

Abstract
Background: Congenital diaphragmatic hernia (CDH) is a simple diaphragmatic defect that is seen frequently in antenatal scans. Though the surgical repair is relatively easy in the neonate, the mortality is high due to pulmonary hypoplasia and pulmonary vascular changes.
Materials and Methods: The goals of prenatal imaging are to establish the diagnosis. Assessment in a tertiary scanning center would identify prognostic factors which assist in counselling and planning antenatal management. However, the pulmonary hypoplasia associated with the CDH in moderate and severe cases makes the prognosis poor.
Conclusions: Fetal intervention such as, fetal tracheal occlusion, is being trialled and may change the outcomes in the future.
Keywords: congenital diaphragmatic hernia, fetal intervention, fetal MRI, FETO, ultrasound scan
Introduction
Congenital diaphragmatic hernia (CDH) is the consequence of a defect in the development of the diaphragm.
The defect allows the abdominal contents to herniate into the thoracic cavity. The incidence is approximately 2–4 per 10,000 live births, 1 making it one of the more common birth anomalies.
CDH is associated with high mortality but with improvement in detection and perinatal management the overall survival rates are now up to 70%. 2 – 4
With the introduction of minimally invasive fetal intervention the survival of fetuses with CDH is likely to improve further.
Pathogenesis
The development of the diaphragm occurs before 10 weeks gestation and separates the pleuro‐peritoneal canal with a pleuro‐peritoneal membrane to form the diaphragm. Two lateral segments (left and right) and a central segment coalesce together to form the diaphragm. When the fusion is not complete a diaphragmatic hernia results.
The abdominal contents herniate into the thoracic cavity and compress the lungs and often cause a shift of the mediastinum.
The herniation coincides with the critical period of lung development when bronchial branching and pulmonary artery development occurs. The consequence is a marked reduction in terminal bronchioles, thickened alveolar septae, reduced alveolar volume and increased arterial medial wall thickness. 5 – 8 This results in fixed increased vascular resistance and reduced surface area for gas exchange 9 with resultant lung compression causing pulmonary hypoplasia. Therefore, the postnatal compromise is the result of the fixed pulmonary and vascular hypoplasia, and reversible, pulmonary vascular reactivity. This results in respiratory failure and persistent fetal circulation. These features are the main determinants of neonatal survival.
The diaphragmatic defect occurs on the left side in up to 90%, on the right side in 10% 10 and rarely, bilaterally 11 Approximately 70% of defects involve the posterolateral (Bochdalek) region of the diaphragm, with anterior (Morgagni) involvement in 25–30%. 12 , 13 Central regions are rarely affected (Figure 1).
Figure 1.
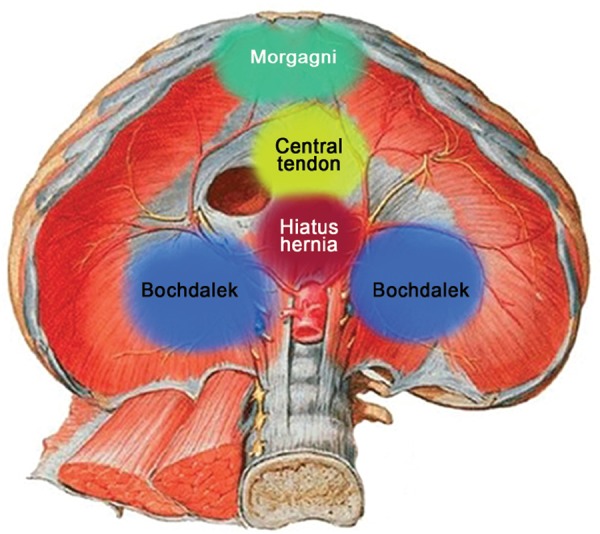
Schematic representation of anterior (Morgagni), posterolateral (left and right Bochdalek) and central diaphragmatic hernia.
Figure 2a.
Normal four chamber axial view of the heart.
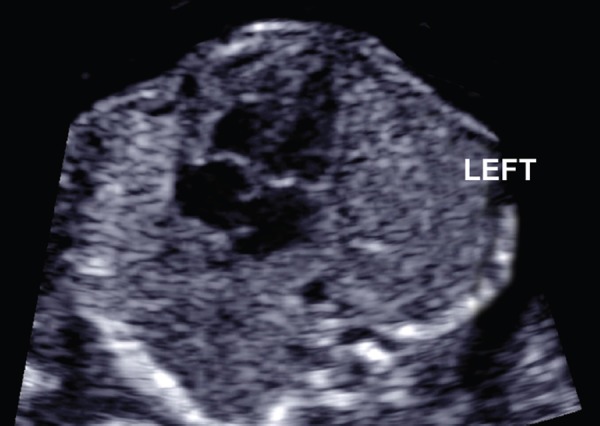
Figure 2b.

Left sided CDH showing stomach and liver in the four chamber view and mediastinal shift of the heart to the right side.
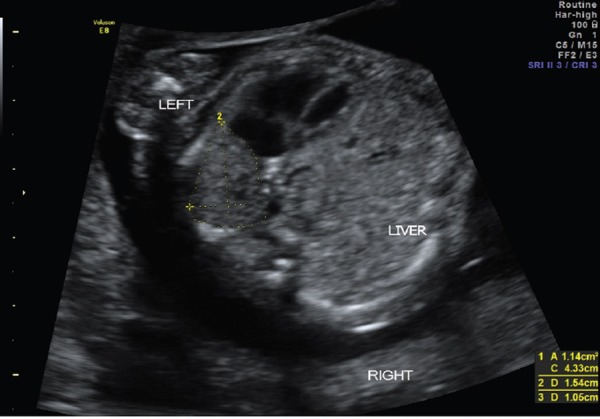
Figure 3.

Coronal view of the abdomen and thorax showing the stomach within the thoracic cavity.
Imaging and prognostic features
The goal of prenatal imaging is to establish the diagnosis. In addition, assessment in a tertiary scanning center would identify prognostic factors which assist in counseling and planning antenatal management. The use of ultrasound for the diagnosis and prognostication of CDH is well established. 14 – 16 Despite this, it can be difficult to diagnose CDH before 24 weeks. 13 Nearly 11% of cases are missed during the antenatal period and diagnosed postnatally. 17
The diagnosis primarily relies on the visualisation of abdominal organs, usually the stomach, within the fetal chest. In a left‐sided CDH the fluid‐filled stomach is seen just behind the left atrium and left ventricle in the lower thorax in an axial four chamber view of the heart.
Indirect features include mediastinal shift and a small abdominal circumference. Non‐visualisation of the stomach within the abdominal cavity supports the diagnosis, although it is not a specific sign. Peristalsis of the viscera maybe seen within the thoracic cavity.
Right‐sided diaphragmatic hernias are less common than their left‐sided counterparts. They are frequently missed as the herniated liver can have a similar echo texture as the lung or a misdiagnosis of a solid mass in the chest. 18 Useful tips to aid diagnosis include Doppler examination to confirm the course of the hepatic vasculature and umbilical vein which may show an elongation of the intra‐abdominal portion of umbilical vein or an abnormal position and bowing of the portal sinus. The portal and hepatic venous branches maybe seen above the diaphragmatic ridge. A cross‐sectional view may show a mid‐thoracic or posterior‐thoracic position of stomach with tissue visualised anteriorly between the stomach and the heart (Figures 4a and b).
Figure 4a.

Right‐sided CDH with the echotexture of the herniated liver similar to the echotexture of the lung.
Figure 4b.
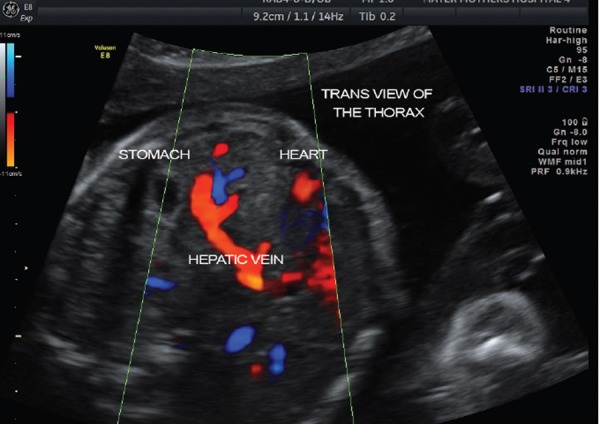
CDH with the hepatic vein seen within the thoracic cavity.
Ultrasound assessment is the current modality for predicting neonatal survival. The observed/expected lung‐to‐head ratio (O/E LHR) is a validated method of assessing lung size. 14 The O/E LHR is a predictor of survival and short term morbidity performed from 22–24 weeks GA, with better prediction when measured between 32–33 weeks gestation. 5 , 19
The technique measures the contralateral lung area and it is related to the fetal head circumference in the lung‐to‐head ratio. These measurements are then compared with the expected ratio for gestational age in the observed‐expected lung‐head ratio. 16
There is a lack of consensus regarding the technique and the effectiveness of lung volume measurement. All techniques measure the visualised lung on the axial plane at the level of the four‐chamber‐view (Figure 5)
Figure 5.
Antero‐posterior and tracing methods to estimate lung volume.
A recent editorial by Jani, Peralta and Nicolaides, has highlighted the need to standardise the technique for LHR and reviews the ideal method that should be adopted. 20 Of all the methods the tracing method is the most reproducible. 16
The O/E LHR does have its limitations. The learning curve is steep with a minimum of 70 cases required to achieve competence. 21 Practically, this restricts this technique to the specialised tertiary centers that will be managing the perinatal management of a baby with CDH.
The predictive value of O/E LHR is thought to rely on the postnatal care and survival data for a given centre 22 and will hence become less predictive with alterations in management. The O/E LHR technique gives information about the amount of lung available but it does not predict the status of the pulmonary vascular bed and eventual gas exchange at the alveoli. Pulmonary branch measurements and Doppler studies of pulmonary vascular flow and reactivity have yet to find a place in the routine evaluation of CDH 23 – 25 or in the prediction of pulmonary hypertension. 10
The laterality of the diaphragmatic defect is not an independent predictor of postnatal survival at discharge from hospital. 26 Right‐sided CDH has a poorer outcome 4 , 14 , 27 primarily due to the liver herniation into the chest. Liver herniation is an independent predictor of mortality in CDH. 15 , 22 , 26 , 28 , 29 A left‐sided CDH with liver up, is indicative of an early, large defect. 22 Overall mortality is poorer with up to 55% mortality with liver‐up, compared to 6–26% mortality with liver‐down. 15 , 29
Extracorporeal membrane oxygenation (ECMO) requirement is more likely with liver herniation. 4 , 29
Specialised centers may offer fetal magnetic resonance imaging (MRI) as an assessment of lung volumes (Figure 6). MRI has recently been established as an adjunct to ultrasound in not only the diagnosis of CDH but also to aid the estimation of lung volume. 27 , 29 MRI can provide clarity in cases where ultrasound imaging has been sub optimal and can increase detection of liver herniation. 27
Figure 6.
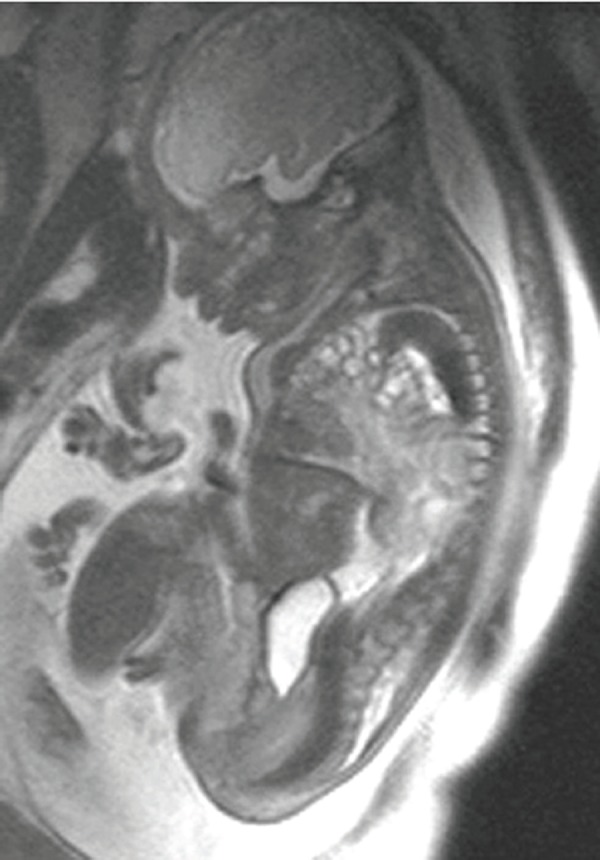
Fetal MRI showing CDH. Bowel is seen within fetal thorax.
Figure 7.
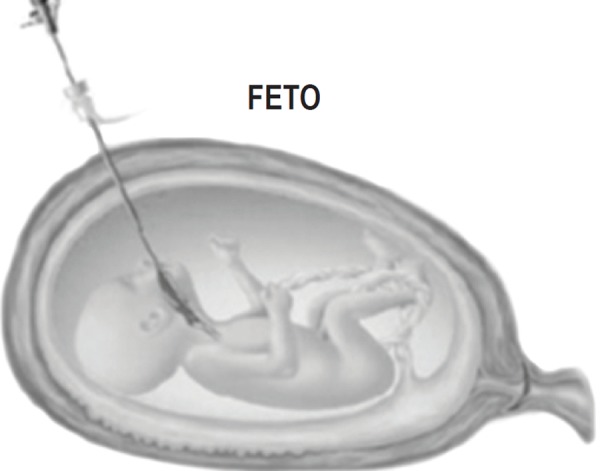
Schematic diagram showing the fetal endoscopic tracheal occlusion (FETO).
MRI fetal lung volume ratio has shown to be the more accurate method of prediction of survival in cases of left 29 and right CDH. 30 Observed/expected total lung volume as detected by MRI has shown to be a better independent predictor of postnatal survival to discharge in comparison with 2D ultrasound. 27
Differential diagnosis and associated anomalies
The main differential diagnoses include intrathoracic lesions such as bronchopulmonary sequestration, congenital cystic adenomatoid malformation, bronchogenic cysts, and enteric cysts. Diaphragmatic eventration is characterised by a deficiency of muscle fibres in all or part of the diaphragm. The deficient areas are replaced by fibrous tissue with a resultant elevation of the dome of the diaphragm. This maybe difficult to differentiate from CDH and an MRI may establish the diagnosis. 31
An isolated CDH carries a relatively more favorable prognosis than a non‐isolated CDH. It is essential to rule out associated structural anomalies. Associated anomalies can include, in descending order, cardiac, renal, central nervous and gastrointestinal systems. 32 , 33 Bilateral CDH is usually associated with multiple anomalies. 11 , 34 Survival of fetuses with associated malformations is approximately 30%. 35
Genetic and non‐genetic syndromes are also associated with CDH. Amniocentesis to diagnose associated genetic anomalies is recommended. 5 Three to 30% of cases will have an associated chromosomal anomaly, with a resultant poorer prognosis. 13 , 36 Chromosomal abnormalities include trisomy 18, tetrasomy, or complex structural abnormalities such as 12q, 4p and 8p deletions. 13 , 35 Genetic syndromes include Smith‐Lemi‐Opitz, CHARGE, Golderhar, Beckwith‐Widemann and Noonan Syndrome. 13
Predicting prognosis
Prenatal prediction of prognosis relies on a number of variables. These include the type of CDH, unilateral or bilateral, isolated or associated with other anomalies and if part of a genetic syndrome. The modalities of investigations include high‐resolution ultrasound in a tertiary center, fetal MRI when indicated, fetal echocardiography and prenatal karyotype. Recent studies appear to indicate some benefit in improved survival of severe cases with fetal intervention. The presence of an experienced neonatology and pediatric surgical team with tertiary level support services with established protocols improves survival.
Future therapy
Fetal Endoscopic Tracheal Occlusion (FETO) is a minimally invasive fetoscopic procedure whereby a balloon is inserted into the fetal trachea with the purpose of blocking the trachea to allow the lungs to expand with the lung secretions. This is currently being used in some expert centres under a trial setting to determine whether this technique will reduce neonatal mortality/morbidity in severe CDH cases secondary to pulmonary hypoplasia.
In 2009, the Eurofetus group reported the results of a cohort of 210 cases with severe CDH who had FETO. 26 Median age at delivery was 35 weeks with a 47% survival to discharge, compared with an estimated 20% survival if untreated. Ruano, et al. followed with a randomised controlled trial (RCT) with FETO in severe cases of CDH. There were 19 cases in each arm. The median age at delivery was 35.4 weeks in the treatment group compared with 37.5 weeks in the control group. Survival at 6 months was 52.6% in the FETO group compared with 5.3% in the control group, i.e. a 10‐fold survival rate.
However, despite these promising studies, these results need to be interpreted with caution. Numbers in RCTs are small. Complications are significant and can include up to a 47% chance of premature rupture of membranes 26 and pre‐term delivery. In addition, the balloon has to be removed before planned delivery or will need to be removed as an emergency procedure at birth. The International Multicentre randomised controlled trial “TOTAL” (Tracheal Occlusion To Accelerate Lung growth) led by the Eurofetus group is currently recruiting women. Until further studies can consolidate the role of FETO in the management of CDH, this procedure is limited to specialised fetal surgery centres under trial conditions.
Summary
CDH is a fetal abnormality that is seen frequently in tertiary centres. The treatment for CDH is an uncomplicated postnatal surgery. However, the pulmonary hypoplasia associated with the CDH in moderate and severe cases makes the prognosis poor. Antenatal assessment at a tertiary centre with fetal intervention when indicated could change the outcomes in the near future.
Acknowledgements
This paper is based upon a presentation by Dr Thomas given at the ASUM MDW, Adelaide March 2012. We are grateful to the inputs from Dr Glenn Gardener, Director Maternal Fetal Medicine, Mater Centre for Maternal Fetal Medicine, Brisbane and Dr Scott Petersen, Staff Specialist, Mater Centre for Maternal Fetal Medicine, Brisbane. We would like to acknowledge Mohit Thomas for helping us with the graphics.
References
- 1. Stevenson R, Hall G. Human Malformations and Related Anomalies, ed 2 Oxford University Press; 2006. pp 14‐217. [Google Scholar]
- 2. Seetharamaiah R, Younger JG, Bartlett RH, Hirschl RB, and the Congenital Diaphragmatic Hernia Study Group . Factors associated with survival in infants with congenital diaphragmatic hernia requiring extracorporeal membrane oxygenation: a report from the Congenital Diaphragmatic Hernia Study Group. J Pediatr Surg 2009; 44: 1315–21. [DOI] [PubMed] [Google Scholar]
- 3. Brownlee EM, Howatson AG, Davis CF, Sabharwal AJ. The hidden mortality of congenital diaphragmatic hernia: a 20 year review. J Pediatr Surg 2009; 44: 317–20. [DOI] [PubMed] [Google Scholar]
- 4. Hedrick HL, Danzer E, Merchant A, Bebbington MW, Zhao H, Flake AW, et al. Liver position and lung‐to‐head ratio for prediction of extracorporeal membrane oxygenation and survival in isolated left congenital diaphragmatic hernia. Am J Obstet Gynecol 2007; 197: 422. e1–4. [DOI] [PubMed] [Google Scholar]
- 5. Kotecha S, Barbato A, Bush A, Claus F, Davenport M, Delacourt C, et al. Congenital Diaphragmatic Hernia. Eur Respir J 2012; 39: 820–29. [DOI] [PubMed] [Google Scholar]
- 6. Areechon W, Reid L. Hypoplasia of lung in congenital diaphragmatic hernia. BMJ 1963; 1: 230–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Kitagawa M, Hislop A, Boyden EA, Reid L. Lung hypoplasia in congenital diaphragmatic hernia. A quantitative study of airway, artery and alveolar development. Br J Surg 1971; 58: 342–46. [DOI] [PubMed] [Google Scholar]
- 8. Wigglesworth JS, Desai R, Guerrini P. Fetal lung hypoplasia: biochemical and structural variations and their possible significance. Arch Dis Child 1981; 56: 606–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Hislop A, Reid L. Persistent hypoplasia of the lung after repair of congenital diaphragmatic hernia. Thorax 1976; 31: 450–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Deprest JA, Nicolaides K, Gratacos E. Fetal surgery for congenital diaphragmatic hernia is back from never gone. Fetal Diagn Ther 2011; 29: 6–17. [DOI] [PubMed] [Google Scholar]
- 11. Neville HL, Jaksic T, Wilson JM, Lally PA, Hardin WD Jr, Hirschl RB, et al. Bilateral congenital diaphragmatic hernia. J Pediatr Surg 2003; 38: 522–24. [DOI] [PubMed] [Google Scholar]
- 12. Keijzer R, Puri P. Congenital diaphragmatic hernia. Semin Pediatr Surg 2010; 19: 180–85. [DOI] [PubMed] [Google Scholar]
- 13. Grisaru‐Granovsky S, Rabinowitz R, Ioscovich A, Elstein D, Schimmel MS. Congenital diaphragmatic hernia: a review of literature and reflection of unresolved dilemmas. Acta Paediatr 2009; 98: 1874–81. [DOI] [PubMed] [Google Scholar]
- 14. Jani J, Nicolaides KH, Keller RL, Benachi A, Peralta CF, Favre R, et al. Observed to expected lung area to head circumference ratio in the prediction of survival in fetuses with isolated diaphragmatic hernia. Ultrasound Obstet Gynecol 2007; 30: 67–71. [DOI] [PubMed] [Google Scholar]
- 15. Mullassery D, Ba'ath ME, Jesudason EC, Losty PD. Value of liver herniation in prediction of outcome in fetal congenital diaphragmatic hernia: a systematic review and meta‐analysis. Ultrasound Obstet Gynecol 2010; 35: 609–14. [DOI] [PubMed] [Google Scholar]
- 16. Peralta CF, Cavoretto P, Csapo B, Vandecrys H, Nicolaides KH. Assessment of lung area in normal fetuses at 12–32 weeks. Ultrasound Obstet Gynecol 2005; 26: 718–24. [DOI] [PubMed] [Google Scholar]
- 17. Gallot D, Coste K, Francannet C, Laurichesse H, Boda C, Ughetto S, et al. Antenatal detection and impact on outcome of congenital diaphragmatic hernia: a 12 year experience in Auvergne, France. Eur J Obstet Gynecol Reprod Biol 2006; 125: 202–5. [DOI] [PubMed] [Google Scholar]
- 18. Jain KK, Sen J, Rathee SK, Saini J. Antenatal diagnosis of a Morgagni hernia in the second trimester. J Clin Ultrasound 2008; 36: 116–18. [DOI] [PubMed] [Google Scholar]
- 19. Jani JC, Nicolaides KH, Benachi A, Moreno O, Favre R, Gratacos E. at al Timing of lung size assessment in the prediction of survival in fetuses with diaphragmatic hernia. Ultrasound Obstet Gynecol 2008; 31: 37–40. [DOI] [PubMed] [Google Scholar]
- 20. Jani JC, Peralta CF, Nicolaides KH. Lung‐to‐head ratio: a need to unify the technique. Ultrasound Obstet Gynecol 2012; 39: 2–6. [DOI] [PubMed] [Google Scholar]
- 21. Cruz‐Martinez R, Figueras F, Moreno‐Alvarez O, Martinez JM, Gomez O, Hernandes‐Andrade E, et al. Learning curve for the lung area to head circumference ratio measurement in fetuses with congenital diaphragmatic hernia. Ultrasound Obstet Gynecol 2010; 36: 32–36. [DOI] [PubMed] [Google Scholar]
- 22. Hedrick HL. Management of prenatally diagnosed congenital diaphragmatic hernia. Semin Fetal Neonatal Med 2010; 15: 21–27. [DOI] [PubMed] [Google Scholar]
- 23. Ruano R, Aubry M, Barthe B, Mitanchez D, Dumez Y, Bianchi A. Quantitative analysis of fetal pulmonary vasculature by 3‐dimensional power Doppler ultrasonography in isolated congenital diaphragmatic hernia. Am J Obstet Gynecol 2006; 195: 1720–28. [DOI] [PubMed] [Google Scholar]
- 24. Fuke S, Kanzaki T, Mu J, Wasada K, Takemura M, Mitsuda N, et al. Antenatal prediction of pulmonary hypoplasia by acceleration time / ejection time ratio of fetal pulmonary arteries by Doppler blood flow velocimetry. Am J Obstet Gynecol 2003; 188: 228–33. [DOI] [PubMed] [Google Scholar]
- 25. Okazaki T, Okawada M, Shiyanagi S, Shoji H, Shimizu T, Tanaka T, et al. Significance of pulmonary artery size and blood flow as a predictor of outcome in congenital diaphragmatic hernia. Pediatr Surg Int 2008; 24: 1369–73. [DOI] [PubMed] [Google Scholar]
- 26. Jani J, Keller R, Benachi A, Nicolaides KH, Favre R, Gratacos E, et al. Prenatal prediction of survival in isolated left‐sided congenital diaphragmatic hernia. Ultrasound Obstet Gynecol 2006; 27: 18–22. [DOI] [PubMed] [Google Scholar]
- 27. Jani JC, Nicolaides KH, Gratacos E, Valencia CM, Done E, Martinez JM, et al. Severe diaphragmatic hernia treated by fetal endoscopic tracheal occlusion. Ultrasound Obstet Gynecol 2009; 34: 304–10. [DOI] [PubMed] [Google Scholar]
- 28. Victoria T, Bebbington MW, Danzer E, Flake AW, Johnson MP, Dinan D, et al. Use of magnetic resonance imaging in prenatal diagnosis of the fetus with isolated left congenital diaphragmatic hernia. Prenat Diagn 2012; 32: 715–23. [DOI] [PubMed] [Google Scholar]
- 29. Gerards FA, Twisk JW, Tibboel D, van Vugt JM. Congenital diaphragmatic hernia: 2D lung area and 3D lung volume measurement of the contralateral lung to predict postnatal outcome. Fetal Diagn Ther 2008; 24: 271–76. [DOI] [PubMed] [Google Scholar]
- 30. Claus F, Sandaite I, DeKoninck P, Moreno O, Cruz‐Martinez R, van Mieghem T, et al. Prenatal Anatomical Imaging in Fetuses with Congenital Diaphragmatic Hernia. Fetal Diagn Ther 2011; 29: 88–100. [DOI] [PubMed] [Google Scholar]
- 31. Graham G, Devine PC. Antenatal diagnosis of congenital diaphragmatic hernia. Semin Perinatol 2005; 29: 69–76. [DOI] [PubMed] [Google Scholar]
- 32. Stoll C, Alembik Y, Dott B, Roth MP. Associated malformations in cases with congenital diaphragmatic hernia. Genet Couns 2008; 19: 331–39. [PubMed] [Google Scholar]
- 33. Ninos A, Pierrakakis S, Stavrianos V, Papaioanou G, Ajiazi A, Lordanou C, et al. Bilateral congenital anterior diaphragmatic hernia: a case report. Hernia 2006; 10: 525–27. [DOI] [PubMed] [Google Scholar]
- 34. Slavotinek AM. Single gene disorders associated with congenital diaphragmatic hernia. Am J Med Genet C Semin Med Genet 2007; 145C: 172–83. [DOI] [PubMed] [Google Scholar]
- 35. Witters I, Legius E, Moerman P, Deprest J, Van Schoubroeck D, Timmerman D, et al. Associated malformations and chromosomal anomalies in 42 cases of prenatally diagnosed diaphragmatic hernia. Am J Med Genet 2001; 103:278–82. [PubMed] [Google Scholar]
- 36. Ruano R, Yoshisaki CT, da Silva MM, Ceccon ME, Grasi MS, Tannuri U, et al. A randomised controlled trial of fetal endoscopic tracheal occlusion versus postnatal management of severe isolated congenital diaphragmatic hernia. Ultrasound Obstet Gynecol 2012; 39: 20–27. [DOI] [PubMed] [Google Scholar]