

Abstract
Background
Conflicts arising from cultural diversity among patients and hospital staff in China have become intense. Hospitals have an urgent need to improve transcultural self-efficacy of nurses for providing effective transcultural nursing.
Objective
The purpose of the research was to (a) evaluate the current status of perceived transcultural self-efficacy of nurses in general hospitals in Guangzhou, China; (b) explore associations between demographic characteristics of nurses and their perceived transcultural self-efficacy; and (c) assess the reliability and validity of scores on the Chinese version of the Transcultural Self-Efficacy Tool (TSET).
Methods
A cross-sectional survey of registered nurses from three general hospitals was conducted. Quota and convenience sampling were used. Participants provided demographic information and answered questions on the TSET.
Results
A total of 1,156 registered nurses took part. Most nurses had a moderate level of self-efficacy on the Cognitive (87.9%), Practical (87%), and Affective (89.2%) TSET subscales. Nurses who were older; who had more years of work experience, higher professional titles, higher incomes, and a minority background; and who were officially employed (not temporary positions) had higher perceived transcultural self-efficacy. Reliability estimated using Cronbach’s alpha was .99 for the total TSET score; reliability for the three subscales ranged from .97 to .98. Confirmatory factor analysis of TSET scores showed good fit with a three-factor model.
Conclusion
The results of this study can provide insights and guidelines for hospital nursing management to facilitate design of in-service education systems to improve transcultural self-efficacy of nurses.
Key Words: China, continuing education, immigration, in-migration, nurse, self-efficacy, transcultural nursing
China is a multiethnic country. The majority of the population belongs to the Han ethnic group. In the Chinese context, “minorities” refers to people from ethnicities other than Han (Jiang, 2010). In China, there are cultural differences in habits, language, religion, dietary habits, and value systems between the Han ethnic group and minorities. This unique cultural difference contributes to the phenomenon of a Chinese culture with multiple subcultures (Zhou, 2014).
With the acceleration of global economic integration, immigration from the Southern Hemisphere to the Northern Hemisphere or from the countryside to cities leads to cultural differences (Bernal & Froman, 1993). China began the process of reform and opening up in 1978, along with an improvement in the market economy. Advances in industrialization and urbanization and domestic migration from the countryside to large cities began. Domestic migration has become a prominent issue because a large number of farmers who were originally dependent on the land and minorities who had inhabited the frontier (plateaus, mountains, grasslands, and forest areas) for generations have flocked to cities in which most residents are from the Han ethnic group (N. Li, 2013). When aboriginal minorities come from the economically and socially less-developed rural areas, pastoral areas, and the western frontier to metropolises with a dominant Han culture, they encounter not only urban–rural differences but also the more prominent ethnic cultural differences (Xing & LI, 2011). Berry and Sabatier (2010) also consider that, similar to international migrants, migrants within a country also experience cultural differences. Leininger (1991) and Cronin and Harrison (1988) believe that cultural differences between majority and minority cultures within the same country require transcultural nursing care: Nurses should be sensitive and understand the patient’s worldview, religion, economic status, political view, education, language, gender, and health beliefs.
Guangzhou is an international metropolis in a developed region of China with a resident population of 12,700,800 (National Bureau of Statistics of China, 2011). Its developed economy has provided employment opportunities that attract minorities from enclaves in western China, such as Xinjiang, Xizang, Qinghai, and Ningxia. Data from 2010 revealed that there are 55 minority groups in Guangzhou comprising a total population of 635,900. There is one immigrant from another province for every three people in the resident population in Guangzhou (National Bureau of Statistics of China, 2011).
Compared with migration issues during urbanization—which were caused by a domestic rural minority labor force migrating into the cities—the foreign population flocking to Guangzhou is more challenging and has created an increasingly significant multicultural convergence (Q. Li, 2013). Guangzhou has a geographic location adjacent to Hong Kong and Macao and has become a major habitation for foreigners in China. Guangzhou contains one third of the foreign population in China; there are 600,000 foreign residents in Guangzhou (National Bureau of Statistics of China, 2011).
Multicultural convergence has also brought religious diversity to Guangzhou. As an example, there are currently approximately 300,000 Muslims in Guangdong Province, among whom 150,000 are domestic migrants and 150,000 are foreigners (mainly from the Middle East, Southeast Asia, Africa, and other countries and regions; National Bureau of Statistics of China, 2011).
The influx of migrants has posed serious challenges for public services in Guangzhou, including health services. General hospitals are the major medical resources in Guangzhou, and patient treatment and hospitalization are also concentrated at the general hospitals (Jiang, 2013). Within Chinese hospitals, incidents of physician–patient conflicts have become more intense and occurrences are increasing (Wang, Wang, Cheng, & Gao, 2013). Cultural conflicts between nurses and patients have emerged along with the overall pressure on medical resource supply.
Cultural conflicts between nurses and patients have emerged along with the overall pressure on medical resource supply.
Nurses in Guangzhou general hospitals receive their core basic education and their vocational education in nursing under the predominant Han culture. Their living and work environments reflect the city’s mainstream culture. However, domestic and foreign immigrants have their national psychology, cultures, value systems, religious beliefs, and social customs (N. Li, 2013). Taking language as an example, Guangzhou is the city with the most serious multilingual conflicts in China. Cantonese, the predominant dialect, is the main language used by Guangzhou natives; it is second only to the official language Mandarin in China. Cantonese is very different from Mandarin in pronunciation, vocabulary, and grammar and has relatively independent pronunciation, systematic vocabulary, and grammar specifications (Qian, 2010). Over 60 million local people use Cantonese, and Cantonese dominates the television media in Guangzhou (Li, 2012). In 2010, Guangzhou natives had a heated online debate and even public demonstration related to “promoting Mandarin versus defending Cantonese.” This rapid development and strong impact has caused widespread concern among Chinese people abroad; there has rarely been a precedent such as this in China (Xiao, 2010). The working language of hospital nurses is Mandarin. However, many of the nurses in Guangzhou’s hospitals are not from Guangzhou, and thus, they have significant difficulties communicating with local patients who only speak Cantonese.
Many of the nurses in Guangzhou’s hospitals are not from Guangzhou, and thus, they have significant difficulties communicating with local patients who only speak Cantonese.
The growing likelihood of encountering patients from different countries, ethnic groups, or cultural backgrounds requires Chinese nurses to have transcultural nursing knowledge and skills to meet their patients’ needs. Cultural competence is defined as “the attitude, knowledge and skills required to provide quality nursing to patients with cultural differences”; to provide safe and effective nursing care, nurses must have the cultural competence to understand and respond to a patient’s perception of disease and health; their language and worldview; and cultural, social, economic, and other factors (Calvillo et al., 2009).
Bandura’s (1986) self-efficacy theory is the important theoretical basis for this study. Bandura’s self-efficacy refers to people’s confidence or belief in their ability to achieve behavioral goals in specific fields such as transcultural nursing care. Transcultural self-efficacy is defined as “a nurse’s confidence when providing nursing care for patients from different cultural backgrounds” (Jimenez, Contreras, Shellman, Gonzalez, & Bernal, 2006). Some studies (Bernal & Froman, 1993; Geissler, 1992; Leininger, 1991; Rooda, 1993) have indicated that a nurse’s lack of perceived transcultural self-efficacy will cause patients with cultural differences to feel discriminated against and miscommunicated with and can lead to incorrect diagnoses and invalid nursing interventions. One study showed that nurses’ lack of perceived transcultural self-efficacy can cause increased depression and pain in patients (Davidhizar & Giger, 2004). Jeffreys (2010a) used Bandura’s (1986) model to propose that an individual with a high level of perceived self-efficacy (confidence) will take the initiative to seek knowledge that improves personal transcultural nursing skill and cultural competence. Nurses must increase their level of transcultural self-efficacy to improve their cultural competence to care for an increasing number of patients with cultural differences (Coffman, Shellman, & Bernal, 2004; Leininger, 1991).
Improving hospital nurses’ transcultural nursing skills and, thus, their perceived transcultural self-efficacy has become a pressing issue for Chinese nursing management. However, for some time, nursing education in China has been overly focused on basic medical education to the neglect of education in the humanities, resulting in an absence or shortage of transcultural nursing education (Zhang, Peng, Yu, & Xu, 2010). Therefore, student nurses and clinical nurses receive very little training in transcultural nursing. Providing continuing education targeted to nurses with various demographic characteristics could help to improve their transcultural self-efficacy and thus their transcultural nursing capability (Dawson & Lighthouse, 2010). No study providing the relevant background data has been conducted in China. The reason that no scholars or studies in China have proposed continuing education programs for transcultural nursing is that no one has analyzed the training needs of different nurse groups from an empirical perspective.
Purpose
The purpose of our study is to assess the current perceived transcultural self-efficacy among nurses in Guangzhou and to discuss the demographic characteristics related to perceived transcultural self-efficacy. To that effect, this study aimed to (a) evaluate nurses’ perceived transcultural self-efficacy, (b) explore demographic characteristics in relation to perceived transcultural self-efficacy, and (c) asses the reliability and validity of scores on the Transcultural Self-Efficacy Tool-Chinese Version (TSET-CV).
Methods
Design
The study is a cross-sectional survey. The survey was completed in 2015. The TSET-CV was used to assess the current levels of nurses’ perceived self-efficacy at hospitals in Guangzhou.
Sample
Nurses from three general hospitals in Guangzhou, China, completed the survey. The inclusion criteria were: (a) registered nurses and (b) nurses who were directly involved in patient care. Nursing staff sizes of the three hospitals varied in a 3:1:1 ratio. Within hospitals, nurses were sampled at convenience until the entire sample composition was approximately 60%, 20%, and 20% from the three hospitals, respectively.
Instrumentation
The TSET-CV scale was translated from the English version of the Transcultural Self-Efficacy Tool (TSET; Jeffreys, 2010a; Jeffreys, 2010b). The TSET is mainly used to measure and assess self-efficacy in using transcultural nursing skills to treat patients from different cultures. Many scholars have used the TSET to measure the transcultural self-efficacy perceptions of nursing students and nurses (Jeffreys, 2010a; Jeffreys & Dogan, 2010; Jeffreys & Smodlaka, 1999).
In this study, we obtained a permission license to use the TSET from Springer Publishing Company. The transcultural translation and adjustment of the scale followed the guidelines of the American Academy of Orthopaedic Surgeons Evidence-Based Medicine Committee (Beaton, Bombardier, Guillemin, & Ferraz, 2000). In the first step, the researcher and a teacher specializing in English independently translated the English version of the TSET into Chinese and further revised their translations through discussion and evaluation. In the second step, one American-English teacher who was familiar with Chinese and one nurse researcher who was proficient in English—neither of whom had seen the English version of the TSET—independently translated the Chinese version back into English. In the third step, the translators and researchers compared the accuracy of the two back-translated versions and the accuracy of the TSET items between the back-translated versions and original English version to detect differences. In the fourth step, the participating translators and researchers and the nursing and psychology experts formed a committee to assess the translation quality and content validity of the final TSET-CV. Finally, a group of 35 nurses discussed the presentation of the items to confirm that the most appropriate and commonly used Chinese expressions had been used in the texts and that they were comprehensible.
The final TSET-CV contains two parts. The first part is a demographic questionnaire, which collects information about gender, age, work experience, educational background, professional title, monthly income, work department, marital status, nationality, and employment type. The second part includes three subscales and 83 items in total. Likert-type response options ranging from 1 to 10 were used in this study (1 = no self-confidence, 10 = very confident). The Cognitive subscale (25 items) measures how cultural knowledge confidence may influence nursing care for clients with different cultural backgrounds. The Practical subscale (28 items) measures confidence in interviewing clients with different cultural backgrounds to learn their values and beliefs. The Affective subscale (30 items) measures the degree of confidence in identifying values, attitudes, and beliefs concerning cultural awareness, acceptance, appreciation, recognition, and advocacy. Factor analysis of TSET scores has supported the three-dimensional structure (Chen, Wang, & Peng, 2015; Halter et al., 2015; Jeffreys & Dogan, 2012).
Self-efficacy level (SEL) was calculated as follows: (a) low (nurses who selected a response of 1 or 2 on 80% or more of the subscale items); (b) high (nurses who selected a response of 9 or 10 on 80% or more of the subscale items); or (c) moderate (nurses who selected a response of 3–8 on 80% or more of the subscale items or who did not fall into the low or high group). Self-efficacy strength (SEST) refer to the average strength of self-efficacy perceptions within a particular dimension (subscale) of the construct. SEST scores on the Cognitive, Practical, and Affective subscales were calculated by totaling the subscale item responses and dividing the result by the number of subscale items, resulting in the mean score (Jeffreys, 2010a).
Data Collection
All of the investigators received the same training before the survey was conducted. Subsequently, the nurses were asked to independently and anonymously complete the questionnaires. The 30-minute long survey was conducted in a meeting room in the department where the nurses worked, and the answers were written on paper. The collected questionnaires were screened to exclude those with incomplete responses to the demographic items. All of the instruments could be completed within 30–40 minutes. The process of questionnaire collection lasted for two months. The collected questionnaires were inspected, and incomplete questionnaires were excluded.
The nurses who participated in the survey were all volunteers and were informed of the purpose and significance of the study by the research group members. Our study was reviewed and approved by the ethics committee at Chongqing Medical University and was approved by the Nursing Department and the Clinical Department at the three participating hospitals, including Guangdong Provincial People’s Hospital.
Data Analysis
SPSS version 22.0 software and Mplus7 were used for the statistical analysis. Frequencies were obtained for each SEL. Associations between nurse demographic characteristics and TSET scale and subscale scores were based on t-tests and F-tests. A nominal p-value of .05 was used. Reliability was estimated using Cronbach’s alpha. Confirmatory factor analysis with maximum likelihood estimation was used to assess dimensional structure. Three correlated factors were specified, with indicators linked to factors using the pattern for scoring TSET subscales. Root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), the Tucker–Lewis Index (TLI), and comparative fix index (CFI) were used to assess fit (Wen, Hau, & Marsh, 2004).
RESULTS
Sample Characteristics
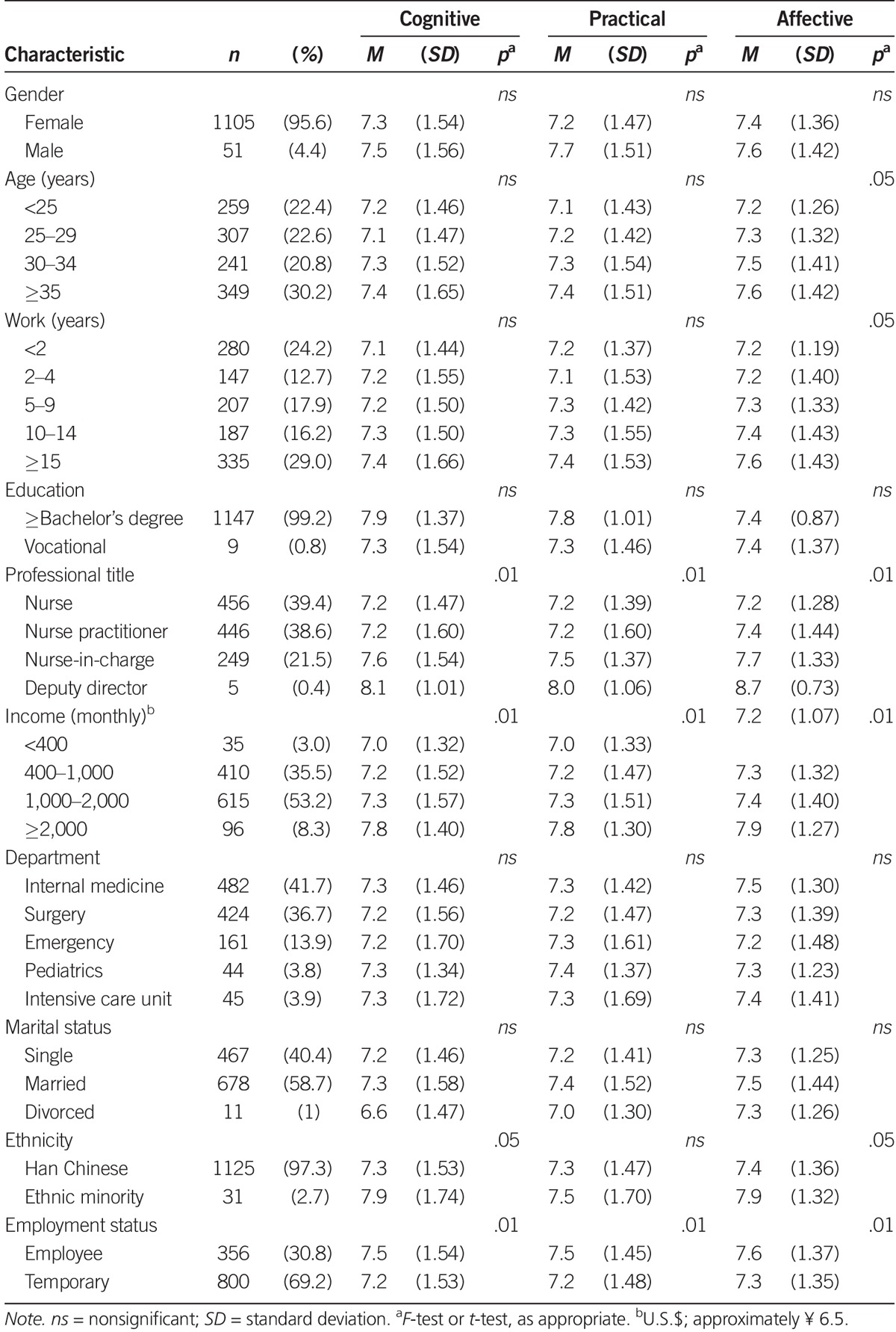
In total, 1,276 questionnaires were returned, and 1,156 (90.6%) questionnaires were complete. The demographic characteristics are presented in detail in Table 1. In brief, most participants were women with a fairly even age distribution (slightly more in the >35 years group), with work experience ranging from less than 2 years to more than 15 years. Almost all had college education or higher. Nurses and nurse practitioners were about equally represented and together accounted for about 80% of the sample. Likewise, nurses working in internal medicine or surgical nursing areas were about equally represented and accounted for almost 80% of the sample. Nurses with temporary employment status outnumbered those with official positions (n = 800, 69.2% vs. n = 356, 30.8%). Married nurses accounted for more than half of the study sample (n = 687, 58.7%). Almost all of the nurses were from the Han ethnic group (n = 1,125, 97.3%), and only 2.7% (n = 31) were from minority groups.
TABLE 1.
Participant Characteristics and Transcultural Self-Efficacy Tool Scores
Transcultural Self-Efficacy and Related Factors
Relationships between demographic characteristics and TSET-CV subscale scores are shown in Table 1. There was no significant difference in the scores of nurses with different genders, education status, or those from different departments, or marital statuses. There were significant differences in the scores of nurses in different age groups, those with different years of work experience, and those from different professional titles, incomes, ethnic groups, or employment types.
There were significant differences in the Affective subscale scores for nurses in different age groups. Post hoc tests results showed that nurses’ ages in the youngest age group (≤25 years) had significantly lower scores than the nurses’ ages of 30–34 years or >35 years.
Nurses with different years of work experience showed significant differences in Affective subscale scores. The post hoc results showed that nurses with less than 2 years of work experience had the lowest scores, and nurses with 15 years or more of work experience had significantly higher scores than other nurses.
Nurses with different professional job titles exhibited significant differences in all three subscales scores. The post hoc test results suggested that the deputy director nurses and nurses-in-charge had significantly higher scores compared with the nurse practitioners and nurses without titles. The nurses without titles had the lowest scores. The deputy director nurses had significantly higher scores compared with the nurses-in-charge.
Nurses with different incomes showed significant differences for all three subscale scores. The post hoc test results revealed that the nurses with monthly incomes higher than the equivalent of U.S.$2,000 had significantly higher scores on all three subscales than did the nurses with other income levels. Nurses with incomes lower than U.S.$400 had the lowest scores.
The Han nurses and minority nurses showed significantly different scores on the Cognitive and Affective subscales. The minority nurses had higher scores than the Han nurses.
Nurses with different employment types showed significant differences on all three subscales. The officially employed nurses had significantly higher scores than the temporary nurses did.
The above analyses indicates that nurses with the following characteristics had relatively lower transcultural self-efficacy: Those with less than 2 years of work experience or no title, who earned less than $400 a month, who were from the Han ethnic group, and who were temporary employed.
Transcultural Self-Efficacy Level
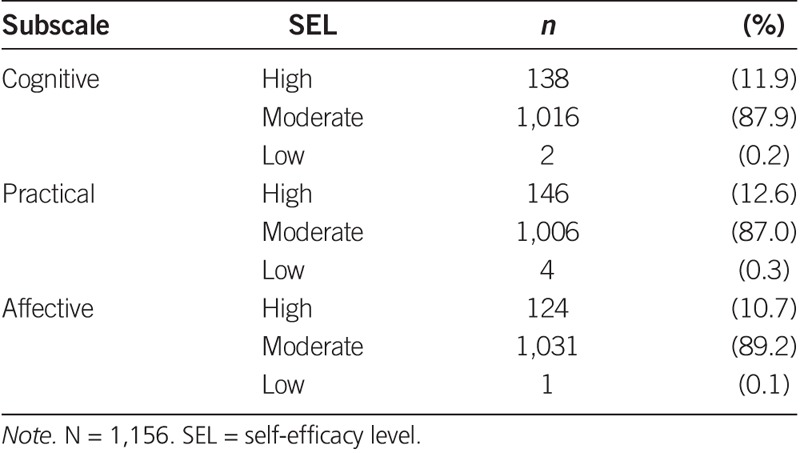
Table 2 shows the transcultural SEL for the Cognitive, Practical, and Affective subscales of the TSET-CV among the nurses working in general hospitals in Guangzhou, China. The data show that nurses with moderate SELs dominated the Cognitive (87.9%), Practical (87%), and Affective (89.2%) subscales. An average of 11.7% of the nurses had a high SEL (Cognitive: 11.9%, Practical: 12.6%, Affective: 10.7%). An average of 0.2% of nurses had a low SEL (Cognitive: 0.2%, Practical: 0.3%, Affective: 0.1%).
TABLE 2.
Perceived Self-Efficacy Level Distributions
Reliability and Validity
The overall Cronbach’s alpha was .99. Estimates of reliability using coefficient alpha for the Cognitive subscale, the Practical subscale, and the Affective subscale were .968, .979, and .968, respectively. Confirmatory factor analysis was conducted using the three-dimensional model with correlated factors established by Jeffreys and Dogan (2012). In this sample, CFI = 0.902, TLI = 0.907, RMSEA = 0.057, and SRMR = 0.049. The CFI and TLI were greater than the theoretical requirement of 0.9, the RMSEA was less than the theoretical requirement of 0.1, and the SRMR was less than the theoretical requirement of 0.08, indicating that fit was adequate (Wen et al., 2004) with good construct validity. Detailed information about specification, parameter estimates, and fit is available (see Figure, Supplemental Digital Content 1, http://links.lww.com/NRES/A187).
Discussion
Previous perceived transcultural self-efficacy studies have used nursing students as study subjects and the multinational immigrant culture as the background. Our study mainly focuses on nurses’ perceived self-efficacy when interacting with patients with multicultural differences. We found that nurses in general hospitals in Guangzhou have a moderate transcultural SEL. Older nurses—those with more years of work experience, higher professional titles, and higher incomes—and those from a minority background and who are officially employed have high perceived transcultural self-efficacy.
Most nurses had a middle-range SEL. In addition, nurses with a high SEL were rare, suggesting that the total confidence level of nurses when interacting with patients with cultural differences is not very high. This situation is likely related to the Chinese nursing education system. Chinese nursing education has historically focused excessively on basic medical education. No dedicated transcultural nursing classes are offered during nursing education. In-service continuing education at the hospital also fails to offer related information, leading to inadequate and insufficient transcultural nursing information (Zhang et al., 2010). In addition, Jimenez et al. (2006) reported that an important reason that nurses in the United States show a higher level of transcultural self-efficacy than Spanish nurses do is that transcultural nursing has been integrated into the curriculum of nursing education in the United States. One study found that transcultural nursing courses can improve the transcultural self-efficacy of nurses (Coffman et al., 2004). Therefore, we propose that China should offer transcultural nursing courses in nursing education programs, and hospitals should also offer training in transcultural nursing knowledge and skills in their continuing education programs for nurses.
Findings from other studies suggest that certain demographic variables can have significant effects on nurses’ perceived transcultural self-efficacy (Bernal & Froman, 1993; Joseph, 2004). For example, gender of nurses can influence their perceptions of transcultural self-efficacy (Joseph, 2004). However, the results of our study did not show gender differences in nurses’ perceived transcultural self-efficacy; we speculate that the hospital in Joseph’s (2004) study was a military hospital, and thus, special considerations were applied to that situation. Kim (2013) also compared the transcultural self-efficacy of nurses of different genders and found results consistent with our findings. We believe this may be because the participants in our study were similar to those in Kim’s (2013) study—and both studies had samples that included fewer than 5% of male nurses. The survey showed that the higher the education level of the nurses, the higher their self-efficacy scores (Kim, 2013). Our results may have shown no differences in transcultural self-efficacy among nurses with different education levels because transcultural nursing education is neglected in all levels of nursing education in China. Therefore, there are unlikely to be any education-related difference in transcultural self-efficacy strength among nurses.
The TSET-CV score results revealed that the nurses of <25 years of age had the lowest subscale scores, and nurses of >35 years of age had the highest scores. This result is consistent with Molinari and Monserud’s (2009) study, which suggests that older nurses have better transcultural perceived self-efficacy. The nurses who have worked for 15 years or longer had significantly higher scores compared with other nurses; moreover, the greater their total years of work experience, the higher their SEST scores. China has a large population and a sizeable patient population. In the general hospitals that were surveyed in this study, the average number of outpatients is approximately 10,000 and the average number of hospitalized patients is more than 3,000 every day. This unique medical situation in China has enabled nurses to accumulate a wealth of work experience. Studies have shown that clinical experience can give nurses more confidence to care for patients with cultural differences (Cortis, 2003; Sarafis & Malliarou, 2013). It can be speculated that nurses with more years of work experience will accumulate more clinical nursing experience and will, therefore, show more confidence when interacting with patients from different cultures.
The Chinese system of nursing professional titles is a unique human resources management system. A nurse’s professional title is a comprehensive reflection of education, professional theoretical and technical skills, research ability, and other factors. The professional titles are ranked into five levels: nurse director, deputy nurse director, nurse-in-charge, nurse practitioner, and nurse (Xu, 2008). Nurses with advanced professional titles generally have higher education levels, better professional skills, and stronger research and clinical comprehensive abilities. There are limited numbers of nurse directors in Chinese hospitals. They are mainly in charge of education and management and rarely work in clinics. Therefore, there were no nurse directors in our samples. Our survey results showed that the deputy nurse directors and nurses-in-charge both had significantly higher scores than the nurse practitioners and nurses with no title; the deputy director nurses had significantly higher scores than the nurses-in-charge. Our results are consistent with the expectations for cultural competence, which indicates that attitudes, knowledge, and skills are essential capabilities for nurses to provide quality care for patients with cultural differences (Giger et al., 2007). Therefore, it can be hypothesized that a nurse’s comprehensive experience, such as education, professional skill level, and clinical experience, can increase her or his confidence when interacting with patients from different cultures. In addition, the nurses with higher incomes had higher scores, and the differences were significant differences for all three subscales. A deep-seated reason for this relationship that the income of nurses at general hospitals in China is associated with their professional title; a nurse’s salary depends on title, and the higher her title, the higher the salary. Nurses with advanced titles will have higher incomes. Therefore, it is only an illusion that a higher income leads to higher self-efficacy.
The ethnic minority nurses all had higher scores on TSET-CV subscales than the Han nurses, and there was a significant difference for two subscales. With the reform of China’s higher education system and population policy, an increasing number of minority college students come to urban colleges from their remote native lands to receive higher education. However, culture influences the human psychological structure, and ethnic minority college students are influenced by many aspects, including their histories and cultures, geographical environments, religion, customs, and lifestyles. The process by which they accept the Han culture is not one of assimilation into Han culture, but “dual process of acceptance and dissention.” As minority students, they are attempting to blend into the mainstream culture dominated by the Han culture; however, they inwardly struggle to remain within their cultures (Fei, 1989; Jiang, 2010). Joseph (2004) also reported that a minority nurse group had higher perceived transcultural self-efficacy than a nonminority nurse group. Our study results also showed that nurses with a minority cultural background had higher confidence than Han nurses when interacting with patients from different cultures.
Officially employed nurses refer to nurses who are directly employed by and sign contracts with hospitals. Temporary nurses refer to nonofficially employed nurses who sign contracts with a third party and are sent to work in the hospital. Officially employed nurses had significantly higher scores than temporary nurses. Compared with temporary nurses, official employees have priority access to the hospital’s reeducation, professional development, and job promotion opportunities; they also have little or no risk of being dismissed and have a relatively stable working environment. According to Bandura’s (1986) theory, perceived self-efficacy plays an important role in self-regulation of the emotional state. When individuals face pressure or a threatening environment emotional impact, the perceived nonefficacy can induce negative emotions, such as anxiety, fear, and depression. These negative emotions further weaken the individual’s behavioral enthusiasm and disturb the normal exertion of multiple psychological functions. In contrast, a high perceived self-efficacy can result in a positive emotional experience, such as confidence (Bandura, 1986). Officially employed nurses are more confident than temporary nurses when communicating with patients from different cultures; this finding suggests that a stable work environment and promising career development opportunities are beneficial perceived transcultural self-efficacy in nurses.
Unlike nursing students in schools, nurses have only one option for improving their clinical transcultural ability and perceived transcultural self-efficacy, namely, through in-service continuing education. Nurses in Chinese hospitals have no opportunity for transcultural education when they are students, and therefore, their overall transcultural SEL is not high. Hospital nursing management should intervene by offering continuing education on transcultural nursing appropriate to the demographic characteristics of the nurses to make up for the missed education to some extent, so that nurses can provide high-quality transcultural nursing to patients for decades of working life to come. The results also inspired suggestions for China’s nursing education programs; transcultural nursing courses should be included in nursing education programs, and these courses should be taught 1 year before graduation to help student nurses better learn and master transcultural nursing skills during practical training and, thus, have a higher level of transcultural nursing self-efficacy and capability when they become nurses.
Conclusion
Overall levels of perceived transcultural self-efficacy were not high among Chinese nurses in Guangzhou. Transcultural self-efficacy was higher among nurses who were older; those who had more years of work experience, higher professional titles, higher incomes, a minority background; and those who were officially employed. Nursing management in hospitals should offer continuing education on transcultural nursing. Doing so will compensate for the transcultural nursing education Chinese nurses miss as students and enable them to provide quality nursing to the increasing number of patients from different cultures.
Supplementary Material
Figure.
No caption available.
Footnotes
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.nursingresearchonline.com).
The authors would like express their deepest gratitude to Professor Marianne Jeffreys and to the Springer Publishing Company for providing the Transcultural Self-Efficacy Tool and technical support. This study has no conflicts of interest with other papers, studies, authors, and publishers.
The authors have no conflicts of interest to report.
REFERENCES
- *URLs for select references from the Chinese literature are available as Document, Supplemental Digital Content 2, http://links.lww.com/NRES/A188
- Bandura A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice Hall. [Google Scholar]
- Beaton D. E., Bombardier C., Guillemin F., & Ferraz M. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine, 25, 3186–3191. doi:10.1097/00007632-200012150-00014 [DOI] [PubMed] [Google Scholar]
- Bernal H., & Froman R. (1993). Influences on the cultural self-efficacy of community health nurses. Journal of Transcultural Nursing, 4, 24–31. doi:10.1177/104365969300400205 [DOI] [PubMed] [Google Scholar]
- Berry J. W., & Sabatier C. (2010). Acculturation, discrimination, and adaptation among second generation immigrant youth in Montreal and Paris. International Journal of Intercultural Relations, 34, 191–207. doi:10.1016/j.ijintrel.2009.11.007 [Google Scholar]
- Calvillo E., Clark L., Ballantyne J. E., Pacquiao D., Purnell L. D., & Villarruel A. M. (2009). Cultural competency in baccalaureate nursing education. Journal of Transcultural Nursing, 20, 137–145. doi:10.1177/1043659608330354 [DOI] [PubMed] [Google Scholar]
- Chen J., Wang Y., & Peng Y. (2015). [Revision of transcultural self-efficacy tool (Chinese version)]. Chinese Nursing Research, 29, 1811–1814. [Google Scholar]
- Coffman M. J., Shellman J., & Bernal H. (2004). An integrative review of American nurses’ perceived cultural self-efficacy. Journal of Nursing Scholarship, 36, 180–185. doi:10.1111/j.1547-5069 .2004.04032.x [DOI] [PubMed] [Google Scholar]
- Cortis J. D. (2003). Culture, values and racism: Application to nursing. International Nursing Review, 50, 55–64. doi:10.1046/j.1466-7657.2003.00152.x [DOI] [PubMed] [Google Scholar]
- Cronin S. N., & Harrison B. (1988). Importance of nurse caring behaviors as perceived by patients after myocardial infarction. Heart & Lung, 17, 374–380. [PubMed] [Google Scholar]
- Davidhizar R., & Giger J. N. (2004). A review of the literature on care of clients in pain who are culturally diverse. International Nursing Review, 51, 47–55. doi:10.1111/j.1466-7657.2003.00208.x [DOI] [PubMed] [Google Scholar]
- Dawson L., & Lighthouse S. (2010). Assessment of self-efficacy for cultural competence in prescribing. Journal for Nurse Practitioners, 6, 44–48. doi:10.1016/j.nurpra.2009.02.012 [Google Scholar]
- Fei X. (1989). [The multinational unified pattern of the Chinese nation]. Beijing, China: Central Institute for Nationalities.* [Google Scholar]
- Geissler E. M. (1992). Nursing diagnoses: A study of cultural relevance. Journal of Professional Nursing, 8, 301–307. doi:10.1016/8755-7223(92)90057-6 [DOI] [PubMed] [Google Scholar]
- Giger J., Davidhizar R. E., Purnell L., Harden J. T., Phillips J., Strickland O., … American Academy of Nursing (2007). American Academy of Nursing Expert Panel report: Developing cultural competence to eliminate health disparities in ethnic minorities and other vulnerable populations. Journal of Transcultural Nursing, 18, 95–102. doi:10.1177/1043659606298618 [DOI] [PubMed] [Google Scholar]
- Halter M., Grund F., Fridline M., See S., Young L., & Reece C. (2015). Transcultural self-efficacy perceptions of baccalaureate nursing students. Journal of Transcultural Nursing, 26, 327–335. doi:10.1177/1043659614526253 [DOI] [PubMed] [Google Scholar]
- Jeffreys M. R. (2010a). Teaching cultural competence in nursing and health care (2nd ed.). New York, NY: Springer Verlag. [Google Scholar]
- Jeffreys M. R. (2010b). The cultural competence education resource toolkit. New York, NY: Springer. [Google Scholar]
- Jeffreys M. R., & Dogan E. (2010). Factor analysis of the transcultural self-efficacy tool (TSET). Journal of Nursing Measurement, 18, 120–139. doi:10.1891/1061-3749.18.2.120 [DOI] [PubMed] [Google Scholar]
- Jeffreys M. R., & Dogan E. (2012). Evaluating the influence of cultural competence education on students’ transcultural self-efficacy perceptions. Journal of Transcultural Nursing, 23, 188–197. doi:10.1177/1043659611423836 [DOI] [PubMed] [Google Scholar]
- Jeffreys M. R., & Smodlaka I. (1999). Construct validation of the transcultural self-efficacy tool. Journal of Nursing Education, 38, 222–227. [DOI] [PubMed] [Google Scholar]
- Jiang H. (2013). [The resource allocation and operating mechanism of Guangzhou’s public hospitals] (Unpublished master’s thesis). Jinan University, Guangzhou, China.* [Google Scholar]
- Jiang M. (2010). [Aspects of ethnic minority medical students’ psychological adjustment from the perspective of mainstream culture]. Guizhou Ethnic Studies, 6, 170–175. doi:10.13965/j.cnki.gzmzyj10026959.2010.06.013 [Google Scholar]
- Jimenez J. A., Contreras J. L., Shellman J., Gonzalez M. L., & Bernal H. (2006). The level of cultural self-efficacy among a sample of Spanish nurses in Southeastern Spain. Journal of Transcultural Nursing, 17, 164–170. doi:10.1177/1043659605285417 [DOI] [PubMed] [Google Scholar]
- Joseph H. J. (2004). Attitudes and cultural self-efficacy levels of nurses caring for patients in army hospitals. Journal of the National Black Nurses Association, 15, 5–16. [PubMed] [Google Scholar]
- Kim S. H. (2013). [Transcultural self-efficacy and educational needs for cultural competence in nursing of Korean nurses] (Article in Korean). Journal of Korean Academy of Nursing, 43, 102–113. doi:10.4040/jkan.2013.43.1.102 [DOI] [PubMed] [Google Scholar]
- Leininger M. M. (1991). Cultural care, diversity, and universality: A theory of nursing. New York, NY: National League of Nursing. [PubMed] [Google Scholar]
- Li N. (2013). [Construction of the image of new immigrants by urban mainstream media] (Unpublished master’s thesis). Guangzhou University, Guangzhou, China. Retrieved from http://www.cnki.net/KCMS/detail/detail.aspx?FileName=1014111204.nh&DbName=CMFD2014 [Google Scholar]
- Li Q. (2013). [Study of urban management of foreign population—Using Guangzhou as an example]. City Watch, 3, 138–147.* [Google Scholar]
- Li T. Y. (2012). [Study of the existence value and development prospects of Cantonese in television media] (Unpublished master’s thesis). Jinan University, Guangzhou, China. Retrieved from http://www.cnki.net/KCMS/detail/detail.aspx?FileName=1012031246.nh&DbName=CMFD2012 [Google Scholar]
- Molinari D. L., & Monserud M. (2009). Rural nurse cultural self-efficacy and job satisfaction. Journal of Transcultural Nursing, 20, 211–218. doi:10.1177/1043659608330350 [DOI] [PubMed] [Google Scholar]
- National Bureau of Statistics of China. (2011). The 6th national population census. Retrieved from http://www.stats.gov.cn
- Qian W. (2010). [Comparison of the differences between Mandarin and Cantonese]. Journal of Language and Literature Studies, 6, 1–3.* [Google Scholar]
- Rooda L. A. (1993). Knowledge and attitudes of nurses toward culturally different patients: Implications for nursing education. Journal of Nursing Education, 32, 209–213. [DOI] [PubMed] [Google Scholar]
- Sarafis P. A., & Malliarou M. M. (2013). Cultural self-efficacy of baccalaureate nursing students in a Greek University. Iranian Journal of Nursing and Midwifery Research, 18, 446–450. [PMC free article] [PubMed] [Google Scholar]
- Wang J., Wang W., Cheng S., & Gao K. (2013). [China doctor–patient relationship crisis management system research in China]. Medicine and Society, 3, 20–22. doi: 10.3870/YXYSH.2013.03.007.* [Google Scholar]
- Wen Z. L., Hau K. T., & Marsh H. W. (2004). [Structural equation model testing: Cutoff criteria for goodness of fit indices and chi-square test]. Acta Psychologica Sinica, 36, 186–194.* [Google Scholar]
- Xiao H. (2010). [Language and culture “conflict” analysis in social context—Using “promoting Mandarin” versus “defending Cantonese” as an example]. Fujian Tribune (The Humanities & Social Sciences Monthly), 12, 197–199.* [Google Scholar]
- Xing Z., & Li A. (2011). [Construction of urban ethnic cultural infusion and a happy society—Using Guangzhou as an example]. Journal of Guangdong University of Foreign Studies, 2011(4), 66–70.* [Google Scholar]
- Xu Z. J. (2008). [Study on the establishment of a hierarchical classification management system for Shanghai caregivers] (Unpublished master’s thesis). Fudan University, Shanghai, China.* [Google Scholar]
- Zhang X. L., Peng Y. Q., Yu H. P., & Xu L. (2010). [Educational advancement of multicultural nursing in China]. Chinese General Practice, 13, 133–135.* [Google Scholar]
- Zhou C. L. (2014). [Brief discussions on contemporary social mainstream culture and subculture in China]. Education Teaching Forum, 20, 163–164.* [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.