

Abstract
Introduction and Aims
Enforcement of liquor licensing laws is limited by inadequate police information systems. This study aimed to: (i) determine the effectiveness of an intervention in facilitating police recording of the alcohol consumption characteristics of people involved in assaults; and (ii) describe such characteristics by geographic area and setting of alcohol consumption.
Design and Methods
A stepped wedge trial was conducted across New South Wales, Australia. An intervention to facilitate police recording of alcohol consumption information for people involved in incidents was implemented. For people involved in an assault the proportion for which alcohol consumption information was recorded was assessed. The proportion of assaults that were alcohol related, the proportions of people that consumed alcohol prior to the assault, were intoxicated, and had consumed alcohol in various settings, are described.
Results
Post‐intervention, alcohol consumption information was recorded for 85–100% of people involved in an assault incident. The proportion of incidents recorded as alcohol‐related increased significantly (26–44.5%; P < 0.0001). The proportion of assaults classified as alcohol related was significantly greater in regional/rural areas (50–47%) than in metropolitan areas (38%). More people in metropolitan areas (54%) consumed alcohol on licensed premises prior to an assault than in regional/rural areas (39–42%), with approximately 70% of persons intoxicated regardless of setting of alcohol consumption. Twenty per cent of premises accounted for 60% of assaults linked to licensed premises.
Discussion and Conclusions
The intervention was effective in enhancing the recording of alcohol‐related information for assault incidents. Such information could enhance targeted policing of liquor licensing laws. [Wiggers JH, Hacker A, Kingsland M, Lecathelinais C, Tindall J, Bowman JA, Wolfenden L. Facilitating police recording of the alcohol‐related characteristics of assault incidents: A stepped wedge implementation trial. Drug Alcohol Rev 2015;00:000–000]
Keywords: alcohol, assault, data collection, intervention, police
Introduction
Worldwide, alcohol misuse is a significant cause of acute alcohol‐related harms, such as assaults and drink driving [1]. To prevent such harms, governments have introduced liquor licensing laws to control the supply and consumption of alcohol in a variety of community settings [1, 2]. When enforced, such laws are effective in reducing alcohol‐related harms [2, 3].
Alcohol‐related harms vary across geographic areas and alcohol consumption settings. While private venues are the most commonly reported setting for consuming alcohol [4], the amount of harm associated with consumption in licensed venues (e.g. bars, pubs, nightclubs) is disproportionately greater [2, 5, 6, 7, 8, 9], despite them operating under liquor licensing regulations to minimise the risk of harm [10]. It has been suggested that limited compliance by licensed premises with liquor licensing laws, particularly those relating to the ‘over serving’ of alcohol to intoxication, contributes to this disproportionate association [11, 12, 13]. One possible explanation for the limited compliance is less than optimal policing of liquor licensing laws. In Australia for example, just 3% of breaches of liquor licensing laws have been reported to involve breaches by licensed premises, with the remaining 97% involving breaches by consumers [5].
A number of factors have been reported to impede policing of liquor licensing laws, including a lack of skills and training [9] and limited availability of relevant intelligence information [14, 15]. Various approaches to policing, such as intelligence‐led and problem orientated policing [16, 17, 18, 19], have been suggested to address such barriers and have demonstrated effectiveness in reducing crimes, such as homicide and violence, antisocial behaviour, car theft and drug dealing [8, 20, 21, 22, 23]. These approaches generally involve the systematic collection of information regarding the characteristics of incidents, the use of such information to identify high‐risk locations, offenders and types of crime, and the subsequent selection and targeting of policing responses [2].
Despite the centrality of information systems to enhancing police capacity to respond to crime [16], analysis of police information systems in the USA [24], UK [25] and Australia [26] suggest that such systems do not facilitate the recording and analysis of information regarding what constitutes an ‘alcohol‐related incident’, the intoxication status of persons involved in incidents and the setting of alcohol consumption preceding an incident [27, 28, 29]. While a number of studies in the UK have demonstrated the collection and use of similar information [7, 30, 31], they have not involved the recording of information regarding the location of alcohol consumption prior to an incident, limiting the ability to link an incident to a specific premises.
The absence of systematic police recording of alcohol crime intelligence information limits understanding of the variability of such crimes across geographic areas and alcohol consumption settings and, in turn, the appropriate targeting of police responses. Although police recording of such information has been demonstrated to be feasible for drink driving incidents [32], only one study has reported the feasibility of recording such information for a broader range of alcohol‐related incident types [29]. The study team has previously reported that, following a 12‐month organisational change intervention in a single police region in Australia, between 87% and 100% of incidents had such information recorded [33].
As no studies have reported the ability to increase police recording of information regarding the alcohol‐related characteristics of attended incidents over an extended period of time and across diverse geographic areas, a study was undertaken to: (i) determine the effectiveness of an intervention to facilitate police recording of the alcohol consumption characteristics of people involved in assault incidents; and (ii) describe such characteristics by geographic area and setting of alcohol consumption.
Methods
Study design and setting
A stepped wedge pragmatic trial was conducted across the state of New South Wales (NSW), Australia (population 6.7 million) [34]. The stepped wedge study design provides a number of advantages in the conduct of complex practice change interventions [35, 36]. First, sequential intervention implementation allows the effect of extraneous variables on the outcome of interest to be accounted for, and for each ‘step’ to act as its own control [35]. Second, the design addresses the practical difficulty of recruiting a sufficient number of like policing units for the conduct of a parallel cluster randomised controlled trial [35, 36]. Third, the design provides an opportunity for all policing units across the state to receive the intervention, providing a key requirement for engagement and intervention sustainability [36].
The intervention was implemented sequentially in each of three, convenience‐based geographic areas defined by police administrative boundaries that, when combined, constituted the entire state (area 1: regional/rural/remote; area 2: coastal regional; area 3: metropolitan). The number and sequence of implementation areas was dictated by police operational requirements. The ‘follow‐up’ period for the trial was from the beginning of the intervention in each area to the end of data collection (45 months for area 1, 30 months for area 2 and 16 months for area 3).
The population of the three areas was approximately 1.4 million, 1.4 million and 3.9 million people respectively. The study was approved by the University of Newcastle Human Research Ethics Committee (HREC Approval No: H 609 1198).
Sample
Assault incidents
All police‐recorded assault incidents over a period of 7 years (1999–2005) were assessed. Assault incidents were selected as alcohol consumption is commonly associated with such incidents and the recorded incidence of assaults is less likely to be influenced by policing activity [37, 38, 39].
People involved in assaults
The alcohol consumption characteristics of all people involved in police recorded assault incidents in the state during the study period were assessed.
Intervention
In NSW, the policing of liquor licensing legislation is the responsibility of state‐based police services and a liquor licensing authority. All operational members of the New South Wales Police Force (approximately 12 000) were the focus of the intervention [40].
For each area, the intervention (Alcohol Linking Program) involved two components: (i) police systematically recording four items of information regarding the alcohol consumption characteristics of persons involved in attended incidents; and (ii) the use of specific implementation strategies to facilitate such information recording.
Police recording of the alcohol consumption characteristics of people in attended incidents
In NSW, routine policing practice involves police recording the details of all attended incidents in a single state‐wide database. Prior to the study, police were able to record (‘flag’), on a discretionary basis, whether an incident was ‘alcohol‐related’. Police were also able to record information regarding the alcohol consumption characteristics of people involved in attended incidents in narrative form and on a discretionary basis. Such information was not readily accessible or analysable.
The intervention involved police being asked to systematically record in the database the following four items of information for both alleged offenders and victims involved in attended incidents: (i) alcohol consumption prior to the incident (based on police observation or questioning); and, if alcohol had been consumed (ii) their intoxication status (‘Not’, ‘Slightly’, ‘Moderately’, ‘Well’ or ‘Seriously’ intoxicated), based on assessment of appearance and demeanour as per existing police protocols and evidence that intoxication can be accurately assessed in this way [41, 42]; (iii) the most recent setting of alcohol consumption (licensed premises, home/private residence, non‐licensed restaurant/cafe, public place, special event/function); and, if the most recent location of consumption was a licensed premises; (iv) the name and address of the premises.
Strategies to support implementation of police recording of information
Based on organisational change and implementation science theory and evidence [14, 43, 44, 45], the following six strategies were delivered by the research team over an 18‐month period in each area to support police to record the required information as part of routine practice.
Leadership support
Formal support for the program was gained and communicated by senior police (Commissioner/Assistant Commissioner), and a police advisory group was established to oversee the delivery of the intervention.
Enhancement of police information collection and recording systems and procedures
Standard operational procedures for the collection of the required information and their recording in the database were developed.
To facilitate police recording of the required information, the state‐wide database was modified. First, the database was modified to make recording of the four items of information mandatory. Second, if a person involved in an incident was recorded as having consumed alcohol prior to its occurrence, the incident was automatically ‘flagged’ as ‘alcohol‐related’. Third, to facilitate the ready analysis of recorded information, the database was modified to produce automated data reports.
Modifications to the database were implemented sequentially at the commencement of the intervention in each of the three study areas and were retained as routine practice following completion of the study. In area 1, the modifications were introduced in April 2002, in area 2 in June 2003 and in area 3 in September 2004.
Training of police
Mandatory training regarding alcohol‐related crime and the intervention requirements was provided to all operational police via integration into professional development program, police college curricula, shift changeover briefings and on an ad hoc basis.
Quality assurance and performance feedback
The prevalence of information recording by police was formally reported monthly to commanders, incorporating comparison against agreed benchmarks, between commands, and over time.
Communication
The rationale, progress and outputs of the intervention were communicated to all levels of police via routine and program‐specific meetings. Posters, notebook holders, computer prompts and aids were used to promote the program and its requirements.
Implementation support staff
Research staff members were located in regional police stations for the 18‐month intervention period in each area to support delivery of the above strategies.
Data collection procedures
Outcome data were extracted from the New South Wales Police incident database described above.
Measures
Police recording of information items for persons involved in assault incidents.
The proportion of people involved in assault incidents (offender/victim combined) for whom the four information items was recorded was assessed. When ‘not known’ was recorded, the record was classified as not having the information recorded.
Assault incidents ‘flagged’ as alcohol‐related
Whether an incident of assault was ‘alcohol‐related’ was determined by whether it was ‘flagged’ as such in the database.
Alcohol‐related characteristics of people involved in assault incidents
For each person recorded as involved in an assault incident, data were extracted to determine their consumption of alcohol prior to the incident, and if they had consumed alcohol, their intoxication level (‘Not’, ‘Slightly’, ‘Moderately’, ‘Well’ or ‘Seriously’ intoxicated) [41, 42] and the setting where they last consumed alcohol (‘Licensed premises’, ‘Home/private residence’, ‘Non‐licensed restaurant/café’, ‘Public place’ or ‘Special licensed event/function’).
Statistical analysis
Police recording of information items for people involved in assault incidents
As the police database and associated procedures did not support the standardised recording of the four new information items prior to intervention in each area, the level of recording of such information prior to the intervention was deemed to be zero.
‘Immediate’ (1 month after implementation commencement in each area) and ‘long term’ (from the second month after implementation commencement to the end of the study) prevalence of information recording were calculated as mean monthly proportions and standard deviation of people who had their prior alcohol consumption status, intoxication status, last setting of alcohol consumption and name/address of licensed premises (where applicable) recorded in the database.
Assault incidents ‘flagged’ as alcohol related
The mean monthly proportion and standard deviation of assault incidents that were ‘flagged’ as alcohol‐related pre and post the intervention were calculated for each of the three areas. For each area and for all areas combined, multivariate analysis was undertaken using linear regression models to test for differences in pre‐ and post‐intervention means, models that included an interaction term for study period and area, a month variable to account for seasonal variation, and an incremental month number variable to account for underlying trends over time. Similar linear regression models were used to test for differences in incidents ‘flagged’ as alcohol‐related between areas.
Alcohol characteristics of people involved in assault incidents
Mean monthly proportions (and standard deviations) of people that were recorded to: have consumed alcohol; to have been ‘intoxicated’ (‘Moderately’, ‘Well’ or ‘Seriously’ intoxicated); and to have last consumed alcohol in each specified setting of alcohol consumption were calculated for each of the three areas. Linear regression models (as described above) were used to test for differences between areas in such mean proportions.
Intoxication and setting of prior alcohol consumption
All persons recorded as ‘Moderately’, ‘Well’ or ‘Seriously’ intoxicated were collapsed into a single category: ‘intoxicated’. For ‘intoxicated’ persons, the mean monthly proportions and standard deviations that were recorded to have last consumed alcohol in each of the various settings of consumption were calculated for each area. For all persons who were recorded to have consumed alcohol in each setting, the mean monthly proportion and standard deviation that was recorded as ‘intoxicated’ was calculated for each area. For each area, for the last year of the intervention, the mean monthly proportion and standard deviation of licensed premises that were associated with ‘intoxicated’ persons involved in assault incidents were calculated, as was the median (range) number of ‘intoxicated’ persons associated with licensed premises.
SAS (version 9.3 SAS Institute Inc. Cary, NC, USA) was used for the conduct of all statistical analyses.
Results
Sample
Assault incidents
For area 1, over the 45 months from the beginning of the intervention to the end of follow‐up data collection, 65 724 assaults were recorded (1461 per month). For area 2, 38 022 assault incidents were recorded (1267/month over a 30‐month follow‐up period) and for area 3, 47 491 assault incidents were recorded (2968/month over a 16‐month follow‐up period).
People involved in an assault incident
Over the same period, 131 862 people (209 per 100 000 population per month) were recorded as being involved in an incident of assault in area 1, 75 444 (178 per 100 000 population per month) in area 2, and 90 102 (145 per 100 000 population per month) in area 3.
Recording of information for people involved in an assault incident
In the month immediately following the introduction of the intervention, the mean monthly proportion of people involved in an assault for whom data on each of the four new information items was collected ranged from 79% to 100%. Similar levels of recording were evident across the three areas (Table 1). From the second month after the introduction of the intervention to the completion of the follow‐up period (‘long term’), such proportions either slightly increased or remained the same, ranging from 85% (SD: 1.9%) for recording the setting of alcohol consumption in area 3 to >99% for the recording of intoxication level across all areas. For all information items very similar levels of recording was achieved across the three areas (Table 1).
Table 1.
Recording of alcohol characteristics information for people involved in an incident of assault at 1‐month post‐intervention and from second month to completion of study
| Information item | Area | Mean monthly % of people: 1 month post‐intervention | Mean monthly % of people: from 2nd month to end of study |
|---|---|---|---|
| Prior alcohol consumption status | 1 | 84% (n = 1497) | 89% (SD = 2.2% n = 117 409) |
| 2 | 79% (n = 1699) | 89% (SD = 3.0% n = 66 826) | |
| 3 | 85% (n = 4423) | 91% (SD = 1.2% n = 81 653) | |
| Intoxication level | 1 | 100% (n = 594) | >99% (SD = 0.08% n = 46 129) |
| 2 | 100% (n = 596) | >99% (SD = 0.07% n = 24 829) | |
| 3 | 100% (n = 1167) | >99% (SD = 0.03% n = 23 650) | |
| Setting of alcohol consumption | 1 | 86% (n = 512) | 89% (SD = 2.0% n = 41 002) |
| 2 | 84% (n = 500) | 89% (SD = 2.4% n = 21 949) | |
| 3 | 84% (n = 979) | 85% (SD = 1.9% n = 20 121) | |
| Licensed premises name and address | 1 | 96% (n = 213) | 98% (SD = 1.8% n = 15 338) |
| 2 | 98% (n = 215) | 98% (SD = 1.7% n = 8 990) | |
| 3 | 98% (n = 557) | 99% (SD = 0.8% n = 10 657) |
Assaults ‘flagged’ as alcohol related
The mean monthly proportion of incidents ‘flagged’ as alcohol‐related increased from pre‐ to post‐intervention implementation for all areas combined (pre‐intervention: 26% (SD: 7.65); post‐intervention: 44.5% (SD: 5.83) (Table 2). A similar level of increase was evident in each area.
Table 2.
Mean monthly proportion of assault incidents flagged as ‘alcohol‐related’, pre‐ and post‐intervention implementation, by area
| Area | % assault incidents ‘flagged’ as alcohol‐related pre‐intervention (SD) | % assault incidents ‘flagged’ as alcohol‐related post‐intervention (SD) | Adjusteda change in mean proportion of assaults ‘flagged’ as ‘alcohol‐related'—pre‐ to post‐intervention | P value |
|---|---|---|---|---|
| 1 | 33.2% (3.81) | 49.7% (2.90) | 17.9% | <0.0001 |
| 2 | 29.0% (3.14) | 47.0% (2.86) | 16.4% | <0.0001 |
| 3 | 18.5% (2.74) | 37.5% (2.21) | 15.0% | <0.0001 |
| All | 26.0% (7.65) | 44.5% (5.83) | 18.5% | <0.0001 |
Adjusted for seasonal variation and underlying trends over time.
The mean monthly proportion of assault incidents that were ‘flagged’ as alcohol‐related varied by area, with a greater prevalence in area 1 (49.7%; SD: 2.90) and area 2 (47%; SD: 2.86) relative to area 3 (37.5%; SD: 2.21) (Figure 1 and Table 2).
Figure 1.
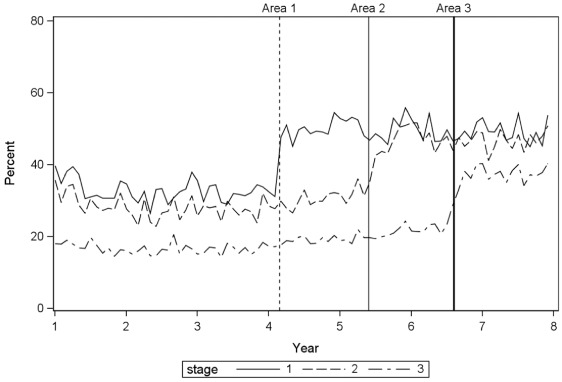
Proportion of assault incidents flagged as alcohol related, pre‐ and post‐intervention, by area.
Alcohol‐related characteristics of people involved in assault incidents
The mean monthly proportion of people involved in an assault who were recorded as having consumed alcohol prior to the incident varied significantly between areas (Table 3). A similar proportion of people who consumed alcohol before an incident were recorded across the three areas as being intoxicated. Significantly more people were recorded to have consumed alcohol in a private residence prior to the incident in areas 1 and 2, while significantly more consumed alcohol in licensed premises in area 3.
Table 3.
Alcohol characteristics of people involved in assault incidents, by area
| Alcohol characteristic | Area | Mean monthly % at completion of follow‐up | P value |
|---|---|---|---|
| Consumption of alcohol prior to incident | 1 | 39% (SD: 2.8% n = 46 150) | <0.0001 |
| 2 | 37% (SD: 2.6% n = 24 839) | ||
| 3 | 29% (SD: 1.8% n = 23 653) | ||
| Intoxicated a | 1 | 71% (SD: 2.0% n = 32 832) | 0.0006 |
| 2 | 70% (SD: 1.7% n = 17 374) | ||
| 3 | 69% (SD: 1.3% n = 16 297) | ||
| Consumed alcohol on a licensed premises b | 1 | 39% (SD: 4.4% n = 15 718) | <0.0001 |
| 2 | 42% (SD: 3.8% n = 9 179) | ||
| 3 | 54% (SD: 4.3% n = 10 789) | ||
| Consumed alcohol in public place b | 1 | 4% (SD: 1.1% n = 1 525) | <0.0001 |
| 2 | 5% (SD: 1.6% n = 1 224) | ||
| 3 | 5% (SD: 1.0% n = 950) | ||
| Consumed alcohol in a private residence/home b | 1 | 55% (SD: 3.9% n = 22 690) | <0.0001 |
| 2 | 50% (SD: 3.1% n = 11 062) | ||
| 3 | 39% (SD: 3.7% n = 7 995) | ||
| Consumed alcohol in a non‐licensed restaurant/cafe b | 1 | 0.04% (SD: 0% n = 15) | — |
| 2 | 0% (n = 0) | ||
| 3 | 0% (n = 0) | ||
| Consumed alcohol in ‘other’ location b | 1 | 3% (SD: 1.5% n = 1 054) | 0.06 |
| 2 | 2% (SD: 1.6% n = 484) | ||
| 3 | 2% (SD: 0.6% n = 387) |
aPeople whose intoxication status was recorded as ‘not known’ were excluded from the denominator. bPeople whose last place of consumption was recorded as ‘not known’ were excluded from the denominator.
Intoxication and setting of prior alcohol consumption
Little difference was evident in the mean monthly proportion of people in each setting of consumption who were recorded as being intoxicated (68% private residence; 70% licensed premises). People who last consumed alcohol in a private residence accounted for the largest proportion of intoxicated people involved in assault incidents in areas 1 (55%; SD: 4.2%) and 2 (49% SD: 3.6%) (Table 4). In contrast, people who last consumed alcohol in a licensed premise accounted for the largest proportion of those who were intoxicated in area 3 (56% SD: 4.8%).
Table 4.
Location of prior alcohol consumption for ‘intoxicated’ people (mean monthly proportions), by area
| Last place of consumption | Area 1: % of intoxicated people (n = 32 832) | Area 2: % of intoxicated people (n = 17 374) | Area 3: % of intoxicated people (n = 16 297) |
|---|---|---|---|
| Licensed premises | 39% (SD: 4.8%) | 43% (SD: 4.3%) | 56% (SD: 4.8%) |
| Residence/home | 55% (SD: 4.2%) | 49% (SD: 3.6%) | 37% (SD: 4.3%) |
| Non‐licensed restaurant/café | 0.03% (SD: 0.1%) | 0% | 0% |
| Event/function | 0% | 0% | 0% |
| Public place | 4% (SD: 1.4%) | 6% (SD: 1.9%) | 5% (SD: 1.1%) |
| Other | 2% (SD: 1.6%) | 2% (SD: 1.5%) | 2% (SD: 0.7%) |
| All | 100% | 100% | 100% |
A median of 2–3 intoxicated people per licensed premises were recorded to have been involved in an assault incident in the last year of the study across the three areas (range: area 1: 1–76; area 2: 1–53; area 3: 1–108). For the three areas respectively, 8%, 12% and 13% of licensed premises had 12 or more such people associated with the premises in this period. Of the licensed premises linked to at least one assault incident involving an intoxicated person, 20% of premises were recorded to be associated with 61.5%, 62.4% and 61.3% of such incidents for the three areas respectively.
Discussion
Following implementation of the intervention, alcohol consumption information was recorded by police for 85–100% of people involved in assault incidents. This level of recording was achieved across all four information items, in all three areas and sustained for up to 45 months. The mean proportion of assault incidents classified as alcohol related was significantly greater in regional/rural areas (50–47%) than in metropolitan areas (38%). More people in metropolitan areas (54%) were reported to consume alcohol on licensed premises prior to an assault than people in regional/rural areas (39–42%). Twenty per cent of premises accounted for approximately 60% of all assaults linked to licensed premises, with single licensed premises associated with up to 108 assaults in 1 year. Approximately 70% of persons involved in such incidents were reported as being intoxicated regardless of where they last consumed alcohol, including in licensed premises. These observed differences in the occurrence of assaults between geographic areas, and between and within settings of alcohol consumption demonstrate the potential of the newly acquired information to inform the targeting of policing strategies to high‐risk areas and settings of alcohol consumption.
Previous short‐term studies (up to 12 month of intervention) have reported that between 81% and 95% of police‐attended incidents or persons involved in such incidents have had their alcohol‐related status recorded [46, 47, 48]. The findings of the study confirm the viability of police recording this and additional alcohol consumption information, demonstrate that such recording can occur in a routine manner sustained over an extended period of time, on a jurisdiction‐wide basis, and for a variety of incident types, not only those defined by alcohol involvement, such as drink driving offences [32, 47]. The findings are supported by crime statistics routinely reported by the NSW Bureau of Crime Statistics and Research [49].
The prevalence of alcohol involvement in assaults found in this study is broadly consistent with that reported in previous studies [9, 48]. Briscoe and Donnelly reported that 23.1% of assault incidents were flagged as ‘alcohol‐related’ by New South Wales Police, a proportion that approximates the 26% of incidents flagged in this study prior to the intervention [27]. The observed increase in the prevalence of such incidents to 44.5% demonstrates the enhanced availability of information afforded to police by the intervention. However, such a prevalence is lower than the 77% of assault, offensive behaviour and language incidents reported to be alcohol related in a 2‐week study by Ireland and Thommeny [46], a difference that may be explained by the shorter study timeframe, and differences in incident types, season and location in that study.
The realisation of harm reduction benefits from the enhanced availability to police of alcohol‐related information is dependent on the manner in which the information is subsequently applied to responses by police and other agencies. While such agencies have a range of strategies for policing liquor licensing regulations [50], including education, deterrence, evidence gathering and formal law enforcement, the deployment of such strategies is suggested to be non‐systematic [14]. The enhanced information availability provides a basis for more systematic approaches to the use of such strategies [16, 17]. A randomised controlled trial of an intervention utilising police recorded incident information found a 15% greater reduction in alcohol‐related incidents associated with premises that received the intervention compared with those that received normal policing [33]. As that study was conducted using study‐specific intelligence gathering tools, further research is required to confirm these findings using routinely collected and recorded police data.
The utility of the information recorded in this study could be enhanced by combining it with information from other sources, such as police infringement notices and judicial and other actions undertaken in relation to alcohol policing [5]. Through the combining of such information, a more robust approach to identifying the need and type of police response appropriate for high‐risk areas and settings could be achieved.
The findings of this study should be considered in the context of a number of its design characteristics. First, the stepped wedge study design used in this study was modified due to the absence of pre‐intervention data regarding the level of police recording of the new information items. Notwithstanding this limitation, the consistency and replication of the observed findings in the absence of any other known explanation supports the conclusion that enhanced information availability is likely to be attributable to the intervention.
Second, the use of self‐reported last‐place‐of‐alcohol‐consumption information, and self‐reported name and address of licensed premises carries a risk of inaccuracy. The recording of information with such limitations is, however, a normal element of policing practice, providing preliminary information before the gathering of more reliable and valid evidence to establish definitive associations between incidents, people and locations. In this context, the utility of the recorded information is recognised as being restricted to having an ‘intelligence’ function, with the information not being considered to infer causality. An alternative means of identifying high‐risk locations and settings of alcohol consumption is to utilise information regarding the actual location of assaults (e.g. on licensed premises). Such information is however similarly limited by potential biases associated with the reporting of such incidents by licensees and/or the persons involved. Nonetheless, further research regarding the validity of the reported information is warranted.
Third, the intervention program was implemented in a single police jurisdiction in Australia, thereby potentially limiting its generalisability. However, as the intervention has the ability to be tailored and scaled to accommodate variations between jurisdictions in terms of information systems, data collection processes and legislative context, it has the potential to be implemented more broadly. This potential has been demonstrated by the successful implementation by New Zealand Police of an equivalent alcohol‐related crime information system, using similar implementation strategies [51].
Finally, although the intervention sought to enhance police recording of the new information items for multiple incident types, only one incident type (assaults) was considered in this study. Further research is required to determine the generalisability of the study findings to other incident types.
Acknowledgements
The research team acknowledges funding support provided by Alcohol Education and Research Foundation, New South Wales Police, Hunter New England Population Health, The University of Newcastle and Hunter Medical Research Institute. The research team would also like to acknowledge the support of the project staff involved in developing and delivering the intervention across New South Wales.
Wiggers, J. H. , Hacker, A. , Kingsland, M. , Lecathelinais, C. , Tindall, J. , Bowman, J. A. , and Wolfenden, L. (2016) Facilitating police recording of the alcohol‐related characteristics of assault incidents: A stepped wedge implementation trial. Drug Alcohol Rev, 35: 30–39. doi: 10.1111/dar.12330.
John H Wiggers DipTeach, BA(Psych/SocSci)(Hons), PhD, Professor and Director, Andrew Hacker BA(Psych)(Hons) PhD, Melanie Kingsland, BAppSci, MMedSci, PhD Candidate and Program Manager, Christophe Lecathelinais MAppMath, Statistician, Jennifer Tindall BAppSci(Hons), MMedSci, Program Manager, Jenny A Bowman BPsyc(Hons) PhD, Associate Professor, Luke Wolfenden, BSci(Psych)(Hons) PhD, Associate Professor/Research Fellow and Program Manager.
References
- 1. World Health Organisation . Global status report on alcohol and health. Geneva: World Health Organisation, 2014. [Google Scholar]
- 2. Barbor T, Caetano R, Casswell S, et al Alcohol: no ordinary commodity—research and public policy. Oxford: Oxford University Press, 2010. [Google Scholar]
- 3. Miller P, Diment C, Zinkiewicz L. The role of alcohol in crime and disorder. Melbourne: The Australian Drug Foundation, 2012. [Google Scholar]
- 4. Australian Institute of Health and Welfare . National Drug Strategy Household Survey detailed report 2013. Canberra: AIHW, 2014. [Google Scholar]
- 5. Briscoe S, Donnelly N. Liquor licensing enforcement activity in New South Wales. Sydney: NSW Bureau of Crime Statistics and Research, 2003. [Google Scholar]
- 6. Rowe S, Wiggers J, Wolfenden L, Francis L. Establishments licensed to serve alcohol and their contribution to police‐recorded crime in Australia: further opportunities for harm reduction. J Stud Alcohol Drugs 2010;71:909–916. [DOI] [PubMed] [Google Scholar]
- 7. Warburton AL, Shepherd JP. Tackling alcohol related violence in city centres: effect of emergency medicine and police intervention. Emerg Med J 2006;23:12–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Graham K, Homel R. Raising the bar: preventing aggression in and around bars, pubs and clubs. Devon: Willan Publishing, 2008. [Google Scholar]
- 9. Briscoe S, Donnelly N. Assaults on licensed premises in inner‐urban areas (Report No. 2). Sydney: NSW Bureau of Crime Statistics and Research, 2001. [Google Scholar]
- 10. NSW Government . Liquor Act NSW: NSW. 2006. Available from: http://www.austlii.edu.au/au/legis/nsw/consol_act/la2007107/ (accessed May 2015).
- 11. Andreasson S, Lindewald B, Rehnman C. Over‐serving patrons in licensed premises in Stockholm. Addiction 2000;95:359–363. [DOI] [PubMed] [Google Scholar]
- 12. Scott L, Donnelly N, Poynton S, Weatherburn D. Young adults' experiences of responsible service practices in NSW: an update. Sydney: NSW Bureau of Crime Statistics and Research, 2007. [Google Scholar]
- 13. Costello D, Robertson A, Ashe M. Drink or drunk: why do staff at licensed premises continue to serve patrons to intoxication despite current laws and interventions. Canberra: Commonwealth of Australia, 2011. [Google Scholar]
- 14. Doherty S, Roche A. Alcohol and licensed premises: best practice in policing, a monograph for police and policy makers. Payneham: Australasian Centre for Policing Research, 2003. [Google Scholar]
- 15. Barton A, Evans R. Proactive policing on Merseyside. London: Crown Publishing, 1999. [Google Scholar]
- 16. Goldstein H. Problem‐oriented policing. New York: McGraw Hill, 1990. [Google Scholar]
- 17. Radcliffe J. Intelligence‐led policing. Trends Iss Crime Crim Justice 2003;248:1–6. [Google Scholar]
- 18. Nicholas N. An environmental scan on alcohol and other drug issues facing law enforcement in Australia 2010. Hobart: NDLERF, 2010. [Google Scholar]
- 19. Nicholas R. Identifying and responding to problematic licensed premises: a guide for police. Adelaide: Australasian Centre for Policing Research, 2006. [Google Scholar]
- 20. Braga A, Kennedy DM, Warning EJ. Problem‐oriented policing, deterrence, and youth violence: an evaluation of Boston's operation ceasefire. J Res Crime Delinq 2001;38:195–226. [Google Scholar]
- 21. Braga A, Weisburg D, Waring E, et al Problem‐oriented policing in violent crime places: a randomized controlled experiment. Criminology 1999;37:541–580. [Google Scholar]
- 22. McIlwain G, Homel R. Sustaining a reduction of alcohol‐related harms in the licensed environment: a practical experiment to generate new evidence. Brisbane: Key Centre for Ethics, Law, Justice & Governance, Griffith University, 2009. [Google Scholar]
- 23. Sherman L, Eck J. Policing for crime prevention In: Sherman LWFD, Welsh BC, MacKenzie DL, eds. Evidence‐based crime prevention, 2nd edn London: Routledge, 2006. [Google Scholar]
- 24. Flynn A, Wells S. Community indicators: assessing the impact of alcohol use on communities. Alcohol Res 2013;35:135–149. [PMC free article] [PubMed] [Google Scholar]
- 25. Social Issues Research Centre . Counting the cost: the measurement and recording of alcohol‐related violence and disorder. London, UK: Social Issues Research Centre, 2002. [Google Scholar]
- 26. Morgan A, McAtamney A. Key issues in alcohol‐related violence. Canberra: Australian Institute of Criminology, 2009. [Google Scholar]
- 27. Briscoe S, Donnelly N. Temporal and regional aspects of alcohol‐related violence and disorder. Sydney: NSW Bureau of Crime Statistics and Research, 2001. [Google Scholar]
- 28. Brinkman S, Chikritzhs T, Stockwell T, Mathewson P. An indicator approach to the measurement of alcohol‐related violence In: Williams P, ed. Alcohol, young persons and violence. Canberra: Australian Institute of Criminology, 2001. [Google Scholar]
- 29. World Health Organisation . International guide for monitoring alcohol consumption and related harm. Geneva: WHO, 2000. [Google Scholar]
- 30. Moore SC, Brennan IR, Murphy S, et al The reduction of intoxication and disorder in premises licensed to serve alcohol: an exploratory randomised controlled trial. BMC Public Health 2010;10:607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Moore SC, Murphy S, Moore SN, et al An exploratory randomised controlled trial of a premises‐level intervention to reduce alcohol related harm including violence in the United Kingdom. BMC Public Health 2012;12:412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Gruenewald PJ, Stockwell T, Beel A, Dyskin E. Beverage sales and drinking and driving: the role of on‐premise drinking places. J Stud Alcohol 1999;60:47–53. [DOI] [PubMed] [Google Scholar]
- 33. Wiggers J, Jauncey M, Considine R, et al Strategies and outcomes in translating alcohol harm reduction research into practice: the Alcohol Linking Program. Drug Alcohol Rev 2004;23:355–364. [DOI] [PubMed] [Google Scholar]
- 34. Australian Bureau of Statistics . 3101.0 – Australian demographic statistics. 2005. Available at: http://www.abs.gov.au/AUSSTATS/abs@.nsf/allprimarymainfeatures/8486924370CD6CB2CA2571EF007D51B2?opendocument (accessed June 2015).
- 35. Hawkins N, Sanson‐Fisher R, Shakeshaft A, et al The multiple baseline design for evaluating population‐based research. Am J Prev Med 2007;33:162–168. [DOI] [PubMed] [Google Scholar]
- 36. Sanson‐Fisher R, Bonevski B, Green L, et al Limitations of the randomised controlled trial in evaluating population‐based research. Am J Prev Med 2007;33:155–161. [DOI] [PubMed] [Google Scholar]
- 37. English D, Holman D, Milne E, et al The quantification of drug caused morbidity and mortality in Australia. Canberra: Australian Government Publishing Service, 1995. [Google Scholar]
- 38. Giesbrecht N, Nesbitt S. Alcohol and crime: from understanding to effective intervention. J Subst Use 2001;6:215–217. [Google Scholar]
- 39. Matka E. Uses and abuses of crime statistics report No. 11. Sydney: NSW Bureau of Crime Statistics and Research, 1997. [Google Scholar]
- 40. New South Wales Police Force . 2006–2007 annual report. 2007. Available at: http://www.police.nsw.gov.au/__data/assets/file/0019/111277/2006‐07_Annual_Report.pdf (accessed August 2014).
- 41. Chesher G, Greeley J, Saunders J. Tolerance to the effects of alcohol In: Greeley J, Gladstone W, eds. The effects of alcohol on cognitive, psychomotor and affective functioning. Monograph No. 8. Sydney: National Drug and Alcohol Research Centre, 1989. [Google Scholar]
- 42. Teplin L, Lutz G. Measuring alcohol intoxication: the development, reliability and validity of an observational instrument. J Stud Alcohol 1985;46:459–466. [DOI] [PubMed] [Google Scholar]
- 43. Grieves J. Introduction: the origins of organisational development. J Manage Dev 2000;19:345–447. [Google Scholar]
- 44. Green LW, Kreuter M. Health program planning: an educational and ecological approach. Boston, MA: McGraw Hill, 2005. [Google Scholar]
- 45. Damschdoder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci 2009;4:50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Ireland C, Thommeny J. The crime cocktail: licensed premises, alcohol and street offences. Drug Alcohol Rev 1993;12:143–150. [DOI] [PubMed] [Google Scholar]
- 47. Lang E, Stockwell T. Drinking locations of drink‐drivers: a comparative analysis of accident and non‐accident cases. Accid Anal Prev 1991;23:573–584. [DOI] [PubMed] [Google Scholar]
- 48. Arro P, Crook G, Fenton T. The nature and extent of alcohol‐related incidents requiring police attention in South‐East Queensland. Brisbane: Queensland Department of Health and Queensland Police Service, 1992. [Google Scholar]
- 49. NSW Bureau of Crime Statistics and Research . NSW crime tool [November 2014]. 2014. Available at: http://crimetool.bocsar.nsw.gov.au/bocsar/.
- 50. Scott M, Dedel K. Assaults in and around bars, 2nd edn Washington, DC: Department of Justice, 2006. [Google Scholar]
- 51. New Zealand Police . Framework for preventing and reducing alcohol‐related offending and victimisation 2010–2014. Wellington: New Zealand Police, 2010. [Google Scholar]