

Abstract
Angioedema is a rare condition which manifests as sudden localised, non-pitting swelling of certain body parts including skin and mucous membranes. It is vital that anaesthesiologists understand this condition, as it may present suddenly in the perioperative period with airway compromise. To identify literature for this review, the authors searched the PubMed, Medline, Embase, Scopus and Web of Science databases for English language articles covering a 10-year period, 2006 through 2016. Angioedema can be either mast-cell mediated or bradykinin-induced. Older therapies for histaminergic symptoms are well known to anaesthesiologists (e.g., adrenaline, anti-histamines and steroids), whereas older therapies for bradykinin-induced symptoms include plasma and attenuated androgens. New classes of drugs for bradykinin-induced symptoms are now available, including anti-bradykinin, plasma kallikrein inhibitor and C1 esterase inhibitors. These can be used prophylactically or as rescue medications. Anaesthesiologists are in a unique position to coordinate perioperative care for this complex group of patients.
Key words: Airway, angioedema, bradykinin, C1 esterase inhibitor, histamine
INTRODUCTION
Angioedema is a rare condition that manifests itself by sudden localised, non-pitting swelling of certain body parts including skin and mucous membranes.[1,2] When an angioedema attack is triggered in the perioperative period, the anaesthesiologist may be faced with a confusing constellation of signs and symptoms that require effective, rapid intervention, especially when progressive airway compromise is evident. Indeed, multiple factors are present in the perioperative period that may predispose the patient to an attack of angioedema.[3]
The purpose of this narrative review is to provide the perioperative clinician with a historical perspective of this condition, an understanding of the aetiology and pathophysiology of angioedema, and a framework for both prophylactic and emergent treatment. It is imperative to distinguish between angioedema and anaphylaxis because while presentation may be similar, treatments differ. Emphasis will be placed on new and emerging therapies for angioedema that can be used in the perioperative period. To identify relevant medical literature for this review, the authors searched the PubMed, Medline, Embase, Scopus and Web of Science databases for English language articles covering a 10-year period, 2006 through 2016. Search terms included hereditary angioedema (HAE), acquired angioedema, icatibant, ecallantide and C1 esterase inhibitor (C1 INH). It is important to note that although the terms angioedema and urticaria have been used interchangeably, they possess distinct characteristics and require distinct treatment. Urticaria is a transient erythematous swelling of the skin, accompanied by itching and resolves within 24 h. On the other hand, angioedema is known for swelling which is due to oedema in the deeper dermal, cutaneous and sub-mucosal tissue. The skin itself may appear normal. Our review will focus on only angioedema.
HISTORICAL PERSPECTIVE
Although urticaria was first reported approximately 200 BC, angioedema itself was not described until the 1500's. The term ‘angioedema’ was first coined in 1586.[4] In the 19th century, a case of HAE was reported in a family where the common cause of death was ‘fatal suffocation’.[5] Angioedema received further recognition in the 1960's after cases were reported dating to the 17th century from Swedish church records, where it was common to register cause of death.[6] In 1963, it was discovered that patients with HAE possessed low levels of C1 INH.[7] First described in 1972, acquired angioedema was initially characterised by angioedema symptoms, C1-INH deficiency and hyperactivation of the complement pathway.
EPIDEMIOLOGY
The World Allergy Organisation states that urticaria and/or angioedema has been reported in up to 20% of the general population.[8] In addition, 40-50% of patients with chronic urticaria have angioedema. Angioedema can affect all age groups; however, those with a genetic basis present earlier in adolescence, with a peak incidence in the third decade of life.[8] Hospital admissions due to angioedema have also increased over the years with most cases in patients 65 years of age or older. Of note, females may have a predilection for angioedema since oestrogen has been seen to exacerbate a specific form of angioedema (HAE Type III, see below).[9,10] While there is no clear race predilection, African-Americans are at higher risk of angioedema while taking an angiotensin-converting enzyme inhibitor (ACEI).[11,12] Studies suggest this may be due to a genetic polymorphism, C-2399A of the XPNPEP gene, which is responsible for encoding the enzyme aminopeptidase P.[13] Interestingly, colloids (gelatins) have also been implicated as a cause of angioedema.
CLASSSIFICATION OF ANGIOEDEMA
There are a variety of types of angioedema. Broadly, there is mast-cell mediated and bradykinin-induced angioedema. A third subtype is also described – acquired angioedema of unknown origin.[14] As above, angioedema manifests by sudden, non-pitting swelling of certain body parts; dependent body parts (except feet) are not affected. This is in distinction to oedema from cardiac, renal or hepatic aetiologies, and also distinct from hives in terms of the location of extravasated fluid [Figure 1]. What follows is a description of each of the major subtypes of angioedema [Table 1].
Figure 1.
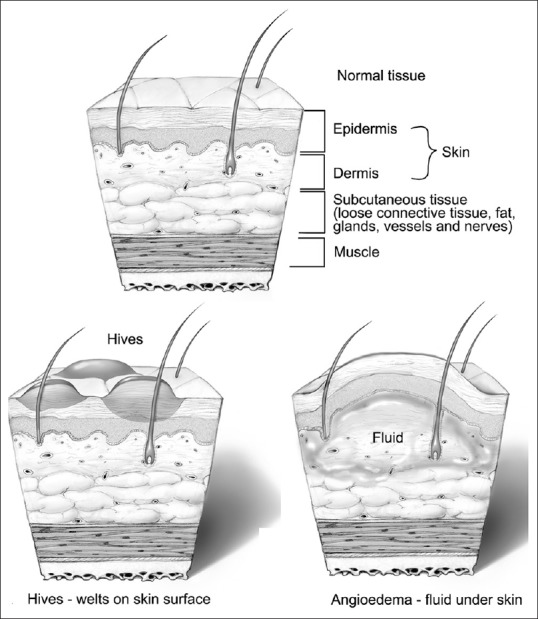
Location of extravasated fluid in hives versus angioedema. By permission of Mayo Foundation for Medical Education and Research. All rights reserved
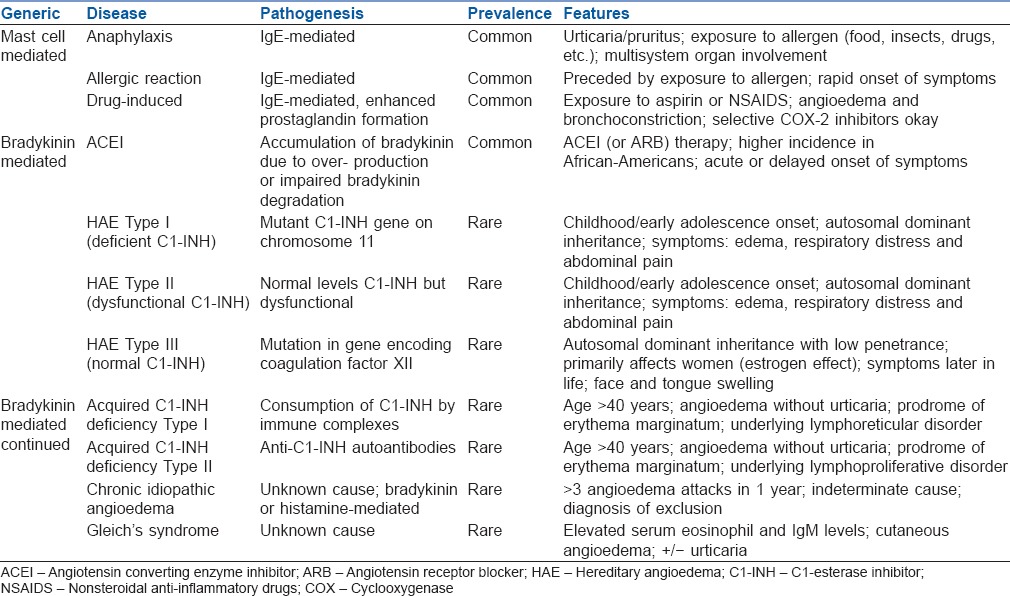
Table 1.
Classification of angioedema
Mast-cell mediated angioedema results from IgE-mediated degranulation of mast cells. The majority of cases are associated with urticaria and/or pruritus [Figure 2]. Anaphylaxis is a severe example of this type of angioedema, which is preceded by exposure to an allergen [Figure 3]. Allergic reactions without anaphylaxis can also give rise to angioedema. A distinguishing feature of allergic angioedema is its ‘temporal’ relationship to a trigger.[15] The onset of symptoms is typically rapid – minutes to a few hours after exposure.
Figure 2.
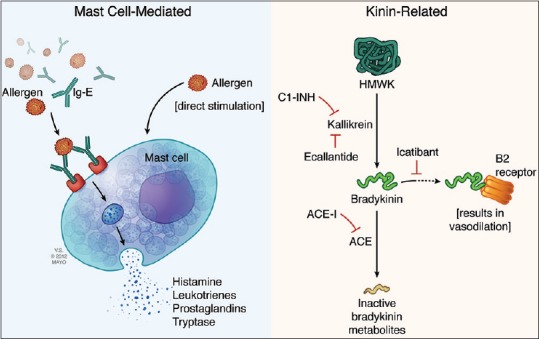
Mechanism of mast cell versus bradykinin mediated angioedema. By permission of Mayo Foundation for Medical Education and Research. All rights reserved
Figure 3.
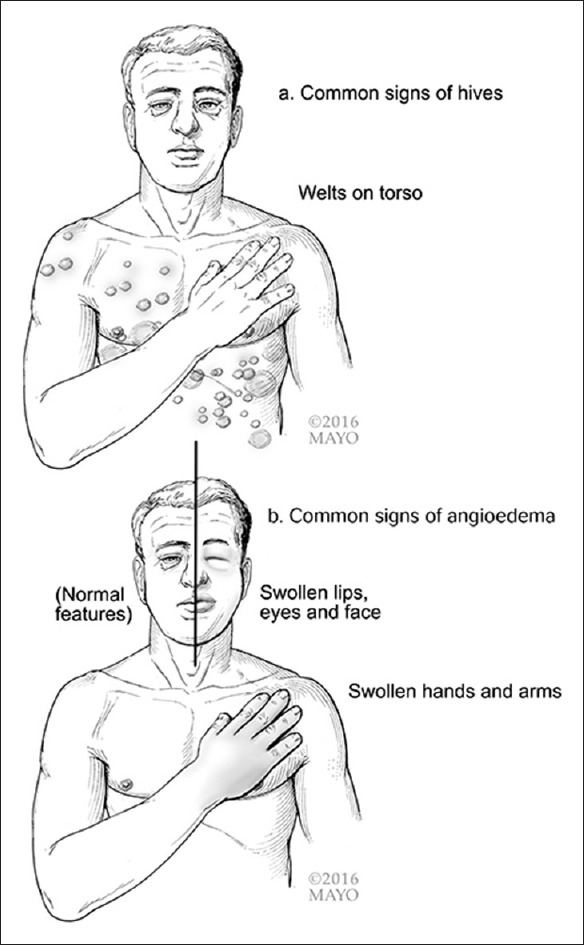
Common signs of hives versus angioedema. By permission of Mayo Foundation for Medical Education and Research. All rights reserved
Aspirin (ASA) and non-steroidal anti-inflammatory drugs (NSAIDS) can cause drug-induced histaminergic angioedema without anaphylaxis, most commonly effecting the periorbital and facial area. NSAID inhibition of cyclooxygenase (COX) promotes prostaglandin formation and other pro-inflammatory mediators, leading to angioedema and bronchoconstriction in susceptible individuals.[16] Interestingly, selective COX-2 inhibitors (e.g., celecoxib) are tolerated quite well by patients who have had angioedema-type reactions to COX-1 or non-selective COX inhibitors.[17,18]
Bradykinin-induced angioedema results from overproduction of bradykinin or inhibition of bradykinin degradation. Typically, mast cells are not involved in this type of angioedema. Therefore, pruritus and urticaria are noticeably absent. Mechanistically, activated factor XII cleaves prekallikrein to produce kallikrein [Figure 2]. Plasma kallikrein then cleaves kininogen to release bradykinin, which binds to B2 receptors on endothelial cells. To modulate bradykinin production, C1 INH inhibits plasma kallikrein and activated factor XII. If C1 INH is deficient in quantity or quality, an uninhibited contact system will produce excess bradykinin.[19]
Increased vascular permeability is caused by bradykinin, resulting in contraction of non-vascular smooth muscle, vasodilation and oedema formation.[20] In addition to the typical locations of swelling, bradykinin-induced angioedema affects the gastrointestinal mucosa.
The most common subtype of bradykinin-induced angioedema is due to ACEI therapy. The prevalence of ACEI induced angioedema ranges from 0.1% to 2.5%.[11,21] Roughly 20-30% of all angioedema cases in the emergency department can be traced to ACEI use.[22] In fact, 0.1–2.5% of patients treated with ACEI experience angioedema.[11,22,23] The onset of symptoms varies greatly, from hours to several years after initiation of ACEI.[11,14,24] The ACEI prevents degradation of bradykinin to inactive fragments with accumulation and enhanced half-life of bradykinin. In particular, African–Americans and immunosuppressed patients are at highest risk.[25,26] There is also the potential for latent angioedema attacks after discontinuation of an ACEI,[27] which can range from several weeks to years. The timeframe for a recurrent angioedema attack if the ACEI is not discontinued is about 10 months.[27]
HAE is another form of non-histaminergic angioedema. It is caused by mutations on the C1 INH gene on chromosome 11, which results in a nonfunctional copy of the SERPING1 gene.[28] The prevalence of HAE is between 1:10,000 and 1:50,000 in the United States.[23,29] It is transmitted in autosomal dominant fashion. In 25% of cases, there is a spontaneous mutation at the C1 INH gene that causes angioedema.[15,30] Often, this form of angioedema begins in childhood and worsens during puberty. Symptoms include severe oedema, respiratory distress and abdominal pain. HAE can be divided into three subtypes: HAE with C1 INH (serpin C1 INH) deficiency (Type I ~85%), HAE with normal (but dysfunctional) C1 INH (Type II ~15%), and HAE which is characterised with normal C1 INH (Type III, rare). Type III is primarily observed in women; it is often associated with oestrogen use. The pathology of Type III HAE is a mutation in the gene encoding for factor XII. Prekallikrein is cleaved to kallikrein by activated factor XII, ultimately generating bradykinin from high-molecular-weight kinin[28,31] [Figure 2]. Oestrogens can exacerbate this gene alteration.[31]
Finally, acquired C1 INH deficiency is a rare cause of angioedema. This form of angioedema can be subdivided into Type I and Type II (see below). In general, enzyme dysfunction is caused by abnormal levels or function of C1 INH, which leads to higher bradykinin levels. Ultimately, there is contact system activation.[32]
Type 1 acquired C1 INH deficiency is attributed to the increased consumption of C1 INH by immune complexes in certain disease states. It occurs predominantly in older patients (>40 years age) and is never associated with a family history.[14,33] In about 15% of cases, there is an underlying lymphoproliferative disorder and/or autoimmune disease, such as monoclonal gammopathy or lymphomas.[34,35] Angioedema with C1 INH deficiency will present with recurrent angioedema without urticaria. A characteristic rash, erythema marginatum, may precede the onset of angioedema. Type 2 acquired C1 INH deficiency is due to anti-C1 INH autoantibodies. These autoantibodies inactivate C1 INH which leads to angioedema.[15]
Considering that HAE and acquired angioedema present with similar symptoms, a detailed history and specialised laboratory tests are crucial in distinguishing between the two variants and ultimately selecting the correct treatment. A key component of the history is age of onset of symptoms.
Chronic idiopathic angioedema is defined as three or more episodes of angioedema within a 1 year period with an indeterminate cause.[15] This is different from the other types due to its association with urticaria, which is not seen in other forms of angioedema. Recurrent swelling that is generally associated with pruritus and urticaria is a hallmark of this subtype. This condition can mimic either bradykinin-mediated or mast-cell mediated angioedema. Patient response to antihistamine therapy is indicative of a mast-cell mediated process.[36,37]
Beyond the above-discussed types of angioedema, there are several rare and esoteric causes of angioedema. For example, Gleich's syndrome is characterised by cutaneous angioedema, with or without urticaria, and elevated serum eosinophil and IgM levels. The cause for Gleich's syndrome is unknown. While medication induced (NSAIDS, ASA and ACEI) angioedema is well-established, it's worth noting that angioedema has also been reported due to calcium channel blockers, rocuronium and propofol.[38,39,40]
Clinical presentation
Angioedema has multiple subtypes as described above, but at their core is a temporary increase in endothelial permeability which in turn leads to plasma extravasation in the deeper layers of the dermis and submucosa. While facial and genital skin is mostly affected, the extremities, airways and intestinal tract may also be involved.[15] Laryngeal involvement varies from mild oedema to severe respiratory distress and asphyxiation. Intestinal tract angioedema may present as abdominal pain with or without nausea, vomiting, diarrhoea and ascites which may be confused with a surgical abdomen.[15]
TREATMENTS FOR ANGIOEDEMA
When a patient with known angioedema develops signs and symptoms in the recovery room suggestive of an angioedema attack, a number of actions are appropriate. Airway assessment is primary. Findings suggestive of obstruction, such as stridor, retractions and paradoxical chest movement are worrisome. If there is evidence of progressive airway compromise from tongue swelling and/or laryngeal oedema, endotracheal intubation is likely to be necessary.
In addition to examination of the oropharynx, nasopharyngoscopy can be considered to evaluate the posterior pharynx and glottis. Patient comorbidities and baseline airway exam should also influence the decision to intubate the trachea versus other options. If endotracheal intubation is selected, issues of sedation versus induction of general anaesthesia before intubation must be addressed, in addition to airway approach (direct laryngoscopy, fibreoptic intubation, videolaryngoscopy, nasal or oral). Supraglottic airways are probably not useful in this setting due to the tongue and laryngeal involvement. Consultation with and the presence of an otolaryngologist is appropriate if available in a timely fashion.
Medication management in the acute setting – intraoperative attack of angioedema
Intra-operatively, it can be difficult to distinguish between anaphylaxis and an angioedema attack. Anaphylaxis may manifest as hypotension, tachycardia, increased airway pressures and rash. Suggestive of angioedema are swelling not associated with a rash; although, this is not pathognomonic. In this setting, initial treatment for anaphylaxis is reasonable; but if there is a lack of response, the clinician should consider treatments for angioedema as described below.
Medication management in the acute setting – patient with known angioedema
Patients with known angioedema who develop symptoms in the PACU should be treated according to the mechanism of swelling. Histamine-mediated angioedema should be treated with adrenaline if there are life-threatening signs and symptoms including airway involvement and low blood pressure. In addition, H-1 antagonists should be administered to reduce histamine related effects; intravenous diphenhydramine is an appropriate choice during urgent scenarios. H-2 blockers can be added to reduce histamine effects such as pruritus, urticaria and hypotension. Finally, although not immediately beneficial, corticosteroids can be administered to suppress inflammatory mediators.
Traditional and accepted management
For patients with known bradykinin associated angioedema, preventing the production of bradykinin or reducing its effect is crucial. Fresh-frozen plasma (FFP) can be administered in the acute setting because it provides C1 INH. The benefit of FFP would extend to patients reacting to an ACEI. However, FFP is not without risks including transmission of bloodborne pathogens, fluid overload and hypersensitivity reactions.
Newer therapies
There are a number of new, targeted therapies for acute attacks of HAE (non-histaminergic type). These US Food and Drug Administration (FDA) approved therapies may also have benefit in ACEI related angioedema; common therapies for histaminergic or anaphylactic aetiologies (adrenaline, H-1 antagonists, corticosteroids) are unlikely to be of benefit when dysregulation of bradykinin is the aetiology of the attack.
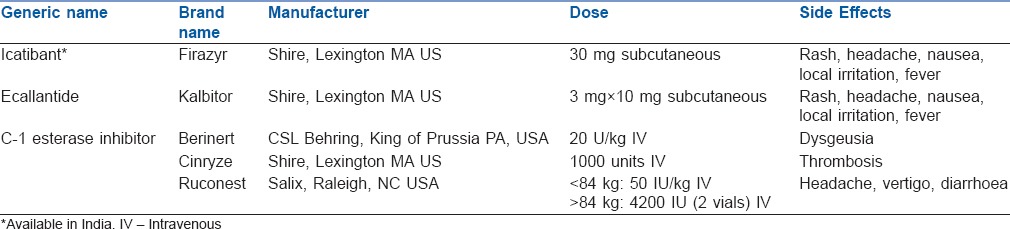
New therapies include: Icatibant (Firazyr®, Shire, Lexington MA, USA) is a synthetic bradykinin receptor antagonist.[33,41] The FDA has approved it for use by physicians or patients ≥18 years of age. A 30 mg dose is administered subcutaneously and can be repeated after 6 h if symptoms return, up to 3 times in 24 h. A number of common side effects include rash, headache, nausea, local irritation at the injection site and fever.
Ecallantide (Kalbitor®, Shire, Lexington MA, USA) was approved in the United States in 2009.[42] It is a plasma kallikrein inhibitor for patients 12 years of age or older which is administered via three subcutaneous injections of 10 mg each. Due to risk of anaphylactoid-type reactions (3%) it is approved for administration by health-care professionals only.[43] Most reactions to ecallantide develop within 1 h. Common side effects are similar to icatibant.
C1 INH is available from several sources, including two products which are plasma derived (Berinert, Cinryze) and a recombinant C1 INH (Ruconest). Berinert® (CSL Behring, King of Prussia PA, USA) is a C1 INH that is a plasma product. It is approved for the treatment of acute HAE attacks involving facial, abdominal, or laryngeal regions in adults and adolescents.[44] The dose is 20 U/kg of body weight, administered intravenously. Since Berinert is a plasma product, there is a risk of infection. Dysgeusia was reported in >4% of patients receiving Berinert infusions (vs. 0%, placebo group).[45] Cinryze® (Shire, Lexington MA, USA) is a similar product with similar safety considerations, risks and side effects. However, Cinryze is approved for intravenous home infusion to prevent HAE attacks. It is administered every 3-4 days in a dose of 1000 units. There have been reports of thrombosis after C1 INH product administration for long-term HAE prophylaxis.[43] Finally, Ruconest® (Salix, Raleigh NC, USA) is a recombinant C1 INH approved for acute HAE attacks [Table 2]. Our review suggests that at a minimum, Icatibant is currently being used in some parts of India.
Table 2.
New treatments for angioedema
PROPHYLAXIS AGAINST ANGIOEDEMA ATTACKS
For patients with known angioedema, the need for prophylaxis before a procedure is driven by diagnosis, personal history and the magnitude of the planned procedure. Multispeciality planning is crucial when caring for patients with angioedema. Many physicians are not familiar with this rare condition. Moreover, anaesthesiologists can play an important coordinating role as perioperative physicians.
Risk factors for attacks in the perioperative period include oral trauma (including instrumentation of the airway), stress, and surgical procedures in the airway itself. A number of reports describe anaesthetic management during various surgical procedures.[33,46,47] Anaesthesia techniques that may reduce the risk of angioedema in the perioperative period include avoidance of instrumenting the airway and even general anaesthesia if possible. Pretreatment with attenuated androgens, C1 INH or FFP is appropriate (see details below) and availability of rescue medications is crucial, including icatibant, ecallantide, C1 INH (either recombinant or plasma derived), or plasma.
Attenuated androgens (most commonly danazol) are thought to increase C1 INH via stimulation of hepatic synthesis among other mechanisms.[48] When used in the lowest effective dose possible for long-term prophylaxis, they appear to have minimal or no virilising side effects, even in female patients, although they should only be used for adults.[49] As a short course of prophylaxis before a procedure, danazol can be prescribed at a dose of 200 mg tid for 5 days preoperatively and 3 days post-operatively.
C1 INH concentrate can be used for short-term prophylaxis 1 h before the procedure in a dose of 1000 units or 20 units/kg. Alternatively, two units of FFP can be administered 1 h before the procedure, but plasma is a less desirable option for reasons noted above.
While prophylaxis before a scheduled procedure is reasonable, another option is to only have medications available to abort an angioedema attack. This approach can be considered if the patient is deemed to be low-risk and the procedure is considered low-risk as well, e.g., surgery that does not require airway manipulation.
MANAGEMENT OF PATIENTS AFTER AN ANGIOEDEMA ATTACK
Once an acute attack of angioedema has stabilised, a number of decisions must be made regarding patient disposition. Consultation with an allergist/immunologist is appropriate for on-going management and advice regarding future prophylactic and abortive therapies.
Obviously if the patient required intubation, Intensive Care Unit (ICU) admission will be necessary. If endotracheal intubation was not necessary, a number of factors can be considered to determine the need for observation on the hospital ward versus ICU versus discharge home. The extent and severity of airway involvement is a primary driver of this decision. Typically, in cases of resolving angioedema involving the face, lips and anterior tongue, the patient can be discharged home or observed on the hospital ward.[50] Conversely, if the patient has evidence of laryngeal involvement, observation in ICU is appropriate. Consultation with an otolaryngologist may be indicated with nasopharyngoscopy to define the involved anatomic regions.
ADDITIONAL TESTING AND FOLLOW-UP
Follow-up should be provided for the patient, depending on their history of angioedema and available resources. New symptoms should trigger a consultation with an allergist/immunologist. If there is suspicion that the episode was triggered by an ACEI, the medication should be held and the prescribing provider notified. A plan for recurrent symptoms should be established, with clear instructions for the patient. Depending on the aetiology of their angioedema, a specific treatment should be made available to them, such as the abortive therapies described above.
Additional testing can be ordered soon after an episode. After an acute attack, C4 levels should be obtained if possible to assist with the diagnosis of HAE, and tryptase level to diagnose anaphylaxis associated with angioedema. Low C4 is associated with HAE and is therefore a good screening test for C1 INH deficiency. Tryptase is normal in HAE but in mast-cell disorders or other causes of anaphylaxis manifesting as angioedema, it may be elevated.
These tests are not ‘point of care’ and as such, they will not guide acute management of angioedema attacks. However, they will be useful for long term management decisions. Obtaining blood samples at the time of the attack will assure they are available for subsequent consultations. Patient and family education is obviously vital throughout the process of diagnosis and treatment of angioedema. In addition, the patient can be offered a ‘Medalert’ bracelet and card.
SUMMARY
Angioedema, with its intermittent and sudden swelling of certain body parts, can be particularly challenging for perioperative physicians. During a surgical episode of care, patients with angioedema are at increased risk of angioedema attacks; airway involvement can be life threatening. Fortunately, anaesthesiologists are in a unique position to coordinate perioperative care for these patients, including prophylactic treatment, abortive therapy and airway management. New classes of drugs, including anti-bradykinin, plasma kallikrein inhibitor and C1 INHs provide additional tools for the perioperative clinician to manage this complex group of patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Bork K. Hereditary angioedema with normal C1 inhibitor activity including hereditary angioedema with coagulation factor XII gene mutations. Immunol Allergy Clin North Am. 2006;26:709–24. doi: 10.1016/j.iac.2006.09.003. [DOI] [PubMed] [Google Scholar]
- 2.Kaplan AP, Greaves MW. Angioedema. J Am Acad Dermatol. 2005;53:373–88. doi: 10.1016/j.jaad.2004.09.032. [DOI] [PubMed] [Google Scholar]
- 3.Williams AH, Craig TJ. Perioperative management for patients with hereditary angioedema. Allergy Rhinol (Providence) 2015;6:50–5. doi: 10.2500/ar.2015.6.0112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Donati G. Statistico-clinical considerations on burn patients treated in the clinica dermatologica di modena during the 1956-1960 period. Arch Ital Dermatol Venereol Sessuol. 1962;31:304–12. [PubMed] [Google Scholar]
- 5.Osler W. Hereditary angioneurotic edema. Am J Med Sci. 1888;95:362. [Google Scholar]
- 6.Arnoldsson H, Belin L, Hallberg L, Helander E, Lindholm B, Westling H. Hereditary periodic oedema. Acta Med Scand. 1967;181:115–24. doi: 10.1111/j.0954-6820.1967.tb07235.x. [DOI] [PubMed] [Google Scholar]
- 7.Donaldson VH, Evans RR. A biochemical abnormality in herediatry angioneurotic edema: Absence of serum inhibitor of c’ 1-esterase. Am J Med. 1963;35:37–44. doi: 10.1016/0002-9343(63)90162-1. [DOI] [PubMed] [Google Scholar]
- 8.Mansi M, Zanichelli A, Coerezza A, Suffritti C, Wu MA, Vacchini R, et al. Presentation, diagnosis and treatment of angioedema without wheals: a retrospective analysis of a cohort of 1058 patients. J Intern Med. 2015;277:585–93. doi: 10.1111/joim.12304. [DOI] [PubMed] [Google Scholar]
- 9.Bouillet L, Ponard D, Drouet C, Jullien D, Massot C. Angioedema and oral contraception. Dermatology. 2003;206:106–9. doi: 10.1159/000068456. [DOI] [PubMed] [Google Scholar]
- 10.Hentges F, Hilger C, Kohnen M, Gilson G. Angioedema and estrogen-dependent angioedema with activation of the contact system. J Allergy Clin Immunol. 2009;123:262–4. doi: 10.1016/j.jaci.2008.10.056. [DOI] [PubMed] [Google Scholar]
- 11.Kostis JB, Kim HJ, Rusnak J, Casale T, Kaplan A, Corren J, et al. Incidence and characteristics of angioedema associated with enalapril. Arch Intern Med. 2005;165:1637–42. doi: 10.1001/archinte.165.14.1637. [DOI] [PubMed] [Google Scholar]
- 12.Mahoney EJ, Devaiah AK. Angioedema and angiotensin-converting enzyme inhibitors: are demographics a risk? Otolaryngol Head Neck Surg. 2008;139:105–8. doi: 10.1016/j.otohns.2008.03.029. [DOI] [PubMed] [Google Scholar]
- 13.Woodard-Grice AV, Lucisano AC, Byrd JB, Stone ER, Simmons WH, Brown NJ. Sex-dependent and race-dependent association of XPNPEP2 C-2399A polymorphism with angiotensin-converting enzyme inhibitor-associated angioedema. Pharmacogenet Genomics. 2010;20:532–6. doi: 10.1097/FPC.0b013e32833d3acb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cicardi M, Aberer W, Banerji A, Bas M, Bernstein JA, Bork K, et al. Classification, diagnosis, and approach to treatment for angioedema: Consensus report from the Hereditary Angioedema International Working Group. Allergy. 2014;69:602–16. doi: 10.1111/all.12380. [DOI] [PubMed] [Google Scholar]
- 15.Nzeako UC, Longhurst HJ. Many faces of angioedema: Focus on the diagnosis and management of abdominal manifestations of hereditary angioedema. Eur J Gastroenterol Hepatol. 2012;24:353–61. doi: 10.1097/MEG.0b013e3283517998. [DOI] [PubMed] [Google Scholar]
- 16.Agostoni A, Cicardi M. Drug-induced angioedema without urticaria. Drug Saf. 2001;24:599–606. doi: 10.2165/00002018-200124080-00004. [DOI] [PubMed] [Google Scholar]
- 17.Fontaine C, Bousquet PJ, Demoly P. Anaphylactic shock caused by a selective allergy to celecoxib, with no allergy to rofecoxib or sulfamethoxazole. J Allergy Clin Immunol. 2005;115:633–4. doi: 10.1016/j.jaci.2004.10.045. [DOI] [PubMed] [Google Scholar]
- 18.Zembowicz A, Mastalerz L, Setkowicz M, Radziszewski W, Szczeklik A. Safety of cyclooxygenase 2 inhibitors and increased leukotriene synthesis in chronic idiopathic urticaria with sensitivity to nonsteroidal anti-inflammatory drugs. Arch Dermatol. 2003;139:1577–82. doi: 10.1001/archderm.139.12.1577. [DOI] [PubMed] [Google Scholar]
- 19.Tse K, Zuraw BL. Recognizing and managing hereditary angioedema. Cleve Clin J Med. 2013;80:297–308. doi: 10.3949/ccjm.80a.12073. [DOI] [PubMed] [Google Scholar]
- 20.Hsu D, Shaker M. An update on hereditary angioedema. Curr Opin Pediatr. 2012;24:638–46. doi: 10.1097/MOP.0b013e328357b25e. [DOI] [PubMed] [Google Scholar]
- 21.Miller DR, Oliveria SA, Berlowitz DR, Fincke BG, Stang P, Lillienfeld DE. Angioedema incidence in US veterans initiating angiotensin-converting enzyme inhibitors. Hypertension. 2008;51:1624–30. doi: 10.1161/HYPERTENSIONAHA.108.110270. [DOI] [PubMed] [Google Scholar]
- 22.Bernstein JA, Moellman J. Emerging concepts in the diagnosis and treatment of patients with undifferentiated angioedema. Int J Emerg Med. 2012;5:39. doi: 10.1186/1865-1380-5-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moellman JJ, Bernstein JA, Lindsell C, Banerji A, Busse PJ, Camargo CA, Jr, et al. A consensus parameter for the evaluation and management of angioedema in the emergency department. Acad Emerg Med. 2014;21:469–84. doi: 10.1111/acem.12341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Stojiljkovic L. Renin-angiotensin system inhibitors and angioedema: anesthetic implications. Curr Opin Anaesthesiol. 2012;25:356–62. doi: 10.1097/ACO.0b013e328352dda5. [DOI] [PubMed] [Google Scholar]
- 25.Burkhart DG, Brown NJ, Griffin MR, Ray WA, Hammerstrom T, Weiss S. Angiotensin converting enzyme inhibitor-associated angioedema: Higher risk in blacks than whites. Pharmacoepidemiol Drug Saf. 1996;5:149–54. doi: 10.1002/(SICI)1099-1557(199605)5:3<149::AID-PDS222>3.0.CO;2-I. [DOI] [PubMed] [Google Scholar]
- 26.Lin RY, Levine RJ, Lin H. Adverse drug effects and angioedema hospitalizations in the United States from 2000 to 2009. Allergy Asthma Proc. 2013;34:65–71. doi: 10.2500/aap.2013.34.3618. [DOI] [PubMed] [Google Scholar]
- 27.Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26:725–37. doi: 10.1016/j.iac.2006.08.001. [DOI] [PubMed] [Google Scholar]
- 28.Levy JH, Freiberger DJ, Roback J. Hereditary angioedema: Current and emerging treatment options. Anesth Analg. 2010;110:1271–80. doi: 10.1213/ANE.0b013e3181d7ac98. [DOI] [PubMed] [Google Scholar]
- 29.Zuraw BL. Clinical practice. Hereditary angioedema. N Engl J Med. 2008;359:1027–36. doi: 10.1056/NEJMcp0803977. [DOI] [PubMed] [Google Scholar]
- 30.Johnston DT. Diagnosis and management of hereditary angioedema. J Am Osteopath Assoc. 2011;111:28–36. [PubMed] [Google Scholar]
- 31.Cichon S, Martin L, Hennies HC, Müller F, Van Driessche K, Karpushova A, et al. Increased activity of coagulation factor XII (Hageman factor) causes hereditary angioedema type III. Am J Hum Genet. 2006;79:1098–104. doi: 10.1086/509899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Konings J, Cugno M, Suffritti C, Ten Cate H, Cicardi M, Govers-Riemslag JW. Ongoing contact activation in patients with hereditary angioedema. PLoS One. 2013;8:e74043. doi: 10.1371/journal.pone.0074043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cicardi M, Banerji A, Bracho F, Malbrán A, Rosenkranz B, Riedl M, et al. Icatibant, a new bradykinin-receptor antagonist, in hereditary angioedema. N Engl J Med. 2010;363:532–41. doi: 10.1056/NEJMoa0906393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bernstein JA, Ritchie B, Levy RJ, Wasserman RL, Bewtra AK, Hurewitz DS, et al. Hereditary angioedema: Validation of the end point time to onset of relief by correlation with symptom intensity. Allergy Asthma Proc. 2011;32:36–42. doi: 10.2500/aap.2011.32.3404. [DOI] [PubMed] [Google Scholar]
- 35.Cicardi M, Zingale LC, Pappalardo E, Folcioni A, Agostoni A. Autoantibodies and lymphoproliferative diseases in acquired C1-inhibitor deficiencies. Medicine (Baltimore) 2003;82:274–81. doi: 10.1097/01.md.0000085055.63483.09. [DOI] [PubMed] [Google Scholar]
- 36.Cicardi M, Bergamaschini L, Zingale LC, Gioffré D, Agostoni A. Idiopathic nonhistaminergic angioedema. Am J Med. 1999;106:650–4. doi: 10.1016/s0002-9343(99)00123-0. [DOI] [PubMed] [Google Scholar]
- 37.Zingale LC, Beltrami L, Zanichelli A, Maggioni L, Pappalardo E, Cicardi B, et al. Angioedema without urticaria: a large clinical survey. CMAJ. 2006;175:1065–70. doi: 10.1503/cmaj.060535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Jeong WJ, Kim WY, Son JH, Lee YS, Kim JH, Park YC. Anaphylaxis with angioedema by rocuronium during induction of general anesthesia – A case report. Korean J Anesthesiol. 2010;58:391–5. doi: 10.4097/kjae.2010.58.4.391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Turcu AF, White JA, Kulaga ME, Skluth M, Gruss CB. Calcium channel blocker-associated small bowel angioedema. J Clin Gastroenterol. 2009;43:338–41. doi: 10.1097/MCG.0b013e31815cf6b9. [DOI] [PubMed] [Google Scholar]
- 40.You BC, Jang AS, Han JS, Cheon HW, Park JS, Lee JH, et al. A case of propofol-induced oropharyngeal angioedema and bronchospasm. Allergy Asthma Immunol Res. 2012;4:46–8. doi: 10.4168/aair.2012.4.1.46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Zanichelli A, Badini M, Nataloni I, Montano N, Cicardi M. Treatment of acquired angioedema with icatibant: A case report. Intern Emerg Med. 2011;6:279–80. doi: 10.1007/s11739-010-0431-4. [DOI] [PubMed] [Google Scholar]
- 42.Cicardi M, Levy RJ, McNeil DL, Li HH, Sheffer AL, Campion M, et al. Ecallantide for the treatment of acute attacks in hereditary angioedema. N Engl J Med. 2010;363:523–31. doi: 10.1056/NEJMoa0905079. [DOI] [PubMed] [Google Scholar]
- 43.Craig T, Aygören-Pürsün E, Bork K, Bowen T, Boysen H, Farkas H, et al. WAO guideline for the management of hereditary angioedema. World Allergy Organ J. 2012;5:182–99. doi: 10.1097/WOX.0b013e318279affa. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.De Serres J, Gröner A, Lindner J. Safety and efficacy of pasteurized C1 inhibitor concentrate (Berinert P) in hereditary angioedema: A review. jean.de.serres@aventis.com. Transfus Apher Sci. 2003;29:247–54. doi: 10.1016/j.transci.2003.08.006. [DOI] [PubMed] [Google Scholar]
- 45.Craig TJ, Levy RJ, Wasserman RL, Bewtra AK, Hurewitz D, Obtulowicz K, et al. Efficacy of human C1 esterase inhibitor concentrate compared with placebo in acute hereditary angioedema attacks. J Allergy Clin Immunol. 2009;124:801–8. doi: 10.1016/j.jaci.2009.07.017. [DOI] [PubMed] [Google Scholar]
- 46.Christensen E, Hurewitz D, Sullivan S. Successful hereditary angioedema prophylaxis with C1 inhibitor in orthognathic surgery. J Oral Maxillofac Surg. 2012;70:1456–8. doi: 10.1016/j.joms.2011.03.061. [DOI] [PubMed] [Google Scholar]
- 47.Hermans C. Successful management with C1-inhibitor concentrate of hereditary angioedema attacks during two successive pregnancies: A case report. Arch Gynecol Obstet. 2007;276:271–6. doi: 10.1007/s00404-007-0329-1. [DOI] [PubMed] [Google Scholar]
- 48.Pappalardo E, Zingale LC, Cicardi M. Increased expression of C1-inhibitor mRNA in patients with hereditary angioedema treated with Danazol. Immunol Lett. 2003;86:271–6. doi: 10.1016/s0165-2478(03)00029-4. [DOI] [PubMed] [Google Scholar]
- 49.Zotter Z, Veszeli N, Csuka D, Varga L, Farkas H. Frequency of the virilising effects of attenuated androgens reported by women with hereditary angioedema. Orphanet J Rare Dis. 2014;9:205. doi: 10.1186/s13023-014-0205-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ishoo E, Shah UK, Grillone GA, Stram JR, Fuleihan NS. Predicting airway risk in angioedema: staging system based on presentation. Otolaryngol Head Neck Surg. 1999;121:263–8. doi: 10.1016/S0194-5998(99)70182-8. [DOI] [PubMed] [Google Scholar]