author, but the original data were not available for retrieval. |
| Koike 2004 | Not relevant to the defined outcomes |
| Qian 2010 | Not relevant to the defined outcomes |
| Tian 2008 | Not a true RCT |
| Wang 2013 | This study was related to different doses which did not meet the inclusion criteria |
| Wei 2009 | Not relevant to the defined outcomes |
RCT: randomised controlled trial
Differences between protocol and review
The following changes have been made in the Methods from protocol to review.
Types of Interventions
In the original protocol, it states:
any Chinese herbal medicine versus placebo for menopausal symptoms (this includes comparisons made on one formula with different doses);
any Chinese herbal medicine versus no treatment for menopausal symptoms;
any Chinese herbal medicine versus conventional therapy (e.g. HT) for menopausal symptoms (CHM were compared with HT and other types of medication separately; similar comparisons in variation were also included);
one type of Chinese herbal medicine (e.g. oral administration) versus another type of Chinese herbal medicine (e.g. topical use) for menopausal symptoms (this includes comparisons made on one formula with different doses);
any Chinese herbal medicine versus acupuncture for menopausal symptoms.
When the review was undertaken, there were a number of comparisons in variation noted. For example, CHM + placebo versus placebo which is a variation of the comparison CHM versus placebo; CHM + placebo versus conventional therapy (HT) + placebo is a variation of the comparison CHM versus conventional therapy (HT). In addition, as control, conventional therapy was assessed either by HT or any medication other than HT termed as a drug. All these variations and refinements are updated as:
CHM versus no treatment
-
CHM versus placebo
including CHM + placebo versus placebo
CHM + conventional therapy (drug as short term) versus placebo + conventional therapy (drug)
-
CHM verus conventional therapy (HT)
including CHM + placebo versus conventional therapy (HT) + placebo
CHM versus conventional therapy (drug)
CHM versus another CHM (different formulations)
CHM versus acupuncture
Types of outcome measures:
The primary outcome in the protocol was defined as 'improvement in frequency or intensity of vasomotor symptoms (i.e. hot flushes and night sweats) evaluated subjectively by participants, usually in daily diaries or by any validated objective scoring system such as Kupperman Index'; however it was noted that such a definition failed to provide a wider scope to the research topic, for example, when either hot flushes or night sweats were measured based on overall scores rather than frequency and intensity, and in a few studies, vasomotor symptoms were also measured based on overall scores without distinguishing hot flushes and night sweats. Hence, more relevant outcomes in the review were considered and evaluated accordingly with priority, that is, only KI and MENQOL, which are most commonly used measurements were included.
We also modified the secondary outcomes, that is only overall scores in questionnaires measuring menopausal symptoms were analysed; subsets of questionnaires were not included.
The relevant outcomes of each comparison are reported as below.
The primary outcome was modified as changes of vasomotor symptoms including:
frequency of hot flushes/night sweats;
severity of hot flushes/night sweats;
overall scores of hot flushes/night sweats (i.e. combination of frequency and severity);
overall scores of vasomotor symptoms (i.e. combination of hot flushes and night sweats).
The secondary outcomes are reported accordingly as below:
menopausal symptoms measured by different instruments;
adverse effects;
quality of Life (QoL);
satisfaction of treatment.
Contributions of authors
Xiaoshu Zhu: registered the title, conceptualised the protocol and wrote the review. XZ also reviewed trials, performed data extraction, data interpretation and assessment. Her experience in preparing CSRs in the field of Chinese medicine guided the preparation of this CSR reflecting the scientific ideology and traditional philosophy for the purpose of its clinical and research validities.
Yuk Lan Liew: commented on and assisted with development of protocol and review. YL reviewed trials, contributed to data extraction, data interpretation and performed data assessment. She also jointly wrote the review and prepared the abstract as well as the Plain language summary. Her solid and sound knowledge and experience in both Western medicine and herbal medicine provided the professional guidance required for preparing this comprehensive CSR.
Zhaolan Liu: commented on and assisted with development of the review. ZL also searched Chinese databases and made significant contribution to data assessment as well as data interpretation with her sound statistics background and experience with CSRs. She jointly wrote the review.
Sources of support
Internal sources
Menstrual Disorders and Sub‐fertility Group, New Zealand.
External sources
University of Western Sydney, National Institute of Complementary Medicine, Australia.
Beijing University of Chinese Medicine, Other.
-
National Center for Complementary and Alternative Medicine (NCCAM), USA.
$5000: Grant Number R24 AT001293.
Declarations of interest
None known.
Edited (no change to conclusions)
References
References to studies included in this review
Azizi 2011 {published data only}
- Azizi H, Liu YF, Du L, Wang CH, Bahrami‐Taghanaki H, Esmaily HO, et al. Menopause‐related symptoms: traditional Chinese medicine vs hormone therapy. Alternative Therapies in Health and Medicine Jul/Aug 2011;17(4):48‐53. [PubMed] [Google Scholar]
Deng 2011 {published data only}
- Deng W, Huang H, Zeng D, Li X, Zhang J, Shao Y, et al. Effect of bushen zhuanggu granules upon gonadal hormone and blood fat in climacteric females [补肾壮骨冲剂对更年期综合征患者性激素及血脂的影响]. Journal of Traditional Chinese Medicine 2011;52(3):208‐13. [Google Scholar]
Gong 2008 {published data only}
- Gong L, Zhang S, Ji L. Effect of hormone and Chinese Traditional Medicine treatment on cognition and memory and quality of life in the women at the early stage of menopause [绝经早期激素与中药治疗对认知记忆和生存质量的影响]. Reproduction and Contraception 2008;28(1):26‐31. [Google Scholar]
Guo 2009 {published data only}
- Guo M, Sheng Y. Clinical observation of 65 cases in menopausal syndrome with TCM syndrome differentiation and treatment [中医辨证治疗更年期综合征65例临床观察]. Journal of Traditional Chinese Medicine 2009;50(Supplement):167‐8. [Google Scholar]
Haines 2008 {published data only}
- Haines CJ, Lam PM, Chung TKH, Cheng KF, Leung PC. A randomized, double‐blind, placebo‐controlled study of the effect of a Chinese herbal medicine preparation (Dang Gui Buxue Tang) on menopausal symptoms in Hong Kong Chinese women. Climateric 2008;11(3):244‐51. [DOI] [PubMed] [Google Scholar]
Jing 2002 {published data only}
- Jing S, Wei M. Clinical study on relationship between memory quotient, estrogen and Chinese nourishing kidney herbs in perimenopausal women [围绝经期妇女的记忆商与雌激素及补肾中药之间关系的临床研究]. Chinese Journal of Integrated Traditional and Western Medicine 2002;22(7):494‐5. [PubMed] [Google Scholar]
Kwee 2007 {published data only}
- Kwee SH, Tan HH, Marsman A, Wauters C. The effect of Chinese herbal medicines (CHM) on menopausal symptoms compared to hormone replacement therapy (HRT) and placebo. Maturitas 2007;58(1):83‐90. [DOI] [PubMed] [Google Scholar]
Li 2009 {published data only}
- Li X, Deng W, Zhang J, Zhou L, Huang W. Effect of bushen zhuanggu granule on the gonadal hormone and blood lipid metabolism in climacteric women [补肾壮骨冲剂对围绝经期妇女性激素及血脂代谢的影响]. Chinese Journal of Integrated Traditional and Western Medicine 2009;29(7):599‐602. [PubMed] [Google Scholar]
Liang 2003 {published data only}
- Liang R, Chen M, Xu Xi, Pan Z, Hu X, Zhou S, et al. Effect of dandi tablet on blood lipids and sex hormones in women of postmenopausal stage [丹地片对绝经后女性血脂及性激素的影响]. Chinese Journal of Integrated Traditional and Western Medicine 2003;23(8):593‐5. [PubMed] [Google Scholar]
Lou 2009 {published data only}
- Lou HY, Huang D, Fang SH, Zhao XF, Huang QX, Wang MZ. Clinical study on XianLing GuBao capsule in patients with menopausal syndrome. China Journal of Chinese Malteria Medice 2009,11;34(22):2950‐2. [Google Scholar]
Plotnikoff 2011 {published data only}
- Plotnikoff GA, Watanabe K, Torkelson C, Valleur J, Radosevich DM. The TU‐025 Keishibukuryogan for hot flash management in postmenopausal women: results and lessons for future research. Menopause August 2011;18(8):886‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Qu 2009 {published data only}
- Qu F, Cai X, Gu Y, Zhou J, Zhang R, Burrows E, et al. Chinese medicinal herbs in relieving perimenopausal depression: a randomized, controlled trial. Journal of Alternative and Complementary Medicine 2009;15(1):93‐100. [DOI] [PubMed] [Google Scholar]
Tao 2009 {published data only}
- Tao L, Ma X, Chen K. Clinical study on effect of Qingxuan Tiaoya Recipe in treating menopausal women with hypertension [清眩调压方治疗更年期女性高血压病的临床研究]. Chinese Journal of Integrated Traditional and Western Medicine 2009.8;29(8):680‐4. [PubMed] [Google Scholar]
van der Sluijs 2009 {published data only}
- Sluijs CP, Bensoussan A, Chang S, Baber R. A randomized placebo‐controlled trial on the effectiveness of an herbal formula to alleviate vasomotor symptoms. Menopause 2009;16(2):336‐44. [DOI] [PubMed] [Google Scholar]
Wu 2013 {published data only}
- Wu S, Ma Y, Ou X, Li D. Research and analysis of 180 cases of patients with the climacteric syndrome treated by herbal paste intervention [膏滋干预脾肾阳虚型更年期综合征180例研究分析]. Medical Innovation of China [Zhong Guo Yi Xue Chuang Xing] 2013;10(25):1‐2. [Google Scholar]
Xia 2012 {published data only}
- Xia Y, Zhao Y, Ren M, Zhang J, Wang Y, Chang Y, et al. A randomized double‐blind placebo controlled trial of a Cinese herbal medicine preparation (Jiawei Qing'e Fang) for hot flashes and quality of life in perimenopausal women. Menopause 2012;19(2):234‐44. [DOI] [PubMed] [Google Scholar]
Xue 2011 {published data only}
- Xue S, Zhang Q, Jiang X, Jin Z. Effect of bushen zhuanggu granules upon gonadal hormone and blood fat in climacteric females [更美宁胶囊治疗更年期综合征的多中心临床研究]. Traditional Chinese Drug Research & Clinical Pharmacology 2011;22(1):117‐20. [Google Scholar]
Zhang 2009 {published data only}
- Zhang G, Zhang G, Ai C, Xie Y, Zhao W, Yue C. Clinical observation of 38 cases involutional depression treated by Zaoren Buxue decoction together with fluoxetine [枣仁补血汤联合氟西汀治疗更年期抑郁症38 例临床观察]. Beijing Journal of Traditional Chinese Medicine 2009.11;28(11):873‐4. [Google Scholar]
Zhang 2012 {published data only}
- Zhang W, Liu Q, Zhang Z, Huang T, Cai Z. Randomized control research on theory of Yunqi in differentiating and treating menopausal insomnia of liver‐kidney deficiency pattern [基于运气学说辨治肝肾亏虚型更年期失眠症的随机对照研究]. Shanghai Journal of Traditional Chinese Medicine 2012;46(3):51‐3. [Google Scholar]
Zhong 2013 {published data only}
- Zhong LLD, Tong Y, Tang GWK, Zhang ZJ, Choi WK, Cheng KL, et al. A randomized, double‐blind, controlled trial of a Chinese herbal formula (Er‐Xian decoction) for menopausal symptoms in Hong Kong perimenopausal women. Menopause 2013;20(7):1‐10. [DOI] [PubMed] [Google Scholar]
Zhou 2007 {published data only}
- Zhou J, Qu F, Nan R, Tang D. The effect of Chinese medicinal herbs in relieving menopausal symptoms in ovariectomized Chinese women.. Explore 2007;3(5):478‐84. [DOI] [PubMed] [Google Scholar]
Zhou 2009 {published data only}
- Zhou LL, Xu LZ, Liu HW, Zhang J, Liu Y, Liu XF, et al. The effect of QOL and cost‐utility analysis on sex hormone and Chinese medicine in women with early postmenopausal. Nan Fang Yi Ke Da Xue Xue Bao [Journal of Southern Medical University] 2009;29(11):2181‐6. [PubMed] [Google Scholar]
References to studies excluded from this review
Davis 2001 {published data only}
- Davis SR, Briganti EM, Chen RQ, Dalais FS, Bailey M, Burger H. The effects of Chinese medicinal herbs on postmenopausal vasomotor symptoms of Australian women. Medical Journal of Australia 2001;174(2):68‐71. [DOI] [PubMed] [Google Scholar]
Koike 2004 {published data only}
- Koike K, Ohno S, Takahashi N, Suzuki N, Nozaki N, Murakami K, et al. Efficacy of the herbal medicine Unkei‐to as an adjunctive treatment to hormone replacement therapy for postmenopausal women with depressive symptoms. Clinical Neuropharmacology 2004;27(4):157‐62. [DOI] [PubMed] [Google Scholar]
Qian 2010 {published data only}
- Qian L, Wang B, Niu J, Gao S, Zhao D. Assessment of the clinical effect of Chinese medicine therapy combined with psychological intervention for treatment of patients of perimenopausal syndrome complicated with hyperlipidemia. Chinese Journal of Integrative Medicine April 2010;16(2):124‐30. [DOI] [PubMed] [Google Scholar]
Tian 2008 {published data only}
- Tian H, Zhang CY. The combination use of acupuncture and Chinese medicines for treatment of menopausal syndrome: a clinical report of 63 cases. Journal of Traditional Chinese Medicine 2008;28(1):3‐4. [DOI] [PubMed] [Google Scholar]
Wang 2013 {published data only}
- Wang CC, Cheng KF, Lo WM, Law C, Li L, Leung PC, et al. A randomized, double‐blind, multiple‐dose escalation study of a Chinese herbal medicine preparation (Dang Gui Buxue Tang) for moderate to severe menopausal symptoms and quality of life in postmenopausal women. Menopause 2013;20(2):223‐31. [DOI] [PubMed] [Google Scholar]
Wei 2009 {published data only}
- Wei D, Li Y H, Zhou W Y, Wang Z Q. Observation on therapeutic effect of runmushu oral liquid in treating xerophthalmia in postmenopausal women [润目舒口服液治疗绝经后期妇女干眼症疗效观察]. Chinese Journal of Integrated Traditional and Western Medicine 2009;29(7):646‐9. [PubMed] [Google Scholar]
Additional references
Amato 2002
- Amato P, Christophe S, Mellon P. Estrogenic activity of herbs commonly used as remedies for menopausal symptoms. Menopause 2002;9:145‐50. [DOI] [PubMed] [Google Scholar]
Avis 2001
- Avis NE, Stellato R, Crawford S. Is there a menopausal syndrome? Menopausal status and symptoms across racial/ethnic groups. Social Science and Medicine 2001;52(3):345‐56. [DOI] [PubMed] [Google Scholar]
Bair 2008
- Bair YA, Gold EB, Zhang G, Rasor N, Utts J, Upchurch D, et al. Use of complementary and alternative medicine during the menopause transition: longitudinal results from the Study of Women's Health Across the Nation [Bair YA1, Gold EB, Zhang G, Rasor N, Utts J, Upchurch DM, Chyu L, Greendale GA, Sternfeld B, Adler SR.Author information]. Menopause 2008;15(1):32‐43. [DOI] [PubMed] [Google Scholar]
Biddle 2003
- Biddle RA, Wilkinson JM, Simpson MD. Do Australian women use complementary medicines for reproductive conditions?. Australian Journal of Pharmacy 2003;22(1):52‐6. [Google Scholar]
Boardman 2015
- Boardman HMP, Hartley L, Eisinga A, Main C, Roqué i Figuls M, Bonfill Cosp X, et al. Hormone therapy for preventing cardiovascular disease in post‐menopausal women. Cochrane Database of Systematic Reviews 2015, Issue 3. [DOI: 10.1002/14651858.CD002229.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Carpenter 2001
- Carpenter JS. The Hot Flash Related Daily Interference Scale; a tool for assessing the impact of hot flashes on quality of life following breast cancer. Journal of Pain Symptom Management 2001;22(6):979‐9. [DOI] [PubMed] [Google Scholar]
Castel‐Branco 2005
- Castelo‐Branco C, Palacios S, Mostajo D, Tobar C, Helde S. Menopausal transition in Movima women, a Bolivian Native‐American. Maturitas 2005;51(4):380‐5. [DOI] [PubMed] [Google Scholar]
Chen 2010
- Chen LC, Wang BR, Chen IC, Shao CH. Use of Chinese herbal medicine among menopausal women in Taiwan. International Journal of Gynecology and Obstetrics 2010;109(1):63‐6. [DOI] [PubMed] [Google Scholar]
Chim 2002
- Chim H, Tan BH, Ang CC, Chew EM, Chong YS, Saw SM. The prevalence of menopausal symptoms in a community in Singapore. Maturitas 2002;41(4):275‐82. [DOI] [PubMed] [Google Scholar]
Colditz 2005
- Colditz GA. Estrogen, oestrogen plus progestogen therapy, and risk of breast cancer. Clinical Cancer Research 2005;11(2 Pt 2):909‐17. [PubMed] [Google Scholar]
Deng 1983
- Deng TT, Guo ZQ. Diagnosis in Traditional Chinese Medicine: Textbook for national TCM tertiary education. Shanghai Science and Technology Press: Shanghai, 1983. [Google Scholar]
Dennerstein 2004
- Dennerstein L, Lehert P. Women's sexual functioning, lifestyle, mid‐age, and menopause in 12 European countries. Menopause 2004;11(6 Pt 2):778‐85. [DOI] [PubMed] [Google Scholar]
Dodin 2013
- Dodin S, Blanchet C, Marc I, Ernst E, Wu T, Vaillancourt C, Paquette J, Maunsell E. Acupuncture for menopausal hot flushes. Cochrane Database of Systematic Reviews 2013, Issue 7. [DOI: 10.1002/14651858.CD007410] [DOI] [PMC free article] [PubMed] [Google Scholar]
Geller 2006
- Geller S, Studee L. Contemporary alternatives to plant estrogens for menopause. Maturitas 2006;55(Supp1):3‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gold 2001
- Gold E, Bromberger J, Crawford S. Factors associated with age at natural menopause in a multiethnic sample of midlife women. American Journal of Epidemiology 2001;153(9):865‐74. [DOI] [PubMed] [Google Scholar]
Greendale 1999
- Greendale GA, Lee NP, Arriola ER. The menopause. Lancet 1999;353(9152):571‐80. [DOI] [PubMed] [Google Scholar]
Greene 1976
- Greene JG. A factor analytic study of climacteric symptoms. Journal of Psychosomatic Research 1976;20(5):425‐30. [DOI] [PubMed] [Google Scholar]
Haines 2005
- Haines CJ, Xing SM, Park KH, Holinka CF, Ausmanas MK. Prevalence of menopausal symptoms in different ethnic groups of Asian women and responsiveness to therapy with three doses of conjugated estrogens/medroxyprogesterone acetate: the Pan‐Asia Menopause (PAM) study. Maturitas 2005;52(3‐4):264‐76. [DOI] [PubMed] [Google Scholar]
Hauser 1994
- Hauser GA, Huber IC, Keller PJ, Lauritzen C, Schneider HP. Evaluation of climacteric symptoms (Menopause Rating Scale) [Article in German]. Zentralblatt für Gynäkologie 1994;116(1):16‐23. [PubMed] [Google Scholar]
Heinemann 2003
- Heinemann LAJ, Potthoff P, Schneider HPG. International versions of the Menopause Rating Scale (MRS). Health and Quality of Life Outcomes 2003;1:28. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins J P T, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration: www.cochrane‐handbook.org. 2011.
Hilditch 1996
- Hilditch JR, Lewis J, Peter A, Maris B, Ross A, Franssen E, et al. A menopause‐specific quality of life questionnaire: development and psychometric properties. Maturitas 1996;24(3):161‐75. [DOI] [PubMed] [Google Scholar]
Hunter 1992
- Hunter MS. The women's health questionnaire: a measure of mid‐aged women's perceptions of their emotional and physical health. Psychology & Health 1992;7(1):45‐54. [Google Scholar]
Kronenberg 2002
- Kronenberg F, Fugh‐Berman A. Complementary and alternative medicine for menopausal symptoms: a review of randomized, controlled trials. Annals of Internal Medicine 2002;137:805‐13. [DOI] [PubMed] [Google Scholar]
Kupperman 1959
- Kupperman HS, Wetchler BB, Blatt MH. Contemporary therapy of the menopausal syndrome. JAMA 1959;171:1627‐37. [DOI] [PubMed] [Google Scholar]
Leach 2012
- Leach M J, Moore V. Black cohosh (Cimicifuga spp.) for menopausal symptoms. Cochrane Database of Systematic Reviews 2012, Issue 9. [DOI: 10.1002/14651858.CD007244] [DOI] [PMC free article] [PubMed] [Google Scholar]
Liu 2008
- Liu YF, Xiao CZ, Wang TF, Zhang LH, Ding K J. Analysis of contemporary literature on the characteristics of Chinese herbal medicine in use, clinical manifestations and distribution of clinical patterns of menopausal syndromes. Bei Jing Zhong Yi Yao Da Xue Xue Bao [Journal of Beijing University of Traditional Chinese Medicine] 2008;31(2):125‐30. [Google Scholar]
Luo 1986
- Luo YK. Gynaecology in Traditional Chinese Medicine: Textbooks for National TCM Tertiary Education. Shanghai: Shanghai Science and Technology Press, 1986. [Google Scholar]
Marjoribanks 2012
- Marjoribanks J, Farquhar C, Roberts H, Lethaby A. Long term hormone therapy for perimenopausal and postmenopausal women. Cochrane Database of Systematic Reviews 2012, Issue 7. [DOI: 10.1002/14651858.CD004143] [DOI] [PubMed] [Google Scholar]
McBane 2008
- McBane S. Easing vasomotor symptoms: besides HRT, what works?. JAAPA 2008;21:26‐32. [DOI] [PubMed] [Google Scholar]
McKinlay 2006
- McKinlay SM, Brambilla DJ, Posner JG. The normal menopause transition. American Journal of Human Biology 2006;4(1):37‐46. [DOI] [PubMed] [Google Scholar]
Michelle 2002
- Michelle P, Warren MD. Use of alternative therapies in menopause. Best Practice & Research Clinical Obstetrics and Gynaecology 2002;16(3):411‐48. [DOI] [PubMed] [Google Scholar]
Ministry of Health of PRC 1995
- Ministry of Health of the People's Republic of China. Clinical Standards for Diagnostic Evidence and Treatment Outcome Evaluation. Beijing: People's Health Publishing House, 1995. [Google Scholar]
Nelson 2008
- Nelson H. Menopause. Lancet 2008;371:60‐70. [DOI] [PubMed] [Google Scholar]
Newton 2002
- Newton KM, Buist DSM, Keenan NL, Anderson LA, LaCroix AZ. Use of alternative therapies for menopause symptoms: results of a population‐based sample. Obstetrics and Gynecology 2002;100(1):18‐25. [DOI] [PubMed] [Google Scholar]
NIH 2005
- NIH. NIH State‐of‐the‐Science Conference Statement on Management of Menopause‐Related Symptoms. NIH Consensus State Science Statements 2005;22(1):1‐38. [PubMed] [Google Scholar]
NJUTCM 2006
- Nanjing University of Traditional Chinese Medicine. Chinese Materia Medica Pharmacopoeia. Shanghai Scientific and Technology Press, 2006. [Google Scholar]
Ososki 2003
- Ososki AL, Kennelly EJ. Phytoestrogens: a review of the present state of research. Phytotherapy Research 2003;17(8):845‐69. [DOI] [PubMed] [Google Scholar]
Peng 2014
- Peng W, Sibbritt DW, Hickman L, Kong X, Yang L, Adams J. A critical review of traditional Chinese medicine use amongst women with menopausal symptoms. Climacteric : the journal of the International Menopause Society 2014;17(6):635‐44. [PUBMED: 24678630] [DOI] [PubMed] [Google Scholar]
Persson 2000
- Persson I. Estrogens in the causation of breast, endometrial and ovarian cancers ‐ evidence and hypotheses from epodemiological findings. Journal of Steroid Biochemistry and Molecular Biology 2000;74(5):357‐64. [DOI] [PubMed] [Google Scholar]
Potthoff 2000
- Potthoff P, Heinemann LA, Schneider HP, Rosemeier HP, Hauser GA. The Menopause Rating Scale (MRS II): methodological standardization in the German population [Article in German]. Zentralblatt für Gynäkologie 2000;122(5):280‐6. [PubMed] [Google Scholar]
Punnonen 1980
- Punnonen RH. Oestrogen‐like effect of ginseng. British Medical Journal 1980;281(6248):1110. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rossouw 2002
- Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Writing Group for the Women's Health Initiative Investigators. Risks and benefits of oestrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomised controlled trial. JAMA 2002;288(3):321‐33. [DOI] [PubMed] [Google Scholar]
Scheid 2007
- Scheid V. Traditional Chinese medicine‐what are we investigating? The case of menopause. Complementary Therapies in Medicine 2007;15:54‐68. [DOI] [PMC free article] [PubMed] [Google Scholar]
Singh 2002
- Singh A, Kaur S, Walia I. A historical perspective on menopause and menopausal age. Bulletin of the Indian Institute of History of Medicine (Hyderabad) 2002;32(2):121‐35. [PubMed] [Google Scholar]
Sloan 2001
- Sloan JA, Loprinzi CL, Novotny PJ, Barton DL, Lavasseur BI, Windschitl H. Methodologic lessons learned from hot flash studies. Journal of Clinical Oncology 2001;19(23):4280‐90. [DOI] [PubMed] [Google Scholar]
Störk 2004
- Störk S, Shouw YT, Grobbee D E, Bots ML. Estrogen, inflammation and cardiovascular risk in women: a critical appraisal. Trends in Endocrinology and Metabolism 2004;15(2):66‐72. [DOI] [PubMed] [Google Scholar]
Taylor‐Swanson 2014
- Taylor‐Swanson L, Thomas A, Ismail R, Schnall J G, Cray S L, Mitchell E S, Woods N F. Effects of traditional Chinese medicine on symptoms clusters during the menopausal transition. Climacteric 2015;18(2):142‐56. [DOI] [PubMed] [Google Scholar]
Tindle 2005
- Tindle HA, Davis RB, Phillips RS, Eisenberg DM. Trends in use of complementary and alternative medicine by US adults: 1997‐2002. Alternative Therapies in Health and Medicine 2005;Jan‐Feb;11(1):42‐9. [PubMed] [Google Scholar]
Xie 2005
- Xie Y, Zhu Y, Wu T. Effects and safety of traditional Chinese medicine for treating postmenopausal Osteoporosis: a systematic review. Chinese Journal of Evidence‐Based Medicine 2005;5(1):20. [Google Scholar]
Xu 2012
- Xu LW, Jia M, Salchow R, Kentsch M, Cui XJ, Deng HY, et al. Efficacy and side effects of Chinese herbal medicine for menopausal symptoms: a critical review. Evidence‐Based Complementary and Alternative Medicine 2012; Vol. 2012:Article ID 568106.19 pages. [PUBMED: 23365599] [DOI] [PMC free article] [PubMed]
Xue 2007
- Xue CC, Zhang AL, Lin V, Costa CDA, Story DF. Complementary and alternative medicine use in Australia: a national population‐based survey. Journal of Alternative and Complementary Medicine 2007;13(6):643‐50. [DOI] [PubMed] [Google Scholar]
Zhu 2009
- Zhu XS, Carlton AL, Bensoussan A. Development in and challenge for traditional Chinese medicine in Australia. Journal of Alternative and Complementary Medicine 2009;15(6):685‐8. [DOI] [PubMed] [Google Scholar]