
FIGURE 1.
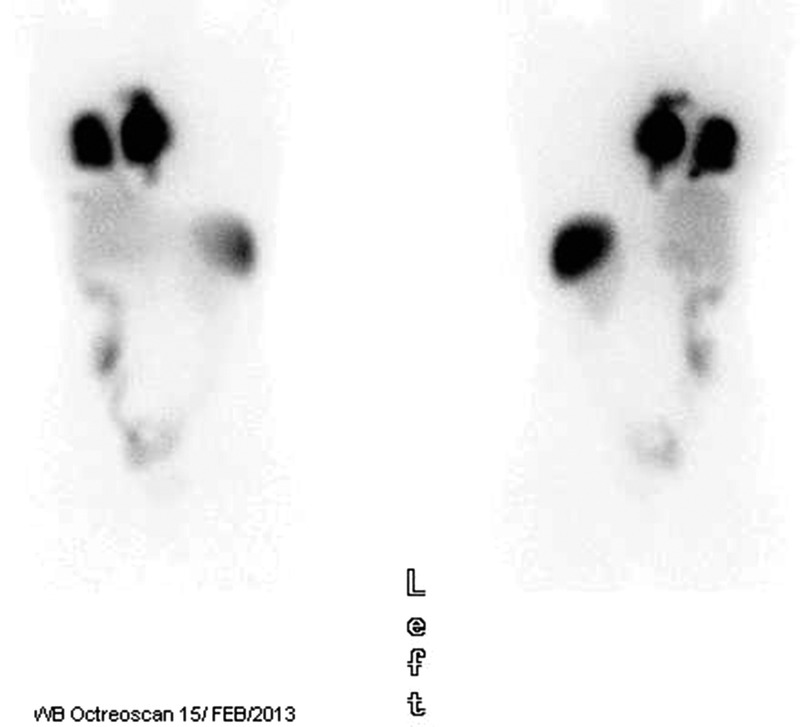
A 36-year-old woman with a diagnosis of a left popliteal synovial sarcoma treated with surgery and chemotherapy (adryamicin/ifosfamide). A local recurrence required additional surgery followed by chemoradiotherapy (70 Gy plus ifosfamide). She had a disease-free interval of 4 years until lung metastasis was detected. Between October 2007 and May 2012, she was treated with several drug combinations (in total, she had been resistant to >6 lines of therapy including all the available active drugs in soft tissue sarcomas) and operated by thoracotomy in 3 stages. Pazopanib treatment was initiated in November 2012 and then interrupted because of hemoptysis. She was referred to our institution in February 2013 presenting extreme weight loss and a performance status of 2. The most recent scan showed lung metastasis in more than 50% of the right side of the thorax, with large pleural disease and mediastinum involvement. Traqueal compression at carina level was present. A computed tomography–guided needle biopsy from a lung metastatic lesion was performed for an expression microarray. A highly significant expression of the somatostatin receptor 2 (SSTR2) gene (in excess of 10-fold) and to a lesser extent SSTR5 (>5-fold) as compared with the normal control tissue was apparent in the normalized microarray data. There are references in literature identifying SSTR in more than 80% of the soft tissue tumors analyzed by reverse transcriptase–polymerase chain reaction,1,2 as well as positive uptake in molecular imaging.3,4 Figure 1 shows the high uptake in the right hemithorax in the Octreoscan confirming the potential indication for somatostatin analog–based treatments. She began lanreotide 30 mg intramuscularly every 2 to 3 weeks until May 31, 2013, reaching disease stabilization.