
FIGURE 3.
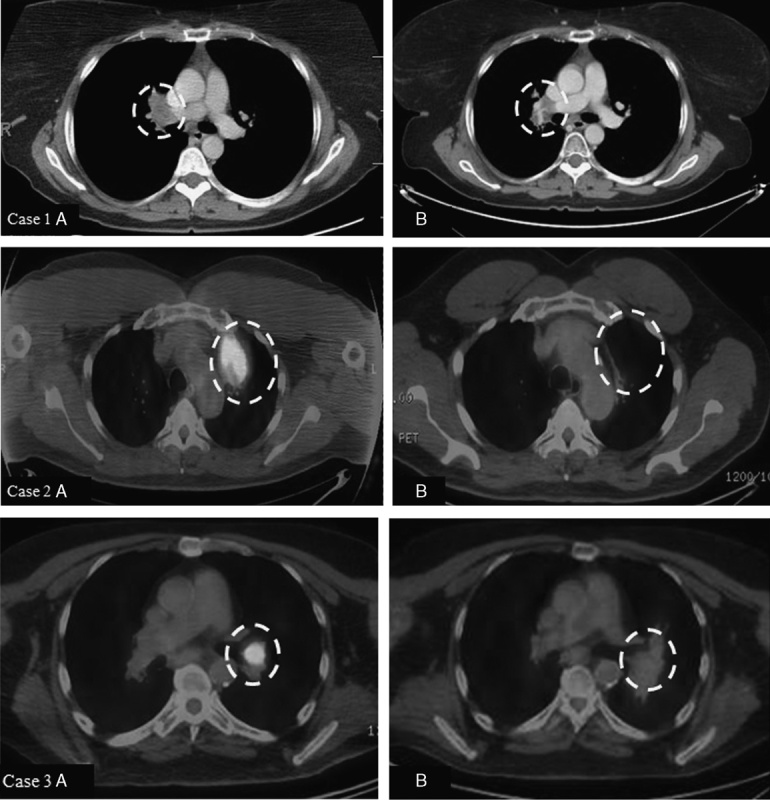
Case 1. A 48-year-old woman with stage IIIC melanoma of the right arm underwent wide local excision and axillary lymph node dissection in 2010. Computed tomography (CT) of the chest demonstrated multiple bilateral pulmonary nodules, and wedge resection of a left lower lobe lesion in July 2012 demonstrated metastatic disease. She completed ipilimumab in December 2012, and CT scan in February 2015 showed isolated progression in the right hilum (1A). She completed 36 Gy in 6 fractions to the right hilum in March 2015 followed by radiographic response. Her most recent CT chest in February 2016 showed stable findings consistent with posttreatment change and no new areas of melanoma involvement (1B). Case 2. A 55-year-old man underwent resection of primary cutaneous melanoma from the left postauricular region and was subsequently diagnosed with metastases to the left parotid and left lung in 2011. He completed ipilimumab in January 2012 with stable left parotid disease and progression at 2 sites in the left upper lobe 1 year later (2A). He completed 36 Gy in 6 fractions to 2 left upper lobe lesions in February 2013 with observation of the parotid disease. He required resection of the parotid nodule in January 2014 that confirmed melanoma. His most recent imaging from January 2016 shows no evidence of active melanoma (2B). Case 3. A 66-year-old man with stage IIIA melanoma of the left cheek diagnosed in 2012 who later developed metastatic disease to the lung in January 2014 was treated with ipilimumab. His lung lesions showed improvement; however, he developed a new and progressive left hilar lesion (3A) which was treated with 30 Gy in 5 fractions in August 2014. His most recent imaging from December 2015 shows no evidence of active melanoma (3B). The white dashed circles highlight the areas of interest described for each image.