

Abstract
Background Humour is a complex, dynamic phenomenon that mainly occurs in social situations between two or more people. Most humour research reviews rehearsed as opposed to spontaneous humour and rarely review the patients’ perspective.
Aim We explore patients’ perspectives on the use of humour in health care. We discuss the asymmetrical and divergent humour use between patients and clinical nurse specialists and posit nurses’ approaches to risk as a contributing factor.
Design A constructivist grounded theory collated researcher‐provoked (interviews, observation, field notes, pre‐and post‐interaction audio diaries) and non‐researcher‐provoked data (naturally occurring interactions) over 18 months. This paper is based upon four patient focus groups. A constant comparison approach to data collection and analyses was applied using interpretative and illustrative frameworks that balanced what was ‘known’ and ‘unknown’ about humour.
Setting and participants Patients were recruited from four patient–peer groups. Three audio‐taped (n = 20) and one observed focus group interactions (n = 12) were undertaken at the groups’ regular meeting places.
Results Patients hold a broad appreciation of humour and recognize it as being evident in subtle and nuanced forms. Patients wish health‐care staff to initiate and reciprocate humour.
Conclusion A chasm exists between what patients apparently want with regard to humour use in health‐care interactions and what actually transpires. Initiating humour involves risk, and risk‐taking requires a degree of self‐esteem and confidence. Nurses are, arguably, risk‐averse and have low self‐esteem. Future research could review confidence and self‐esteem markers with observed humour use in nurses and their interactions across a range of specialities.
Introduction
Humour is a complex, dynamic phenomenon that primarily occurs in social situations between two or more people. 1 However, most humour research to date has focussed on the humour‐health hypothesis – the concept that humour has a positive direct or indirect impact upon health. This body of research and related others largely consists of humour measurement scales being applied to healthy young people in laboratories using rehearsed humour interventions (e.g. jokes, cartoons, comedy videos). 2 Conversely, humour in health‐care interactions is a relatively underdeveloped area whereas research into the patients’ contribution to health‐care interactions per se is, arguably, equally sparse.
In this paper, we review patients’ perspectives on the use of humour in health‐care interactions as provided by three focus groups of patients (lung, breast, prostate cancer) and the observation of one stroke group. The data presented are extracted from a larger grounded theory study on humour use in clinical nurse specialist (CNS)–patient interactions 3 and explore a particular issue that arose out of the main study: the asymmetrical and divergent humour uses of patients and CNSs within health‐care interactions. The aim of this paper is, therefore, threefold:
-
1
To explore patients’ perspective on humour use in health‐care interactions.
-
2
To compare and contrast the patients’ perspectives on humour use in health‐care interactions with the main study’s baseline data corpus and follow‐up data that suggested that CNSs and patients displayed asymmetrical and divergent humour use(s) and
-
3
To suggest the differences between patients’ perspectives on humour and the CNSs approach to humour in health‐care interactions may partly be explained by how risk is perceived by CNSs.
The paper is therefore organized into four parts. First, we briefly discuss the challenges pertaining to humour research. Second, we review how the methods used in the (main) study addressed these challenges. Third, the key findings from the main study are outlined, specifically the asymmetrical and divergent humour use evident between CNSs and patients. Fourth, we present previously unreported findings on patients’ perspectives on humour in health‐care interactions. Finally, we posit nurses’ approaches to risk as a contributing factor in explaining their apparent reluctance to initiate humour.
Researching the phenomenon of humour
There are numerous challenges in researching humour generally; more so when the focus of study is spontaneous humour in health‐care interactions. First, humour is not a unitary construct although it is often viewed as a stable expression of personality in humans. 4 Second, it is multifaceted – involving social, 5 cognitive‐perceptual, 6 emotional (e.g. mirth; 7 and behavioural (e.g. laughter 8 ) aspects. What it is determines, to some extent, if or how it is recognized, understood and reciprocated (or not). Third, the phenomenon therefore needs to be appropriately captured (data collection) and interpreted (data analysis).
Rehearsed humour
The vast majority of existing humour‐health research focuses on the humour‐health hypothesis: the contention that humour has a positive (direct or indirect) impact upon health. Consequently, most humour research attempts to distil the phenomenon into some kind of ‘sense of humour’ measurement scale [e.g. 3WD Humour test, 9 situational humour response questionnaire (SHRQ), 10 humour styles questionnaire (HSQ) 11 ] with a focus on rehearsed humour interventions (e.g. cartoons, jokes). It invariably fails to account for the inextricably social aspect of the phenomenon and the innumerable confounding variables likely to arise (e.g. immunity studies – measuring only salivary immunoglobulin) – even in laboratory conditions in very specific groups (young, health, psychology students). There are, therefore, a number of areas in (rehearsed) humour‐health research that are poorly addressed. For example, the consideration of humour as potentially negative (as opposed to positive) phenomenon, humour use in ill (as opposed to healthy) individuals, recognizing that humour is principally a social entity (as opposed to laboratory‐based) and consequently a spontaneous (as opposed to rehearsed) activity.
Spontaneous humour and health‐care interactions
There are arguably different challenges in researching spontaneous humour, specifically humour in interactions. For example, ethnomethodologists have focussed on laughter as the indicator of humour support 12 although Hay 13 provided a welcome adjunct to existing research via her Conversation Analytic study that reviewed humour support other than laughter (e.g. echoing humour, developing humour). In health care, humour (via laughter) has been reviewed in physician–patient interactions 14 , 15 , 16 , 17 enhancing the growing body of physician–patient interaction data. 18 Conversely, the study of humour in nurse–patient interactions is less prevalent 19 , 21 . Consequently, much of what is written on humour in nurse–patient or nurse–peer settings tends to be opinion‐based and has a preference for prerequisites and exclusion zones 22 (see Ref. 2). Nevertheless, nurses provide the vast majority of direct patient care and might be perceived as being ‘closer’ to the patients. It follows, therefore, that humour might be more prevalent in nurse–patient interactions.
The derisory number of studies devoted to humour in nurse–patient interactions equates with the limited attention given to nurse–patient interactions per se. 23 Gafaranga and Britten 24 suggest the patient’s contribution to interactions has been similarly neglected. Correspondingly, the patients’ contribution to, or perspectives on, humour in health‐care interactions is lacking. We seek to address those omissions.
The methods and theory from the main study will now be briefly reviewed highlighting how the difficulties in capturing and analysing the phenomenon were addressed.
Methods
There were two particular challenges in this study: (i) how to capture spontaneous humour and (ii) recognize humour and/or interpret humour. Accordingly, a flexible and iterative approach to data collection and analysis was required. A constructivist grounded theory approach 25 incorporating constant comparison with open, axial and selective coding was therefore adopted. 26 A constructivist grounded theory approach allows for researcher–participant co‐construction of data and is useful when reviewing areas of which little is known. 27 The main study’s data and the data specific to this paper is outlined in Fig. 1.
Figure 1.
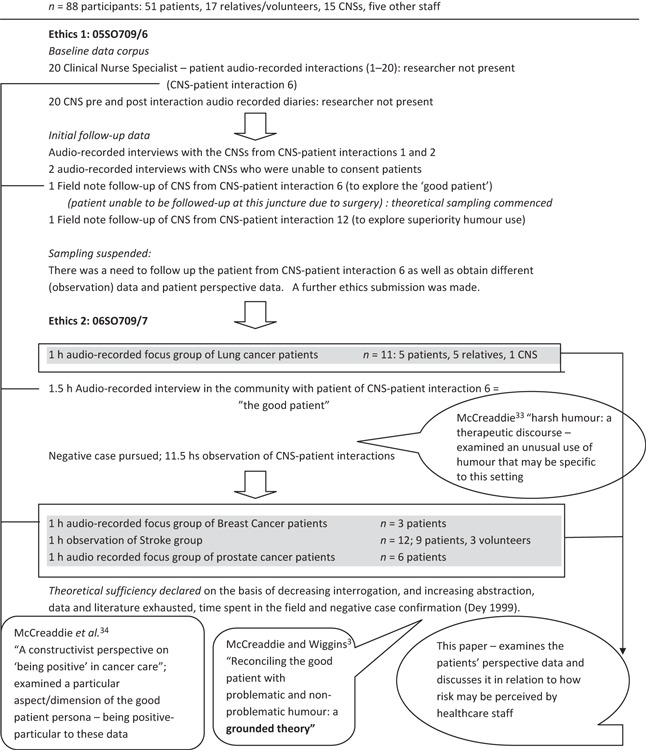
Overview of data in study, publications and data specific to this paper n = 88 participants: 51 patients, 17 relatives/volunteers, 15 CNSs, five other staff.
The main study (05/SO709/6 and 6SO709/7)
The baseline data corpus (Table 1) consisted of twenty naturally occurring CNS–patient interactions and CNS pre‐ and post‐interaction audio diaries. CNSs were asked to audio record two consecutive health‐care interactions of no <20 min duration. The researcher was not present and the CNSs and patients were informed that the study was broadly about communication in health care. CNSs were also asked to record pre‐interaction diaries responding to questions contained in separate pre‐ and post‐interaction sealed envelopes. The post‐interaction envelope contained questions on the CNSs perception of humour use (e.g. smiling, laughter). Consequently, the focus of the study may have been explicit to the CNS at this point. The data contained within the study comprised researcher‐provoked data (e.g. naturally occurring interactions) and non‐researcher‐provoked data (e.g. interviews, questions, field notes).
Table 1.
The baseline data corpus
| 20 CNS‐patient interactions |
| CNSs asked to record 2 interactions consecutively if possible |
| CNSs and patients advised the research is about ‘communication’ |
| 20 CNS pre and post interaction diaries |
| Pre: The CNS was asked to respond to a sheet of open ended questions regarding the patient and the interaction, including, environment, length of relationship, condition etc. |
| Post: Following the interaction CNSs were asked to open a sealed envelope. This contained a sheet of open‐ended questions regarding the CNSs perspective on the interaction and included specific questions on humour e.g. smiling? laughter? The CNSs may therefore, have been alerted to the focus of the study when undertaking the second interaction |
The initial follow‐up data (Fig. 1) comprised audio‐recorded interviews and field notes of CNSs involved in the twenty CNS–patient interactions and two non‐consenters. At this juncture, sampling was suspended as further data and different data (e.g. observation, patients’ perspectives) were required to develop theory. This necessitated a second successful ethics submission. Both ethics submissions addressed issues of anonymity, confidentiality and data protection.
The patients’ perspective data: participants and settings (06SO709/7)
The participants were recruited from peer group settings that largely mimicked those of the CNSs in the baseline data corpus (lung, prostate and breast cancer, stroke). Each of the focus group participants knew each other with the exception of four ‘new’ members in the lung cancer group. This was considered important in terms of obtaining spontaneous and relatively ‘authentic’ data. The focus group participants met with each other regularly (weekly/fortnightly). Following initial contact and information provision regarding the study, the researcher was invited to attend the group meeting to consent and collect data.
The patients’ perspective data: collection and analysis
Focus group data collection took place over a period of 6 months towards the end of the study (Table 2). Groups one, three and four were audio‐recorded and opened with a request for participants to discuss their health‐care experiences generally and ‘communication’ specifically. Humour emerged (spontaneously) without being prompted. Thereafter, the first author followed up the participants’ understanding of the humour expressed and how this related to their experiences of humour in health‐care interactions. In group two, the first author attended and observed a stroke group’s discussion of forthcoming social events. This group was observed as it had been suggested by group facilitators that group members may be uncomfortable with audio‐recording because of their communication difficulties.
Table 2.
Focus group participants (patients perspectives)
| Group 1 lung cancer n = 11 (three male) | Group 2 stroke n = 12 (seven male) | Group 3 breast cancer n = 3 | Group 4 prostate cancer n = 6 |
|---|---|---|---|
| 5 patients | 9 patients | patients | patients |
| 5 relatives | 3 volunteers | ||
| 1 CNS | |||
| Meeting place of group | Meeting place of group | Cancer Support Centre | Cancer Support Centre |
| Audio taped 45 min | Observed for 1 h | Audio taped 75 min | Audio taped 90 min |
| April 2006 | August 2006 | September 2006 | September 2006 |
Interpretative and illustrative frameworks were applied to all data (3, 4). These incorporated humour theories, non‐laughter humour support, discursive features, prosodical features of speech and, at the level of axial coding, an amended form of Martin’s 29 (psychological) overview of humour. Consequently, various aspects of humour were interpreted and illustrated, for example when it occurred, where (in the interaction) how often, what (theoretical) aspect it represented, who initiated and who reciprocated (or not). 30 The interpretative and illustrative frameworks attempted to balance what was ‘known’ about humour (theoretical origins and form) against what was ‘unknown’ (different or unusual presentation). The interpretative and illustrative frameworks emerged during analysis and out of the application of the coding paradigm of Strauss 26 , 31 and Strauss and Corbin 32 , involving open (e.g. gerunds, in vivo codes, constructs), axial and selective coding.
Table 3.
Interpretative and illustrative frameworks
| Humour Theories |
| Superiority social (Hobbes) the degradation theories of humour. e.g. humour agains others (sarcasm) or self (self‐disparaging humour) |
| Incongruity cognitive (Kant) is more typically like a joke. A punch‐line or jab‐line that is at odds with set‐up |
| Release: psycho‐analytic (Freud) is humour released by excess energy which may mask other motives/desires e.g. gallows humour |
| Humour support 13 Examples: |
| Recognition of humour = play along with humour |
| Understanding humour = echo or overlap of speech or humour |
| Amended Jefferson system 28 text based transcription which reviews prosodical features of speechassociated with laughter. Examples: |
| £smile£ denotes smiley voice |
| ha denotes laughter particle (out‐breath) |
| soft softness in volume |
| So::o colon mid‐word denotes stretched sound |
| Martin 29 psychological aspect of interaction –amended as it relates to healthcare. Examples: |
| Cognitive = previous experience of healthcare/others, understanding/education, perception of locus of control |
| Social situational = environment (home/clinic), presence of others, gender, age, length of relationship, length of interaction |
Table 4.
Interpretation and illustration of humour use applied to all data
| Humour aspect | Interpretation | Illustration |
| Humour theories | √ | X |
| Non‐laughter humour support | √ | √ |
| Prosodical features of speech | X | √ |
| Discursive features | √ | √ |
| Overview of humour (in context) Martin 29 | √ | √ |
The grounded theory: key findings from the main study
The main study provided a substantive theory suggesting that patients’ use humour to reconcile a good patient persona and establish and maintain a meaningful and therapeutic interaction with CNSs. The good patient persona is the sum of particular aspects (compliance, sycophancy, positive coping, displaced concern) being enacted to varying degrees within the situated context of the interaction. The good patient persona needs to be maintained within the interaction, and this is reconciled with potentially problematic or non‐problematic humour. In other words, patients need and want a meaningful and therapeutic interaction and they ‘adopt’ (consciously or otherwise) a good patient persona to ingratiate themselves with CNSs. Nevertheless, patients have a range of fears, anxieties and questions that need to be attended to within any health‐care interaction.
Patients may potentially jeopardize the meaningful and therapeutic interaction they wish to obtain by raising fears and anxieties. Hence, patients use humour to affiliate and to encode or express concerns. Sometimes this humour is simply recreational or non‐problematic (e.g. incongruity humour is more affiliative humour) and therefore tends to be more explicit. However, patients may also use less explicit forms of humour (SDH, gallows) and in some circumstances this may be problematic, particularly when it is not recognized as humour or perceived as (potentially) problematic by the CNS. The theory therefore differentiates (potentially) problematic humour from non‐problematic humour and notes that how humour is identified and addressed is central to whether patients’ concerns are resolved or not.
What constitutes potentially problematic humour and non‐problematic humour and how this arises within interactions is discussed elsewhere. 3 However, a key finding – both observed and reported (by patients and CNSs) – was that patients were much more likely to initiate and reciprocate humour than the CNS. There being only one exception to this; a negative case of a CNS in sexual and reproductive health working with female drug users. 33 CNSs were generally unaware of when patients were using humour unless it was structured more like a joke (e.g. incongruity humour) Patients, in pro‐actively initiating and reciprocating humour with health‐care staff, were also noted to have different humour preferences or uses from CNSs. Thus, CNSs used, in turn, superiority, incongruity, gallows and self‐disparaging humour (SDH) while patients used SDH, gallows and incongruity – superiority humour (e.g. sarcasm) was rarely evidenced.
There were therefore considerable (observed and reported) differences between patients and CNSs with regard to humour use in health‐care interactions, and these were evident in the baseline data corpus and follow‐up data. Table 5 provides an overview of the differences in humour use between CNSs and patients and confirms the source of data.
Table 5.
The differences between patients and CNSs in relation to humour use in healthcare interactions
| Humour aspects | Patients | Data source/evidence | CNSs (findings from main study) |
|---|---|---|---|
| Humour recognition | Recognised humour: acutely aware of humour use | BDC, f/up and this paper | Lack of awareness: generally, did not recognize humour |
| Humour understanding | ?a more broad and subtle understanding of humour e.g. as a means to an end not an end in itself | This paper | Generally thought patient humour use due to anxiety |
| Humour reciprocation e.g. laughter, smiles | Always reciprocated humour initiated by CNS | BDC | Generally, rarely (overtly) reciprocated humour initiated by patient |
| Humour initiation | Often initiated humour | BDC and this paper | Rarely initiated humour: patients twice as likely to initiate humour than the CNS (BDC) |
| Humour preferences/types | SDH, gallows, incongruity | BDC | Superiority, incongruity, Gallows, SDH |
BDC, baseline data corpus: 20 CNS‐patient health care interactions and 20 pre and post interaction diaries in the main study. f/up, follow‐up data: audio recorded interviews, field note follow‐up in main study.
The patients’ perspective data were obtained to service theory generation (main study): to corroborate (or deny) the good patient persona and (problematic and non‐problematic) humour use and whether patients were aware of this good patient persona. However, it also provided the basis from which to explore why CNSs and patients apparently have such asymmetrical and divergent humour uses. We now present the patients’ perspective data and thereafter discuss the distinct differences in humour use between CNSs and patients.
Patients’ perspective data: findings
Patients seek more than an interaction with CNSs and others because of the complexity and uncertainty of the situation in which they find themselves. Patients reported a broad and often subtle view of humour use in health‐care interactions, specifically those concerned with establishing their identity as an individual patient and as part of a group. For patients, humour was important in both establishing their identity and in developing a meaningful therapeutic interaction: as a means to an end, not necessarily an end in itself. Being cared for is the pinnacle of the patients’ endeavours and might provide some reassurance that their treatment will be individual and enduring as well as safe and potentially therefore more successful.
Two subcategories emerged from the patients’ perspective data: ‘humour as ambience and support’ and ‘humour, narrative identity and caring’. Humour as ambience and support effectively provides the context and backdrop for the more proactive affiliation of humour; narrative identity and caring. We will therefore briefly review one of the dimensions of this contextual subcategory prior to discussing humour, narrative identity and caring.
Humour as ambience and support
Humour as ambience and support reflects the emotional crisis that might be initially evident in potentially life‐threatening illness (kicked into touch) with the patients’ broad view of humour as a positive outlook (bright and cheery) mediated with the possible confounding expectations of others (positive and strong). There is therefore a fulcrum upon which ‘bright and cheery’ and ‘positive and strong’ are balanced. The dimension of ‘positive and strong’ relates to the broader palliative care literature and is reviewed in a separate article. 34 Here, we have chosen to concentrate on the patients’ broad appreciation of humour, the dimension of ‘bright and cheery’.
Bright and cheery
Blank et al. 34 contend that illness is likely to impact upon an individual’s humour appreciation. This was evident in patients’ reports of their immediate responses that subsequently gave way to the need for more optimistic strategies that ‘boosted my morale no end’ (Billy, lung cancer group 1). Several respondents claimed to despise any propensity for ‘doom and gloom’. Hence, patients held true to a diverse and encompassing definition of humour in terms of smiles or being ‘bright and cheery’.
A bright and cheery ambience might create a sense of poise and assurance from the nurses that resonates with patients who are subsequently imbued with confidence. Patients were cognizant of the demands on the health‐care system: the associated workload and the potential for possible failures or mistakes being juxtaposed with their well‐being which was – to all intents and purposes – contingent upon health‐care staff. Prior to the following extract, the participants were asked whether they had any particular examples of humour being used in a positive or negative way:
Extract 1: Graeme – prostate cancer, group 4
When you are speaking about humour, the day I went for my biopsy, there were eight men and they were all going in within a half hour period. The two nurses that were dealing with the men, you didn’t actually see the person that was going to be doing your biopsy, but the nurses that dealt with the men were good. Trying to keep you cheery and I always remember that I was eighth out of eight. I was the last. I mean you are watching all these guys going away, they were all going away happy and coming back “oh oh.” Number seven. I always remember the guy that was number seven had a reaction and I was due to go in when they were rushing round. But the nurses were bright, they were happy, they were cheery which I think was just right for the situation because there was a lot of worried men there. I thought that was probably the right way.
Various (nurse) authors have suggested that crises or deep psychological distress are exclusion zones with regard to humour. 22 , 36 , 37 There is a certain absurdity in Graeme’s reporting of the above ‘crisis’– pain, concern, emerging crisis and his concomitant approbation of the relatively humorous ambience as being ‘right’ in those circumstances. Perhaps the ‘bright and cheery’ ambience creates an outward impression (to patients) of a potentially critical event being managed effectively and efficiently thereby buffering any potential alarm. A serious and unsmiling approach by the nurses to the crisis might have increased the alarm of the waiting patients. In this instance, humour use by nurses might re‐create the situation as relatively non‐threatening or at least creates that outward impression.
The contextual elements of humour as ambience and support ostensibly operate in a vacuum of the initial flux of diagnosis, prognosis, initial treatment and on‐going treatment. Hence, ‘bright and cheery’ operates to greater or lesser degrees across an evolving spectrum of the patient’s experience. It might appear superficial or as a very light touch at one end of spectrum into something more proactive, intense and fulfilling. Thus, ambience and support merge into the more proactive or assertive subcategory; humour, narrative identity and caring. In this subcategory, the patient seeks to demonstrate identity beyond that of a patient via attempts to affiliate and consolidate interactions that adequately reflects those aspirations. Notably, humour is a key part of this identity work.
Humour, narrative identity and caring
Strauss (p. 11) 31 contends that identity is effectively ‘fateful appraisals made of oneself – by oneself and by others’. Consequently, actions are ‘fashioned’ upon anticipation of ‘their judgements’. The ‘imputation of motives’ Strauss (p. 50) 31 by others is part of that process and is similarly re‐appraised. We would argue that establishing an identity within health‐care interactions (CNS–patient and patient–peers) is as important for the individual as it is for others and that humour use is a key part of this process.
There were therefore two dimensions to this subcategory. ‘First names, football and herbal tea’ denotes the individual or self‐identity that has begun to emerge against the backdrop of humour as ambience and support. There is recognition (by others) of the individual, followed by a more ‘personal’ or individualized rapport that endures via the individual being remembered. Thus, individual identity is enshrined and this is primarily achieved through humour and self‐disclosures. The second dimension –caring and a sense of belonging: group identity– was less recreational and more revealing, assimilating the individual identity into a group of peers, be they nurses or patients (or both). Humour evidenced in these narratives was arguably similar to that shared among friends, 38 thereby indicating a mutual and interdependent coexistence that matured over time.
First names, football and herbal tea
Dewey and Bentley 39 maintained that the extent of knowing is dependent upon the naming of an individual. Extracts two and three both denote the relative kudos of knowing first names, be they patients or those of staff.
Extract 2: Billy – Lung cancer focus group 1
They had a smile on their face, they called you by your first name. We joked about where we were going at the weekend. What’s going on in Glasgow, about Rangers playing Villareal and being robbed.hha. h., They never lost but they were out (laughter).
Extract 3: Jean – Lung cancer focus group
My district nurses and doctors, they come in just to see you. You know their first names because we had a drink of herbal tea and they are all like that.
The above extracts highlight the importance of first names. However, it is not just simply about first names. Both extracts disclose particular information specific to their self‐identity (football and herbal tea) with each, specifically extract two, presented in a humorous way. For example, extract three continues with the CNS, who usually facilitates this group, gently teasing Jean about her predilection for herbal tea which Jean reciprocates by using (like Billy in extract two) SDH. The first name posits recognition, the self‐disclosure individualizes and creates a self‐identity and both are packaged with self‐effacing humour. The naming and the self‐identity, oiled as it is by humour, are arguably the beginning of an image that is more likely to endure or be remembered. Numerous participants discussed the importance of being remembered as part of belonging, even to the extent of feeling a sense of loss once the treatment period ceased.
Patients therefore laud the importance of this process of recognition and in establishing an individual identity with the potential to endure and report humour use as a key facet of this process. However, to what extent, if any; are those processes a pre‐meditated undertaking by the patients?
Extract 4: Lara – Breast cancer support group 3
Sometimes, especially at (the hospital), they are so busy. They just go through the motions.
They don’t have time. What I did find was befriend them in a way, but don’t talk about your cancer, talk to them about other things like holidays and days off and I think you get a better interaction with them and you felt better. That place is scary, they have no time.
Here Lara considers that there are unreasonable demands placed upon health‐care staff’s time and that mistakes can happen. In such circumstance, a patient who has some kind of relationship (as opposed to ‘interaction’) with a member of staff might perhaps fare better than someone who is less well known. However, this might not be the motivation behind Lara’s apparent ‘strategy’ aimed at ‘befriending’ the staff. Notably, she ignores the commonality of the disease (cancer) and instead invokes other perhaps ‘safer’ topics of discussion. Are these topics safer for the over‐worked staff or Lara? In this instance, perhaps the ‘deliberate’ non‐focus on cancer merely serves as a distraction or as a genuine humane interest in individuals, rather than as a way of Lara ingratiating herself with over‐worked staff on which, possibly quite literally, her life depends. Either way, Lara is clearly alluding to a need for something other than a formal clinical interaction.
The final extract presented arguably demonstrates the extent of narrative identity and caring primarily among patients, rather than between patients and health‐care staff. It is taken from field note observations of a Stroke Group attended by nine ‘patients’ and three volunteers. It is an older mixed sex group, comprising ex‐patients who have varying degrees of disability because of stroke. Thus, participants might have significant physical disabilities with regard to mobilizing or speaking. The group meets once a fortnight and volunteers facilitate the group. A male volunteer, Bob, is leading the discussion about upcoming festive activities:
Extract 5: Field note extract: stroke group 2
A ‘discussion’ ensues regarding the organisation of the Christmas lunch including the potential for a Christmas production that only Bob appears to be interested in doing. There is much looking at the floor while he talks about who’ll possibly do what, playing different roles etc. in a possible pantomime. He then asks who could be Santa. At this, Peggy who’d taken a bit of a ribbing from Bob previously, pats him deliberately on his rotund belly! This raises a big laugh, more banter and Peggy laughs and smiles across at me. Each member of the group speaks at some point, almost invited individually to contribute by Bob. Bob is going on a boat trip with three other guys. Leigh (another volunteer) asks how many [alcohol] bottles there would be. There’s much gentle banter and ribbing, occasionally building to a belly laugh, literally as in Peggy tapping Santa’s belly, almost as if people are keen to enjoy the company and camaraderie. What is particularly interesting is how people allow each other to speak and assist occasionally, particularly the patients more so than the volunteers. It’s respectful. As if ‘I know how difficult it is’ and occasionally I heard ‘you can do it/that’s it’ from John, another participant sitting next to me, who otherwise said nothing.
In the above extract, Peggy has severe speech problems. She is dysarthric: she can say occasional words, but might struggle to say the right words. She has had a left cerebral vascular accident with a right‐sided hemiplegia. She walks with difficulty with a tripod but has no use of her right arm. She is sitting to the right of Bob the volunteer and so when she pats him on his belly she quickly adjusts her posture and does so deliberately. It is almost triumphant and the humour endures for the rest of the session as both Peggy and the first author continue to exchange smiles. Despite Peggy’s interactional incapacities, her physical lampooning of Bob as a prospective Santa, because of his large abdomen, was the most humorous instance in all the groups. Her humour was all the more funny because it triumphed over Bob’s teasing (and what the first author perceived to be his somewhat bumptious manner) and Peggy’s disabilities.
Limitations
There are particular limitations with this study. First, the data would have benefited from observations of the health‐care interactions of the patients’ whose (retrospective) perspectives were reported. Second, the focus groups were all peer groups whose members were largely known to each other. Focus groups comprising individuals not known to each other might have produced different findings. Third, the study was carried out in a particular geographical area of the UK. There are, as noted by Davies, 40 distinct cultural differences in the expression of humour. Consequently, the study is specific to the geographical area studied. Four, the interpretative and illustrative framework might have ‘forced’ the data. However, it is our contention that the absence of such a framework would have made the findings less explicit and tangible.
Discussion
The patients’ perspective data serviced theory generation in the main study. In particular, it confirmed that patients and CNSs have asymmetrical and divergent humour uses. The patients’ perspective data presented in this paper suggest that patients consider humour use as integral to their health‐care experiences with health‐care staff as well as other patients and impacts upon how they cope and assert their identity at a time of challenge and crisis.
Humour has been recognized as being an integral part of support groups, 41 and there are a number of studies exploring humour among peers in a variety of settings. 42 , 43 , 44 , 45 However, this paper notes the following: 1, patients hold a broad appreciation of humour and recognize it as being evident in subtle and nuanced forms, and 2, patients wish health‐care staff to initiate and reciprocate humour. Yet, the baseline data corpus and follow‐up data in the main study suggest a chasm between what patients want from health‐care interactions in terms of humour use and what actually transpires (Table 5). The question is – why is that so?
The main study suggested that CNSs may not identify (some) humour initiation by patients, particularly the more subtle nuances of humour use – humour that is not obviously humour (e.g. SDH, gallows). Therefore, unlike patients, CNSs lack humour awareness. Hence, they are unable to either acknowledge or reciprocate humour. Similarly, while patients apparently embrace humour use, CNSs fail to do so and rarely initiate humour. Why? Are they too busy, too task‐focused? Perhaps they are concerned that any humour initiation might compromise their ‘professional’ standing and thereby – as Wooten 46 suggests – cast doubt upon their competency as nurses? Yet, Graeme (extract one) considered that the ‘bright and cheery’ demeanour of the nurses assuaged the patients’ concerns and also established competency concurrently. Thus, professionalism and humour expression need not be mutually exclusive entities.
We suggest there might be a significant contributing factor that partially explains nurses’ apparent reluctance to initiate humour and that is how they perceive risk.
Initiating humour is a potentially risky endeavour. Who wants to tell a joke only to be met with a wall of silence? Is the silence merely a negative comment on the quality or otherwise of the joke’s content or a poor appraisal of the joke‐teller’s skill in telling the joke?
Nurses have a notoriously rule‐governed, risk‐averse profession 47 epitomized perhaps by Nightingale’s (1863: iii) 48 maxim ‘to do the sick no harm’ and expressed by a reliance upon algorithms, protocols and guidelines. Nurses are not, professionally at least, noted risk‐takers.
Several studies using personality‐trait scales suggest there is an association between a ‘good’ sense of humour and extraversion, hedonism or risk‐taking 49 , 50 , 51 . Moreover, a ‘good’ sense of humour also positively correlates with improved psychological well‐being including self‐esteem and social support. 11 , 52 However, some studies suggest that nurses may have low self‐esteem and this tends to correlate with work‐related factors, for example stress, professional satisfaction. 53 , 54 , 55 Thus, some nurses may not have low self‐esteem per se, but develop low self‐esteem as a consequence of work‐related factors.
While a good sense of humour is linked to risk‐taking (generally) and improved psychological well‐being including self‐esteem, this may not necessarily be age (or youth) related. For example, Sumners 56 reviewed 204 nurses and concluded that older, more experienced nurses had more positive attitudes towards humour use. Perhaps older, more experienced nurses have better developed and more durable social support and self‐esteem. Consequently, older nurses may be more able or willing to take risks vis a vis humour use.
Conclusion
Humour might be a risk, but, according to patients, it is a risk worth taking. Indeed, there may even be therapeutic potential in nurses initiating humour. 33 It is therefore important to consider which nurses are more likely to initiate humour use and why. Given the association between humour use and self‐esteem, social support and risk‐taking, we suggest attempting to link nurses’ self‐esteem with humour use. Are nurses’ with greater self‐esteem more likely to take a ‘risk’ and initiate humour with patients? Confidence and self‐esteem markers could be correlated with observed humour use in nurses and their interactions across a range of specialities. Future research could therefore legitimize humour as a therapeutic aspect of health‐care interactions, linking it to clinical outcomes. Researching the role of humour in helping nurses to cope and in reducing burnout – for example increasing self‐esteem and job satisfaction – would also be a worthwhile undertaking.
Conflict of interests
The authors report no conflicts of interest.
Funding
None.
Acknowledgements
The authors thank the patients and CNSs who took part in the study.
References
- 1. Martin RA and Kuiper NA . Daily occurrence of laughter: relationships with age, gender and Type A personality . Humor: International Journal of Humor Research , 1999. ; 12 : 355 – 384 . [Google Scholar]
- 2. McCreaddie M , Wiggins S . The purpose and function of humour in health, healthcare and nursing: a narrative review . Journal of Advanced Nursing , 2008. ; 61 : 584 – 595 . [DOI] [PubMed] [Google Scholar]
- 3. McCreaddie M , Wiggins S . Reconciling the good patient persona with problematic and non‐problematic humour: a grounded theory . International Journal of Nursing Studies , 2009. ; 46 : 1079 – 1091 . [DOI] [PubMed] [Google Scholar]
- 4. Foot H , McCreaddie M . Humour and laughter . In : Hargie O. ( ed . ) The Handbook of Communication Skills , 3rd edn . London : Routledge; , 2006. : 293 . [Google Scholar]
- 5. Apter MJ . A structural‐phenomenology of play . In : Kerr JH , Apter MJ. ( eds ) Adult Play: a Reversal Theory Approach . Amsterdam : Swets and Zeitlinger; , 1991. : 13 – 29 . [Google Scholar]
- 6. Koestler A . The Act of Creation . London : Hutchinson; , 1964. . [Google Scholar]
- 7. Martin RA . The Psychology of Humor: an Integrative Approach . London : Elsevier; , 2006. . [Google Scholar]
- 8. Provine RR , Yong YL . Laughter: a stereotyped human vocalization . Ethology , 1991. ; 89 : 115 – 124 . [Google Scholar]
- 9. Ruch W . Humor‐Test 3 WD (Forms A, B and K) . Germany : University of Dusseldorf; , 1983. . [Google Scholar]
- 10. Lefcourt HM , Martin RA . Humor and Life stress: Antidote to Adversity . New York : Springer‐Verlag; , 1986. . [Google Scholar]
- 11. Martin RA , Puhlik‐Davis P , Larsen G , Gray J , War K . Individual differences in uses of humor and their relation to psychological well‐being: development of the humor styles questionnaire . Journal of Research in Personality , 2003. ; 37 : 48 – 75 . [Google Scholar]
- 12. Glenn P . Laughter in Interaction . Cambridge : Cambridge University Press; , 2003. . [Google Scholar]
- 13. Hay J . The pragmatics of humor support . Humor , 2001. ; 4 : 55 – 82 . [Google Scholar]
- 14. West C . Routine Complications: Troubles with talk between Doctors and patients . Bloomington : Indiana University Press; , 1984. . [Google Scholar]
- 15. Haakana M . Laughter in medical interaction: from quantification to analysis, and back . Journal of Sociolinguistics , 2002. ; 6 : 207 – 235 . [Google Scholar]
- 16. Sala F , Krupat E , Roter D . Satisfaction and the use of humor by physicians and patients . Psychology and Health , 2002. ; 17 : 269 – 280 . [Google Scholar]
- 17. Granetk‐Catarivas M , Goldstein‐Ferber S , Azuri Y , Vinker S , Kahah E . Use of humour in primary care: different perceptions among patients and physicians . Postgraduate Medical Journal , 2005. ; 81 : 126 – 130 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Heritage J , Maynard DW . Problems and prospects in the study of physician‐patient interaction: 30 years of research . Annual Review of Sociology , 2006. ; 32 : 351 – 374 . [Google Scholar]
- 19. Astedt‐Kurki P , Isola A . Humour between nurse and patient and among staff: analysis of nurses’ diaries . Journal of Advanced Nursing , 2001. ; 35 : 452 – 458 . [DOI] [PubMed] [Google Scholar]
- 20. Dean RA , Gregory D . More than trivial: strategies for using humor in palliative care . Cancer Nursing , 2005. ; 28 : 292 – 300 . [DOI] [PubMed] [Google Scholar]
- 21. Thornton J , White A . A Heideggerian investigation into the lived experience of humour by nurses in an intensive care unit . Intensive and Critical Care Nursing , 1999. ; 15 : 266 – 278 . [DOI] [PubMed] [Google Scholar]
- 22. Sullivan JL , Deane DM . Humor and health . Journal of Gerontology Nursing , 1988. ; 14 : 20 – 24 . [DOI] [PubMed] [Google Scholar]
- 23. Shattell M . Nurse‐patient interaction: a review of the literature . Journal of Clinical Nursing , 2004. ; 13 : 714 – 722 . [DOI] [PubMed] [Google Scholar]
- 24. Gafaranga J , Britten N . Patient participation in formulating and opening sequences . In : Collins S , Britten N , Ruusuvuori J , Thompson A. ( eds ) Patient Participation in Health Care Consultations: Qualitative Perspectives . Berkshire : Open University Press; , 2007. : 104 . [Google Scholar]
- 25. Charmaz K . Constructing Grounded Theory: a Practical Guide Through Qualitative Analysis . London : Sage Publications; , 2006. . [Google Scholar]
- 26. Strauss A , Corbin J . Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory , 2nd edn . London : Sage Publications; , 1998. . [Google Scholar]
- 27. Morse JM . Situating grounded theory with in qualitative inquiry . In : Schreiber RS , Stern PN. ( eds ) Using Grounded Theory in Nursing . New York : Springer Publishing Company; , 2001. : 1 . [Google Scholar]
- 28. Sacks H , Schegloff EA , Jefferson G . A simplest systematics for the organisation of turn‐taking in conversation . Language , 1974. ; 50 : 696 – 735 . [Google Scholar]
- 29. Martin RA . Humor, laughter, and physical health: methodological issues and research findings . Psychological Bulletin , 2001. ; 127 : 504 – 519 . [DOI] [PubMed] [Google Scholar]
- 30. McCreaddie M , Payne S . Evolving grounded theory methodology: towards a discursive approach . International Journal of Nursing Studies , 2010. ; 47 : 781 – 793 . [DOI] [PubMed] [Google Scholar]
- 31. Strauss A . Mirrors and Masks: the Search for Identity . Transaction Publishers : New Jersey; , 1997. . [Google Scholar]
- 32. Strauss A , Corbin J . Basics of Qualitative Research: Grounded Theory Procedures and Techniques . London : Sage Publications; , 1990. . [Google Scholar]
- 33. McCreaddie M . Harsh humour: a therapeutic discourse . Health and Social Care in the Community , 2010. ; 18 : 633 – 642 . [DOI] [PubMed] [Google Scholar]
- 34. McCreaddie M , Payne S , Froggatt K . Ensnared by positivity: a constructivist perspective on ‘being positive’ in cancer care . European Journal of Oncology Nursing , 2010. ; 14 : 283 – 290 . [DOI] [PubMed] [Google Scholar]
- 35. Blank A , Tweedale M , Cappelli M , Ryback D . Influence of trait anxiety on perception of humor . Perceptual and Motor Skills , 1983. ; 57 : 103 – 106 . [DOI] [PubMed] [Google Scholar]
- 36. Astedt P , Liukkonen A . Humor in nursing care . Journal of Advanced Nursing , 1994. ; 20 : 183 – 188 . [DOI] [PubMed] [Google Scholar]
- 37. Herth K . Contributors of humor as perceived by the terminally ill . American Journal of Hospice and Palliative Medicine , 1990. ; 7 : 36 – 40 . [DOI] [PubMed] [Google Scholar]
- 38. Holmes J , Marra M . Over the edge? Subversive humor between colleagues and friends . Humor , 2002. ; 15 : 65 – 87 . [Google Scholar]
- 39. Dewey J , Bentley J . Knowing and the Known . Boston : Beacon Press; , 1949. . [Google Scholar]
- 40. Davies C . The Mirth of Nations . New Jersey : Transaction Publishers; , 2002. . [Google Scholar]
- 41. Oliffe JL , Ogrodniczuk J , Bottorff JL , Hislop TG , Halpin M . Connecting humor, health, and masculinities at prostate cancer support groups . Psycho-Oncology , 2009. ; 18 : 916 – 926 . [DOI] [PubMed] [Google Scholar]
- 42. O’Connell B , Baker L . Managing as carers of stroke survivors . International Journal of Nursing Practice , 2004. ; 10 : 121 – 126 . [DOI] [PubMed] [Google Scholar]
- 43. Henman LD . Humor as a coping mechanism: lessons from POWs . Humor , 2001. ; 14 : 83 – 94 . [Google Scholar]
- 44. Langley‐Evans A , Payne S . Light‐hearted death talk in a palliative day care context . Journal of Advanced Nursing , 1997. ; 26 : 1091 – 1097 . [DOI] [PubMed] [Google Scholar]
- 45. Buffum MD , Brod M . Humor and well‐being in spouse caregivers of patients with Alzheimer’s disease . Applied Nursing Research , 1998. ; 11 : 12 – 18 . [DOI] [PubMed] [Google Scholar]
- 46. Wooten P . Laughter as therapy for patient and caregiver . In : Hodgkin JE. ( ed . ) Pulmonary Rehabilitation Guidelines to Success . Philadelphia : Lippincott; , 1993. : 422 . [Google Scholar]
- 47. Hart C . Nurses and Politics: the Impact of Power and Practice . Hampshire : Palgrave Macmillan; , 2004. . [Google Scholar]
- 48. Nightingale F . Notes on Hospitals , 3rd edn . London : Longman; , 1863. . [Google Scholar]
- 49. Deckers L , Ruch W . The Situational Humour Response Questionnaire (SHRQ) as a test of ‘sense of humour’ : a validity study in the field of humour appreciation . Personality and Individual Differences , 1992. ; 13 : 1149 – 1152 . [Google Scholar]
- 50. Lourey E , McLachlan A . Elements of sensation seeking and their relationship with two aspects of humour appreciation ‐ perceived funniness and overt expression . Personality and Individual Differences , 2003. ; 35 : 277 – 287 . [Google Scholar]
- 51. Forabosco G , Ruch W . Sensation seeking social attitudes and humor appreciation in Italy . Personality and Individual Differences , 1994. ; 16 : 515 – 528 . [Google Scholar]
- 52. Kuiper NA , Grimshaw M , Leite C , Kirsh G . Humor is not always the best medicine: specific components of sense of humour and psychological well‐being . Humor , 2004. ; 17 : 135 – 168 . [Google Scholar]
- 53. Karanikola MN , Papthanassoglou ED , Giannakopolou M , Koutroubas A . Pilot exploration of the association between self esteem and professional satisfaction in Hellenic hospital nurses . Journal of Nursing Management , 2007. ; 15 : 78 – 90 . [DOI] [PubMed] [Google Scholar]
- 54. Imai K . Occupational factors contributing to low self‐esteem in registered nurses and licensed practical nurses: a multivariate analysis . Journal of Universal Occupational Environmental Health , 2001. ; 23 : 13 – 22 . [DOI] [PubMed] [Google Scholar]
- 55. Fothergill A , Edwards D , Hannigan B , Burnard P , Coyle D . Self‐esteem in community mental health nurses: findings from the all wales stress study . Journal of Psychiatric and Mental Health Nursing , 2000. ; 7 : 315 – 321 . [DOI] [PubMed] [Google Scholar]
- 56. Sumners AD . Professional nurses’ attitudes towards humour . Journal of Advanced Nursing , 1990. ; 15 : 196 – 200 . [DOI] [PubMed] [Google Scholar]