
Fig. 6.
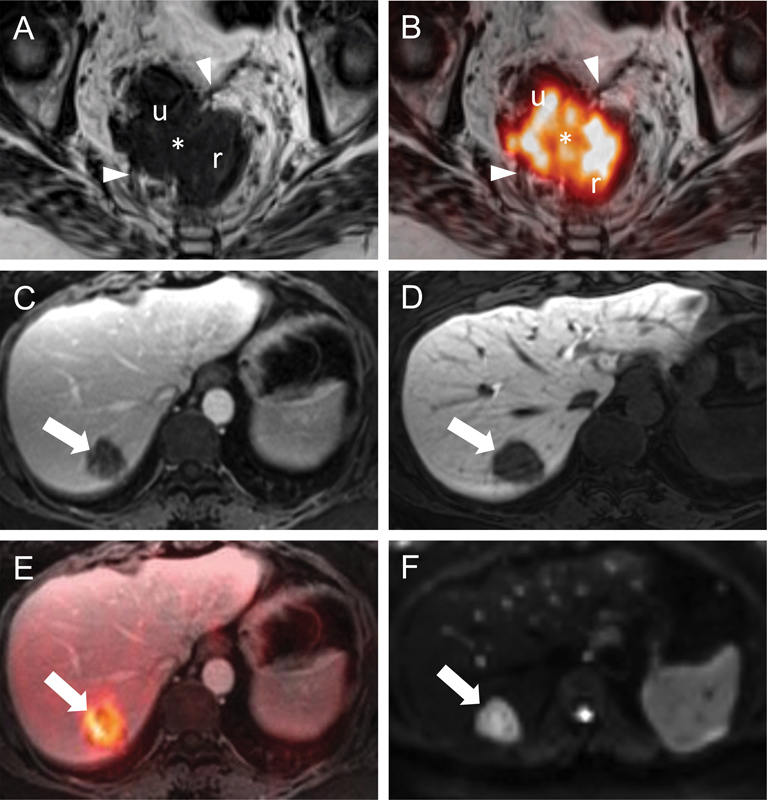
Locoregional and hepatic staging of rectal cancer by PET/MRI. Transaxial T2WIs (A) through the rectum (r) show a right anterolateral rectal tumor (asterisk) that invades the mesorectal fascia (arrowheads). The relationship of the tumor (i.e., abutment vs. invasion) to the uterus (u) is unclear on this image alone. Transaxial T2WIs with FDG-PET fusion (B) at the same level better delineate the borders of this FDG-avid mass (asterisk) with respect to the mesorectal fascia (arrowheads) and confirm invasion of the left posterolateral aspect of the uterus (u). A normal-sized right internal iliac lymph node (not shown) was also FDG-avid and suspicious for regional nodal disease. Transaxial T1WIs (C and D) obtained with gadoxetic acid (Eovist, Bayer HealthCare LLC., Whippany, NJ) in the portal venous (C) and hepatobiliary (D) phases show a well-defined hypointense mass (arrows). This mass is FDG-avid on the fused FDG-PET images (arrow in [E]) and diffusion-restricting on DWI (arrow in [F]). These findings are consistent with a colorectal liver metastasis. DWI, diffusion-weighted imaging; FDG, 2-deoxy-2-[18F]fluoro-D-glucose; PET; positron emission tomography; MRI, magnetic resonance imaging; T2WI, T2-weighted images.