
Figure 1. Surgical extraction of hDRG using ventral approach.
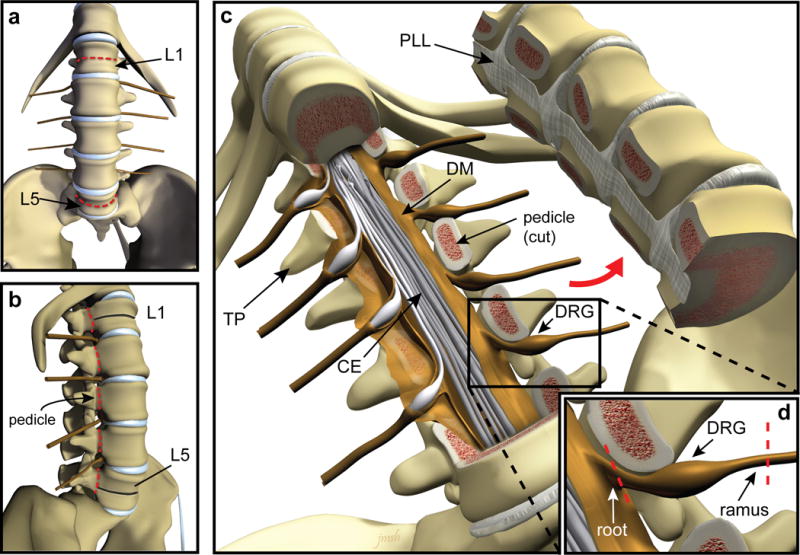
(a–b) Illustration depicting the ventral (a) and lateral (b) views of the spinal column with lumbar vertebral bodies L1 and L5 indicated by arrows. Red dashed lines indicate the location of bone transection. After the spinal column is visualized, lumbar vertebrae can be correctly identified by counting up from L5, which is located directly above the sacrum (a,b). Using a straight osteotome and surgical mallet, the L1 and L5 vertebral bodies are transected, stopping at the spinal canal (red dashed lines in panel a, black lines indicate transected bone in panel b). Using a curved osteotome and mallet or autopsy saw, the pedicles of each vertebrae are transected bilaterally between L1 and L5 (red dashed lines in panel b). (c) Illustration showing the anterior portion of the vertebral column removed to expose the spinal canal where the cauda equina and DRG are located (TP: transverse process, CE: cauda equina, PLL: posterior longitudinal ligament, DM: dura mater, DRG: dorsal root ganglion). (d) Each DRG is dissected away from surrounding bone and connective tissue and the nerve roots and rami are cut to completely free each ganglion (red dashed lines). CAUTION: Donor consent for tissue donation for research purposes must be obtained by OPO or transplant service prior to tissue extraction.