
Fig. 9.
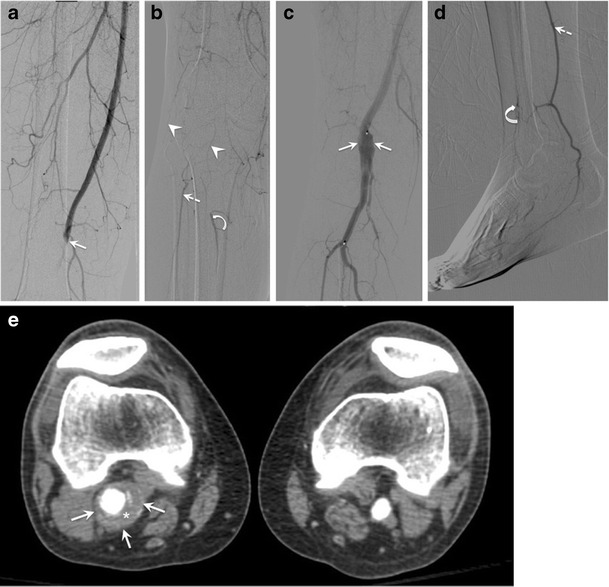
Popliteal artery aneurysm (PAA) in a 52-year-old man admitted for cold right foot. (a, b) Digital subtraction angiography on admission shows abrupt occlusion of the proximal popliteal artery at the level of the adductor hiatus (solid arrow), with minimal collateral vessels around the knee (arrowheads), suggesting acute thrombosis. Distally, there is revascularization of the peroneal (dashed arrow) and anterior tibial (curved arrow) arteries. Patient underwent intravascular catheter-directed thrombolysis, and lytic check at 12 h (not shown) showed incomplete lysis of the thrombus. Patient was continued on the same treatment. (c, d) Digital subtraction angiography at 22 h post-lysis reveals a large PAA (solid arrows), with re-permeabilization of the posterior tibial artery (dashed arrows). However, the distal anterior tibial artery is barely opacified, suggesting vascular changes from chronic distal embolization resulting in tissue loss. (e) Axial CT angiography shows a larger PAA than expected from angiography images (solid arrows), with mural thrombus (asterisk). These findings characterize classical acute (acute thrombosis) and chronic (loss of distal run-off from repeated distal embolization) complications from PAA