
Fig. 2.
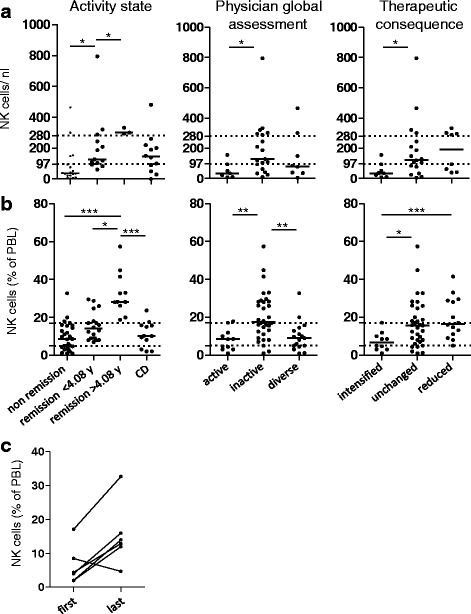
Natural killer (NK) cells inversely correlate with granulomatosis with polyangiitis (GPA) activity. Patients from cohort I and II were included; cohort I has been published in a parent study [15]; cohort II is described in Table 1. a Absolute NK cell numbers are decreased in active GPA. Cohort I, n = 12; cohort II, n = 22; total = 34; control disease (CD), n = 12 patients with inactive systemic inflammatory control diseases (see [15] and Table 1). Dotted lines show upper and lower limits of normal NK cell numbers according to our clinical diagnostic laboratory; medians are indicated by bars. Left subgrouping according to activity states showed significant differences among the groups (Kruskal-Wallis test, p = 0.0029); middle physician global assessment (Kruskal-Wallis test, p = 0.0486); right therapeutic consequence (Kruskal-Wallis test, p = 0.0397). b NK cell percentages are increased in patients with GPA in long-term remission. Cohort I, n = 35; cohort II, n = 22; total = 57; CD, n = 12. Dotted lines correspond to the upper and lower limits of normal NK cell percentages, according to our clinical diagnostic laboratory; medians are indicated by bars. Left subgrouping according to activity states showed significant differences among the groups (Kruskal-Wallis test, p = 0.0001); middle physician global assessment (Kruskal-Wallis test, p = 0.0007); right therapeutic consequence (Kruskal-Wallis test, p = 0.0108). a, b The threshold for long-term remission (4.08 years) had been determined in the parent study [15]. Dunn's post hoc test was significant where indicated in the graphs. c NK cells increase during successful induction therapy. NK cell percentages from six patients with GPA were determined at two or more time points during induction therapy (cohort I, four patients; cohort II, two patients). The first and last measurements are depicted, respectively. Statistical analysis was performed using the Wilcoxon signed rank test, p = 0.0585