
Fig. 13.
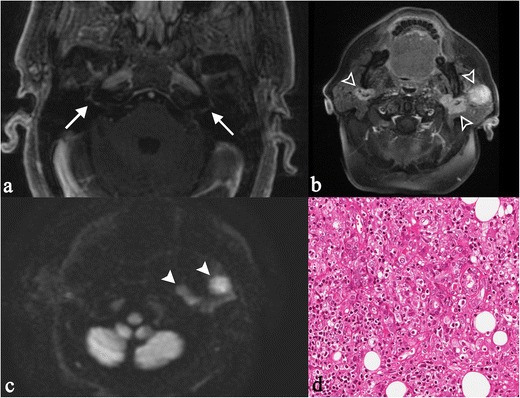
“Heerfordt’s syndrome” in a 60-year-old woman. Clinically, the patient complained of sudden appearance of blurred vision, headache, and mouth deviation to the left after fever. MRI shows bilateral enhancement of facial nerve (white arrows on Fig. 13a), recognizable on T1-weighted image obtained after gadolinium administration. She showed a complete facial palsy and a bilateral enlargement of the cheeks. Physical examination revealed an unpainful enlargement of the left parotid gland, left facial nerve and left abducent nerve palsy. Nodular lesions were found in the parotid glands (same patient in Fig. 8), with evident contrast enhancement on T1-weighted acquisitions after contrast enhancement (Fig. 13b, empty white arrowhead) and on DWI sequences (Fig. 13c, white arrowheads). Chest CT scan and fibrobronchoscopy with bronchoalveolar lavage were suggestive of sarcoidosis. The biopsy of the left parotid gland depicted dense, non-caseating granulomatous infiltrate (Fig. 13d). Lymphocytes and epithelioid histiocytes with abundant eosinophilic cytoplasm and oval vesicular nuclei are observed (H&E 250X). The clinical, radiological and histopathological patterns were consistent with the diagnosis of Heerfordt’s syndrome