

Abstract
Objective
As an independent linear association between 25-hydroxyvitamin D (25(OH)D) and testosterone levels is controversial, this study aimed to explore this topic in men with chronic spinal cord injury (SCI), who exhibit a high prevalence of both androgen and vitamin D deficiency.
Design
Forty-nine men with chronic SCI consecutively admitted to a rehabilitation program underwent clinical/biochemical evaluations.
Results
Deficiency of 25(OH)D (<20 ng/mL) was found in 36 patients (73.5%). They exhibited significantly lower total testosterone and free testosterone levels, higher parathyroid hormone (PTH) and HOMA-IR, a poorer functional independence degree, and were engaged in poorer weekly leisure time physical activity (LTPA). Significant correlates of 25(OH)D levels were: total testosterone, free testosterone, PTH, functional independence degree and weekly LTPA. At the linear regression models, lower 25(OH)D levels were associated with both lower total and free testosterone after adjustment for age, smoking, alcohol consumption, comorbidities and HOMA-IR. However, after full adjustment, also including functional independence degree, BMI and LTPA, only the association of lower 25(OH)D with lower free testosterone was still significant.
Conclusion
In men with SCI, 25(OH)D correlates with total and free testosterone and exhibits an independent linear association with free testosterone. Regardless of this independent link, hypovitaminosis D and androgen deficiency are markers of poor health, sharing common risk factors to take into account in the rehabilitative approach to patients with SCI.
Keywords: Androgen deficiency, Hypogonadism, Hypovitaminosis D, Paraplegia, Tetraplegia
Introduction
Vitamin D, beside its well known role in bone health and calcium metabolism,1 extends its actions well beyond calcium homeostasis. An increasing body of observational data has linked low serum levels of 25-hydroxyvitamin D (25(OH)D) to an increased risk of a variety of chronic diseases, including cancer,2 diabetes,3,4 hypertension,5 autoimmune and musculoskeletal diseases,6 depression7 and cardiovascular diseases.6,8 Biological actions of vitamin D are mediated by the vitamin D receptor (VDR), which is almost ubiquitously expressed in human cells, making biologically plausible a wide spectrum of pleiotropic effects of vitamin D.
The expression of VDR and vitamin D metabolizing enzymes in the male reproductive tract has suggested a biological link between vitamin D and male reproductive hormones.9 An independent association between 25(OH)D and total testosterone levels has been reported in two studies.10,11 However, in the European Male Aging Study (EMAS), a large cross-sectional study among 3369 community-dwelling men, the linear association was lost after adjusting for health and lifestyle factors, although a weak association persisted between vitamin D deficiency and both secondary and compensated primary hypogonadism.12 Actually, low vitamin D and androgen deficiency might represent markers of a poor health status, sharing common underlying aetiologies. If an independent association between vitamin D deficiency and low testosterone really exists, it should be demonstrable, regardless of confounders, in different populations, including men who exhibit a high prevalence of risk factors for both hypovitaminosis D and biochemical androgen deficiency. In this view, men with spinal cord injury (SCI) could represent a suitable clinical model of study.
A higher prevalence of vitamin D deficiency has been reported in patients with SCI than in able-bodied population.13 In these subjects a combination of poor sunlight exposure, inadequate diet, comorbidities and obesity, highly prevalent after SCI, along with the intake of medications that induce hepatic microsomal enzymes, accelerating vitamin D metabolism, could be involved in the pathogenesis of the hypovitaminosis D.14 A decline in serum testosterone levels in men after SCI has been also reported in the last decade.15–20 The very high prevalence of biochemical testosterone deficiency (up to 83%) in men with acute SCI15 is not surprising, considering the effects of acute physical distress and systemic illness on testosterone levels. Nevertheless, higher rates of low serum testosterone have been also reported in men with chronic SCI.16–20 Although the pathophysiology of the high prevalence of biochemical androgen deficiency in men with chronic SCI has not yet been clarified, we recently demonstrated that modifiable life-style related risk factors, such as poor leisure time physical activity (LTPA) and high body mass index (BMI), could represent strong independent predictors of low testosterone in these subjects.19 Interestingly, poor physical activity and overweight could also contribute to the hypovitaminosis D: not only physical inactivity favours a poor sunlight exposure, but also it results in low energy expenditure, thus leading to adiposity excess, which in turn decreases bioavailability of vitamin D.21 However, in a recent report,22 no correlation was found between 25(OH)D and testosterone levels in 29 men with chronic SCI, while a significant correlation was found in 17 age matched, able-bodied controls.
In this study we analyzed the relationship between 25(OH)D and testosterone levels in a larger series of men with chronic SCI, as an association is expected in this population, that exhibits a high prevalence of both hypovitaminosis D and biochemical androgen deficiency, as well as a wide spectrum of risk factors for both of these conditions.
Methods
Study population
Forty-nine male patients, aged 47.5 ± 17.3 years, consecutively admitted to a rehabilitation program at the San Raffaele Institute of Sulmona because of traumatic SCI, were included in the study. All patients had a documented history of neurologically stable SCI for more than 1 year. No patient received testosterone or vitamin D replacement therapy. Sixteen patients took gabapentin for neuropathic pain relief. Coexisting chronic illness were registered: they included heart diseases, hypertension, diabetes and depression. No patient had acute illness hindering the rehabilitative program. All participants were requested to sign a written informed consent and the study was approved by the local ethics committee.
Clinical examination
Patients underwent detailed neurological examination according to the guidelines of the International Standards for Neurological Examination and Functional Classification of Spinal Cord Injury23 and the American Spinal Injury Association (ASIA) protocol was used to define both level and completeness of the lesion.23 According to the ASIA impairment scale, patients with complete lesion and no sensory or motor function preserved in the lowest sacral segment were categorized as A, whereas patients with incomplete lesion were categorized as B–D. Category B indicated sensory incomplete lesion (including segments S4–S5); category C indicated sensory and motor incomplete lesion where more than half of the 10 pairs of key muscles have strength of less than 3 on a scale of 0–5; category D indicated sensory and motor incomplete lesion with at least half of the key muscles having strength greater than or equal to 3.
Functional independence degree was assessed at admission by the Barthel Index. It is a 10-item instrument measuring disability in terms of the level of functional independence obtainable by a patient in personal activities of daily living (ADL), giving a final score that ranges from 0 (totally dependent) to 100 (totally independent).24 Because of its reliability and validity, the Barthel index represents a standard measure of disability in different categories of patients, including spinal cord-injured subjects.25
Body weight was taken with patients wearing light clothing, using a professional mechanical chair scale (Wunder SA BI Srl, Monza, Italy). After placing the patient in a bed, his legs were straightened, his head was positioned in the Frankfurt plane, and his feet were placed in dorsal flexion. Height was determined by an elastic tape, measuring segmentally the heel to knee, the knee to hip and the hip to head distances. The body mass index (BMI) was calculated in kilograms per square meter (kg/m2).
Assessment of Leisure Time Physical Activity
Leisure Time Physical Activity (LTPA) includes physical exertion-related activities, that people choose to do in their free time, and in case of patients with SCI it includes walking or wheeling and certain sports played in a gym. LTPA was quantified using the LTPA Questionnaire for people with Spinal Cord Injury (LTPAQ-SCI).26 This is a SCI-specific measure of minutes of mild, moderate, and heavy intensity LTPA performed over the previous 7 days, according to the physical activity guidelines for people with SCI.27 The questionnaire takes less than 5 minutes to complete and can be self-administered. Participants used an intensity classification chart to distinguish between mild, moderate, and heavy intensity LTPA, based on perceived psychophysical effort. For each intensity level, participants recalled the number of days, over the past 7 days, that they performed LTPA at each intensity. Next, they recalled how many minutes/day they usually spent doing LTPA at that intensity. The scale was scored by calculating the total number of weekly minutes of activity performed at each intensity (number of days of activity × number of minutes of activity). Total weekly minutes were divided by 60 to obtain the number of hours of activity performed over the past week. Due to the high correlation of total LTPAQ-SCI scores with mild, moderate and heavy sub-scores,19 only total LTPAQ-SCI scores were used for analyses
Hormones, biochemistry and haematology
A single fasting morning venous blood sample was obtained from each subject between 8:00 and 9:00 a.m. Serum 25(OH)D levels were determined using a chemiluminescent immunoassay (LIAISON®, DiaSorin, Saluggia, VC, Italy) with intra- and inter-assay coefficients of variation (CV) of 4.5% and 8.5%, respectively. 25(OH)D levels were classified into sufficient(≥30 ng/mL), sub-optimal (20–29.9 ng/mL) and deficient (<20 ng/mL), according to previously recommended cut-off points;28 in particular, values <20 ng/ml (or <50 nmol/l) were considered inadequate or not sufficient.29 Serum levels of total testosterone were measured by chemiluminescence immunoassay, using kits from Ortho-Clinical Diagnostics (Johnson & Johnson, New Brunswick, NJ, USA). The lower detection limit for testosterone quantitation was 0.03 nmol/L; the within- and between-assay CV of testosterone measurements were 2.5% and 4.9%, respectively. A total testosterone level below 300 ng/dL (<10.4 nmol/L) indicated a biochemical androgen deficiency, according to the Endocrine Society guidelines.30 Sex hormone binding globulin (SHBG), luteinizing hormone (LH), parathyroid hormone (PTH) and insulin levels were assessed by chemiluminescence immunoassay, using kits from Medical Systems (Genova, Italy). Free testosterone levels were derived from total hormone, SHBG, and albumin concentrations as previously described,31 using a web-based calculator (http://www.issam.ch/freetesto.htm). All the other biochemical/haematological measurements were performed using standard methods and commercial kits (Instrumentation Laboratory Company, Lexington, MA, USA). Insulin resistance was assessed using the homeostatic model assessment of insulin resistance (HOMA-IR), according to the formula: insulin (mU/L) × glucose (m/dL)/405.32
Statistical analysis
Statistical analysis was performed using the R statistical software (version 2.15.2, 2012, The R Foundation for Statistical Computing, Vienna, Austria). After assessing the distribution of data with Shapiro–Wilk test, Wilcoxon rank-sum test and unpaired two-sided Student's t test were used, as appropriate, for data analysis. Proportional differences were assessed by the χ2 test or the Fisher exact test as appropriate. Correlations were evaluated using the Spearman's or Pearson's correlation test as appropriate. The association of 25(OH)D levels with total and free testosterone levels was evaluated using separate linear regressions analyses of log-transformed values. Adjustments were made for age, smoking, alcohol consumption, coexisting illness, HOMA-IR, functional independence degree, BMI and weekly LTPA. Multicollinearity was assessed using the variance inflation factors (VIFs).
Results
Cohort characteristics and 25(OH)D correlates
A deficiency of 25(OH)D (<20 ng/mL) was observed in 36 patients (73.5% of the study population): in this group 25(OH)D ranged from 4.12 to 19.1 ng/mL. Eleven men (22.4% of the study population) exhibited sub-optimal 25(OH)D levels, ranging from 20.5 to 24.9 ng/mL. Only two men exhibited 25(OH)D levels >30 ng/mL.
Table 1 shows the characteristics of the study population according to 25(OH)D status. Patients with 25(OH)D deficiency exhibited significantly lower total and free testosterone levels, higher PTH, insulin, HOMA-IR and triglycerides values; they also exhibited a lower functional independence degree and were engaged in a significantly poorer weekly LTPA.
Table 1.
Characteristics of the study population categorized by vitamin D status
| 25(OH)D (ng/mL) |
|||
|---|---|---|---|
| Characteristic | <20 (n = 36) | ≥20 (n = 13) | P value |
| Age (yr) | 47.0 [20.0–78.0] | 49.0 [33.0–76.0] | 0.7 |
| Current smokers–no. (%) | 10 (27.8) | 8 (61.5) | 0.06* |
| Alcohol intake ≥1 day/week–no. (%) | 25 (69.4) | 11 (84.6) | 0.5* |
| Body mass index (Kg/m2) | 24.8 ± 4.8 | 23.6 ± 4.2 | 0.4 |
| 25(OH)D (ng/mL) | 11.8 ± 4.2 | 24.4 ± 4.0 | <0.0001 |
| Total testosterone (ng/dL) | 328.0 ± 170.0 | 496.0 ± 132.0 | 0.002 |
| Free testosterone (pg/mL) | 87.1 ± 42.8 | 151.2 ± 46.1 | <0.0001 |
| LH (U/L) | 4.3 [0.7–23.8] | 3.6 [1.1–7.8] | 0.4 |
| SHBG (nmol/L) | 18.1 [2.8–64.0] | 12.5 [5.7–26.3] | 0.4 |
| PTH (pg/mL) | 35.1 [7.5–116.6] | 18.7 [6.0–41.2] | 0.002 |
| Calcium (mg/dL) | 9.4 ± 0.5 | 9.5 ± 0.3 | 0.4 |
| Phosphorus (mg/dL) | 3.9 ± 0.6 | 3.9 ± 0.6 | 0.8 |
| Glucose (mg/dL) | 88.0 [56.0–145.0] | 86.0 [72.0–101.0] | 0.9 |
| Insulin (mU/L) | 8.5 [1.9–30.7] | 5.3 [3.0–9.6] | 0.007 |
| HOMA-IR | 2.0 [0.3–8.1] | 1.0 [0.6–2.1] | 0.004 |
| LDL-c (mg/dL) | 101.2 [53.6–205.6] | 108.6 [68.4–153.2] | 0.5 |
| HDL-c (mg/dL) | 38.0 ± 9.8 | 42.8 ± 6.5 | 0.08 |
| Triglycerides (mg/dL) | 122.0 [42.0–358.0] | 107.0 [52.0–276.0] | 0.03 |
| AST (U/L) | 17.0 [8.0–69.0] | 16.0 [9.0–28.0] | 0.9 |
| ALT (U/L) | 17.0 [5.0–78.0] | 16.0 [9.0–33.0] | 0.7 |
| γ-GT (U/L) | 24.5 [13.0–55.0] | 23.0 [12.0–80.0] | 0.3 |
| Level of lesion–no (%) | |||
| Cervical spine | 19 (52.8) | 3 (23.0) | 0.1# |
| Thoracolumbar spine | 17 (47.2) | 10 (77.0) | 0.1* |
| Lesion completeness–no (%) | |||
| ASIA score A (complete) | 17 (47.0) | 8 (61.5) | 0.6* |
| ASIA score B-D (incomplete) | 19 (53.0) | 5 (38.5) | 0.6* |
| Barthel index (functional independence degree) | 43.0 [3.0–88.0] | 58.0 [12.0–83.0] | 0.03 |
| LTPA (hours/week) | 7.3 ± 4.4 | 12.3 ± 6.0 | 0.003 |
| Coexisting illness–no. (%) | 24 (66.7) | 7 (53.8) | 0.6* |
| CRP>5 mg/L–no. (%) | 12 (33.3) | 1 (7.7) | 0.1# |
| Gabapentin intake–no. (%) | 11 (30.5) | 5 (38.5) | 0.8* |
Data were expressed as mean ± standard deviation when normally distributed, as median [min-max] for parameters with non-normal distribution: unpaired two-sided Student's t test and Wilcoxon rank-sum test were applied to detect differences, according to normal or non-normal distribution of continuous variables. Data were expressed as percentages when categorical: proportional differences were assessed by the χ2 test (*) or the Fisher exact test (#) as appropriate.
25(OH)D = 25-hydroxyvitamin D; lH = Luteinizing hormone; SHBG = sex hormone binding globulin; PTH = parathyroid hormone; HOMA-IR = homeostatic model assessment of insulin resistance; LDL-c = low-density lipoprotein cholesterol; HDL-c = high-density lipoprotein cholesterol; AST = aspartate aminotransferase; ALT = alanine aminotransferase; γ-GT, gamma-glutamyl transpeptidase; ASIA = american spinal injury association; LTPA = leisure time physical activity; CRP = C-reactive protein. Coexisting illness included: heart diseases, hypertension, diabetes and depression.
To convert the values for 25(OH)D to nmol/L, multiply by 2.5; to convert the values for total testosterone to nmol/L, multiply by 0.03467; to convert the values for free testosterone to pmol/L, multiply by 3.467.
Relationship of 25(OH)D with testosterone levels
The levels of 25(OH)D were strongly correlated with free testosterone (r = 0.60, P < 0.0001; Figure 1). Other significant correlates were total testosterone (r = 0.42, P = 0.002; Figure 1), PTH (r = –0.49, P = 0.0003), functional independence degree (r = 0.36; P = 0.01) and weekly LTPA (r = 0.41, P = 0.003).
Figure 1.
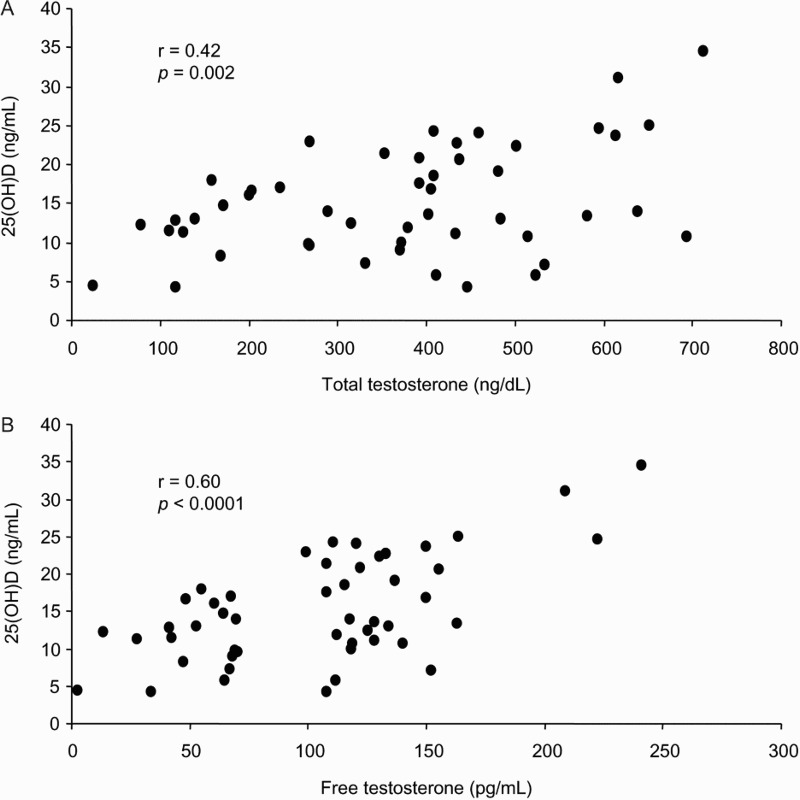
Correlations of 25(OH)D with total testosterone (A) and free testosterone (B). To convert the values for 25(OH)D to nmol/L, multiply by 2.5; to convert the values for total testosterone to nmol/L, multiply by 0.03467; to convert the values for free testosterone to pmol/L, multiply by 3.467.
A biochemical androgen deficiency (total testosterone <300 ng/dL) was observed in 17 patients (34.7%); it was exhibited by 16 of 36 patients with 25(OH)D deficiency (44.4%) but only by 1 of 13 patients (7.7%) with 25(OH)D levels ≥ 20 ng/mL (p = 0.02).
The association of 25(OH)D with total and free testosterone was further explored with linear regression models (Table 2). Lower levels of 25(OH)D were associated with both lower total and free testosterone levels in unadjusted models. These associations persisted following adjustment for age, smoking, alcohol consumption, coexisting illness and HOMA-IR. However, after full adjustment, also including functional independence degree, BMI and weekly LTPA, only the independent association of lower 25(OH)D with lower free testosterone was still significant. Although total and free testosterone were significantly correlated with HOMA-IR, BMI and weekly LTPA (not shown), a multicollinearity effect was ruled out, because the VIFs for independent variables in the regression analyses were lower than 2.6.
Table 2.
Association between 25-hydroxyvitamin D and testosterone levels: linear regressions
| Model I | Model II | Model III | |
|---|---|---|---|
| Total testosterone | 0.30 (0.09, 0.50) | 0.28 (0.02, 0.53) | 0.29 (–0.04, 0.62) |
| P = 0.005 | P = 0.03 | P = 0.08 | |
| Free testosterone | 0.35 (0.18, 0.52) | 0.37 (0.17, 0.58) | 0.42 (0.17, 0.67) |
| P = 0.0001 | P = 0.0007 | P = 0.001 |
Values are β-coefficients (95% CI). Model I, unadjusted; model II, adjusted for age, smoking, alcohol consumption, coexisting illness, and homeostatic model assessment of insulin resistance; model III, adjusted for model II+functional independence degree (Barthel index), body mass index and weekly leisure time physical activity.
Discussion
While an association between 25(OH)D and testosterone levels has been reported in the general population,10–12 their relationship had not been investigated in men with chronic SCI, until a recent report published while this manuscript was in preparation.22 In that study a correlation between 25(OH)D and calculated free testosterone levels was found in 17 controls, but not in 29 men with chronic SCI.
On the contrary, in the present study, 25(OH)D levels were correlated with total and free testosterone levels in men with SCI. In those with 25(OH)D deficiency (73.5%), a biochemical androgen deficiency was ∼6 fold more prevalent than in those with 25(OH)D ≥ 20 ng/mL (44.4% vs 7.7%). This would be expected, as vitamin D and androgen deficiency share some risk factors, including physical inactivity, overweight and coexisting illness, which are highly prevalent in this population. Nevertheless, the significant linear association between 25(OH)D and free testosterone levels persisted after full adjustment for confounders. Actually, although residual confounders cannot be ruled out with certainty, this study indicates an association between 25(OH)D and free testosterone independent of major determinants of 25(OH)D/testosterone, including BMI and physical activity (model III, in Table 2). These data conflict with those from the above mentioned recent report where no correlation was found between 25(OH)D and total and free testosterone.22 Although discrepancy could be explained by differences in the size and characteristics of the study population, extremely low reference values for calculated free testosterone were indicated in that study, so that all values reported both in men with SCI and in control group were in the range of overt hypogonadism according to shared cut-off.30,33,34
An independent linear association between 25(OH)D and testosterone had been previously reported in able-bodied men by two studies,10,11 but not by the EMAS, where it was lost after multivariate adjustment for health and lifestyle factors.12 The evidence for an independent association between 25(OH)D and testosterone is in keeping with experimental/basic findings. Both 25(OH)D and testosterone deficiency might reflect a Leydig cell dysfunction. Leydig cells express CYP2R1 gene, encoding the main enzyme involved in 25-hydroxilation of vitamin D.35 Furthermore, bilateral orchidectomy produced a significant decrease in 25(OH)D levels, not reverted by androgen replacement therapy.36 On the other hand, some evidence also suggests a role for vitamin D in testosterone biosynthesis. VDR-knockout mice developed hypergonadotropic hypogonadism.37 Furthermore, in vitro exposure of human Leydig cell cultures to 1,25(OH)D significantly increased testosterone synthesis, by modifying the expression profiles of steroidogenesis genes.38 Obviously, due to its transversal design, the present study does not help to clarify the nature of this association: low vitamin D as a reflection of testicular dysfunction or playing a causal role in androgen deficiency.
Regardless of the independent link between vitamin D and free testosterone, the present study reinforces the notion that low vitamin D and androgen deficiency are markers of poor health, sharing common risk factors. In the regression analysis, when BMI and physical activity were included, the association of vitamin D with total testosterone was lost and that with free testosterone was attenuated. Both BMI and physical activity, measured as LTPA in men with chronic SCI, are life style-related modifiable risk factors. This could be relevant to clinical practice: in the rehabilitative approach to patients with SCI, a great effort should be made in inducing modifications of these life style-related risk factors, shared by both hypovitaminosis D and androgen deficiency.
Our study suffers from some limitations. Firstly, the limited sample numerousness, which, however, was enough to demonstrate significant and independent associations, likely due to the high prevalence of both vitamin D and androgen deficiency in this populations. Another limitation is that total testosterone was measured by an immunoassay, which has lower accuracy than mass spectrometry, which, however, is rarely used in clinical settings.
Conclusion
An evidence is here provided that, in men with SCI, 25(OH)D correlates with total testosterone and free testosterone and exhibits an independent linear association with free testosterone. Regardless of this independent link, hypovitaminosis D and androgen deficiency share life style-related risk factors to take into account in the rehabilitative approach to patients with SCI.
Disclaimer statements
Contributors AB designed the research, conducted the study, analyzed data and interpreted results, performed statistical analysis and wrote the manuscript; MRCV analyzed data; GF and SF revised the article critically and approved its final version; FF designed the research, analyzed data and interpreted results, wrote the manuscript, revised the article critically and approved its final version.
Funding None.
Conflicts of interest The authors declare no potential conflict-of-interest.
Ethics approval The study was approved by the ethics committee of ASL1 Avezzano-Sulmona-L'Aquila.
Acknowledgments
This work was supported by Ministero dell'Università e della Ricerca (MIUR), Italy.
References
- 1.Lips P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 2001;22(4):477–501. doi: 10.1210/edrv.22.4.0437 [DOI] [PubMed] [Google Scholar]
- 2.Pilz S, Dobnig H, Winklhofer-Roob B, Riedmüller G, Fischer JE, Seelhorst U, et al. Low serum levels of 25-hydroxyvitamin D predict fatal cancer in patients referred to coronary angiography. Cancer Epidemiol Biomarkers Prev 2008;17(5):1228–33. doi: 10.1158/1055-9965.EPI-08-0002 [DOI] [PubMed] [Google Scholar]
- 3.Pittas AG, Lau J, Hu FB, Dawson-Hughes B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab 2007;92(6):2017–29. doi: 10.1210/jc.2007-0298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Forouhi NG, Luan J, Cooper A, Boucher BJ, Wareham NJ. Baseline serum 25-hydroxy vitamin D is predictive of future glycemic status and insulin resistance: the Medical Research Council Ely Prospective Study 1990–2000. Diabetes 2008;57(10):2619–25. doi: 10.2337/db08-0593 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pilz S, Tomaschitz A, Ritz E, Pieber TR. Vitamin D status and arterial hypertension: a systematic review. Nat Rev Cardiol 2009;6(10):621–30. doi: 10.1038/nrcardio.2009.135 [DOI] [PubMed] [Google Scholar]
- 6.Holick MF. Vitamin D deficiency. N Engl J Med 2007;357(3):266–81. doi: 10.1056/NEJMra070553 [DOI] [PubMed] [Google Scholar]
- 7.Lee DM, Tajar A, O'neill TW, O'connor DB, Bartfai G, Boonen S, et al. ; EMAS study group. Lower vitamin D levels are associated with depression among community-dwelling European men. J Psychopharmacol 2011;25(10):1320–8. doi: 10.1177/0269881110379287 [DOI] [PubMed] [Google Scholar]
- 8.Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, et al. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008;117(4):503–11. doi: 10.1161/CIRCULATIONAHA.107.706127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Blomberg Jensen M, Nielsen JE, Jørgensen A, Rajpert-De Meyts E, Kristensen DM, Jørgensen N, et al. Vitamin D receptor and vitamin D metabolizing enzymes are expressed in the human male reproductive tract. Hum Reprod 2010;25(5):1303–11. doi: 10.1093/humrep/deq024 [DOI] [PubMed] [Google Scholar]
- 10.Wehr E, Pilz S, Boehm BO, März W, Obermayer-Pietsch B. Association of vitamin D status with serum androgen levels in men. Clin Endocrinol (Oxf) 2010;73(2):243–8. [DOI] [PubMed] [Google Scholar]
- 11.Nimptsch K, Platz EA, Willett WC, Giovannucci E. Association between plasma 25-OH vitamin D and testosterone levels in men. Clin Endocrinol (Oxf) 2012;77(1):106–12. doi: 10.1111/j.1365-2265.2012.04332.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee DM, Tajar A, Pye SR, Boonen S, Vanderschueren D, Bouillon R, et al. ; EMAS study group. Association of hypogonadism with vitamin D status: the European Male Ageing Study. Eur J Endocrinol 2012;166(1):77–85. doi: 10.1530/EJE-11-0743 [DOI] [PubMed] [Google Scholar]
- 13.Maïmoun L, Fattal C, Sultan C. Bone remodeling and calcium homeostasis in patients with spinal cord injury: a review. Metabolism 2011;60(12):1655–63. doi: 10.1016/j.metabol.2011.04.005 [DOI] [PubMed] [Google Scholar]
- 14.Bauman WA, Zhong YG, Schwartz E. Vitamin D deficiency in veterans with chronic spinal cord injury. Metabolism 1995;44(12):1612–6. doi: 10.1016/0026-0495(95)90083-7 [DOI] [PubMed] [Google Scholar]
- 15.Schopp LH, Clark M, Mazurek MO, Hagglund KJ, Acuff ME, Sherman AK et al. Testosterone levels among men with spinal cord injury admitted to inpatient rehabilitation. Am J Phys Med Rehabil 2006;85(8):678–84. doi: 10.1097/01.phm.0000228617.94079.4a [DOI] [PubMed] [Google Scholar]
- 16.Kostovski E, Iversen PO, Birkeland K, Torjesen PA, Hjeltnes N. Decreased levels of testosterone and gonadotrophins in men with long-standing tetraplegia. Spinal Cord 2008;46(8):559–64. doi: 10.1038/sc.2008.3 [DOI] [PubMed] [Google Scholar]
- 17.Durga A, Sepahpanah F, Regozzi M, Hastings J, Crane DA. Prevalence of testosterone deficiency after spinal cord injury. PM R 2011;3(10):929–32. doi: 10.1016/j.pmrj.2011.07.008 [DOI] [PubMed] [Google Scholar]
- 18.Bauman WA, Fountaine MF, Spungen AM. Age-related prevalence of low testosterone in men with spinal cord injury. J Spinal Cord Med 2014;37(1):32–9. doi: 10.1179/2045772313Y.0000000122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Barbonetti A, Vassallo MRC, Pacca F, Cavallo F, Costanzo M, Felzani G, et al. Correlates of low testosterone in men with chronic spinal cord injury. Andrology 2014;2(5):721–28. doi: 10.1111/j.2047-2927.2014.00235.x [DOI] [PubMed] [Google Scholar]
- 20.Barbonetti A, Caterina Vassallo MR, Cotugno M, Felzani G, Francavilla S, et al. Low testosterone and non-alcoholic fatty liver disease: Evidence for their independent association in men with chronic spinal cord injury. J Spinal Cord Med 2015. DOI: 10.1179/2045772314Y.0000000288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr 2000;72(3):690–3. [DOI] [PubMed] [Google Scholar]
- 22.Gaspar AP, Brandão CM, Lazaretti-Castro M. Bone mass and hormone analysis in patients with spinal cord injury: evidence for a gonadal axis disruption. J Clin Endocrinol Metab 2014;99(12):4649–55. doi: 10.1210/jc.2014-2165 [DOI] [PubMed] [Google Scholar]
- 23.Maynard FM Jr, Bracken MB, Creasey G, Ditunno JF Jr, Donovan WH, Ducker TB, et al. International standards for neurological and functional classification of spinal cord injury. Spinal Cord 1997;35(5):266–74. doi: 10.1038/sj.sc.3100432 [DOI] [PubMed] [Google Scholar]
- 24.Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J 1965;14:61–5. [PubMed] [Google Scholar]
- 25.Barbonetti A, Cavallo F, Felzani G, Francavilla S, Francavilla F. Erectile dysfunction is the main determinant of psychological distress in men with spinal cord injury. J Sex Med 2012;9(3):830–6. doi: 10.1111/j.1743-6109.2011.02599.x [DOI] [PubMed] [Google Scholar]
- 26.Martin Ginis KA, Phang SH, Latimer AE, Arbour-Nicitopoulos KP. Reliability and validity tests of the leisure time physical activity questionnaire for people with spinal cord injury. Arch Phys Med Rehabil 2012;93(4):677–82. doi: 10.1016/j.apmr.2011.11.005 [DOI] [PubMed] [Google Scholar]
- 27.Ginis KA, Hicks AL, Latimer AE, Warburton DE, Bourne C, Ditor DS, et al. The development of evidence-informed physical activity guidelines for adults with spinal cord injury. Spinal Cord 2011;49(11):1088–96. doi: 10.1038/sc.2011.63 [DOI] [PubMed] [Google Scholar]
- 28.Holick MF, Gordon CM. The Hormone Foundation's: patient guide to vitamin deficiency. J Clin Endocrinol Metab 2011;96(7):1–2. doi: 10.1210/jcem.96.7.zeg33a [DOI] [PubMed] [Google Scholar]
- 29.Ross A, Taylor C, Yaktine A, Del Valle H. Dietary Reference Intakes for Calcium and Vitamin D. Institute of Medicine Report Washington, DC: The National Academies Press; 2011. [PubMed] [Google Scholar]
- 30.Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS et al. Task Force, Endocrine Society. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2010;95(6):2536–59. doi: 10.1210/jc.2009-2354 [DOI] [PubMed] [Google Scholar]
- 31.Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab 1999;84(10):3666–72. doi: 10.1210/jcem.84.10.6079 [DOI] [PubMed] [Google Scholar]
- 32.Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28(7):412–9. doi: 10.1007/BF00280883 [DOI] [PubMed] [Google Scholar]
- 33.Wu FC, Tajar A, Beynon JM, Pye SR, Silman AJ, Finn JD, et al. ; EMAS Group. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med 2010;363(2):123–35. doi: 10.1056/NEJMoa0911101 [DOI] [PubMed] [Google Scholar]
- 34.Bhasin S, Pencina M, Jasuja GK, Travison TG, Coviello A, Orwoll E, et al. Reference ranges for testosterone in men generated using liquid chromatography tandem mass spectrometry in a community-based sample of healthy non obese young men in the Framingham Heart Study and applied to three geographically distinct cohorts. J Clin Endocrinol Metab 2011;96(8):2430–9. doi: 10.1210/jc.2010-3012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cheng JB, Levine MA, Bell NH, Mangelsdorf DJ, Russell DW. Genetic evidence that the human CYP2R1 enzyme is a key vitamin D 25-hydroxylase. Proc Natl Acad Sci USA 2004;101(20):7711–5. doi: 10.1073/pnas.0402490101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Foresta C, Selice R, Di Mambro A, Strapazzon G. Testiculopathy and vitamin D insufficiency. Lancet 2010;376(9749):1301. doi: 10.1016/S0140-6736(10)61916-2 [DOI] [PubMed] [Google Scholar]
- 37.Bouillon R, Carmeliet G, Verlinden L, van Etten E, Verstuyf A, Luderer HF, et al. Vitamin D and human health: lessons from vitamin D receptor null mice. Endocr Rev 2008;29(6):726–76. doi: 10.1210/er.2008-0004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hofer D, Münzker J, Schwetz V, Ulbing M, Hutz K, Stiegler P, et al. Testicular synthesis and vitamin D action. J Clin Endocrinol Metab 2014;99(10):3766–73. doi: 10.1210/jc.2014-1690 [DOI] [PubMed] [Google Scholar]