
Figure 5. Factors that influence fetal anaerobic reserve and fetal oxygen debt during labour .
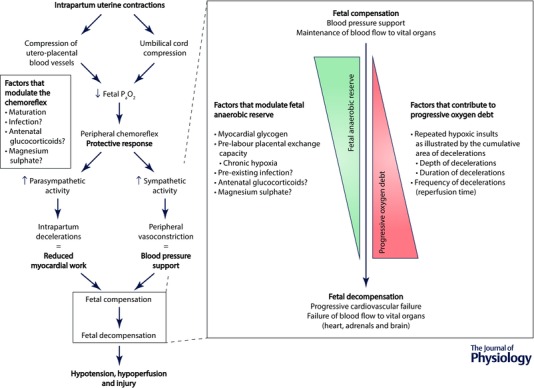
Periods of brief asphyxia are frequent and a normal component of labour. This is offset by the fetus’ ability to adapt to these challenges through peripheral chemoreflex activation and a high anaerobic tolerance. Thus, the vast majority of fetuses adapt effectively to labour and are born healthy. The ability to adapt is finite, however, and can fail in two situations. Firstly, a fetus with good antepartum health and adequate anaerobic reserves can progressively decompensate if exposed to severe repeated asphyxial challenges that are too frequent to allow complete recovery between intense uterine contractions. Secondly, and perhaps of more clinical importance, is the scenario of a fetus entering labour with poor utero‐placental exchange capacity and reduced glycogen reserves. Such fetuses are unable to fully compensate to the repeated asphyxial challenges of a typical labour and will quickly decompensate, leading to hypotension and increasing risk of neural injury.